Small Intestinal Bacterial Overgrowth (SIBO)
Deep-Dive Articles
SIBO is a big topic, and most people land here mid-journey — you’ve already heard of it and want to dig deeper. The eight articles below each focus on one part of the puzzle: how it’s diagnosed, how it’s treated, and why it keeps coming back. Start with whichever piece matches where you are right now.
Hydrogen vs. Methane vs. Hydrogen Sulfide
The three SIBO subtypes explained in plain language — why hydrogen gives you diarrhea, methane causes constipation, and hydrogen sulfide produces that sulfurous “rotten-egg” belching. Which gas is driving your symptoms changes which treatment actually works.
Breath Test Guide
Lactulose vs. glucose vs. trio-smart: which test to ask for, how to prep the 24 hours before (the prep diet matters more than people realize), how to read the curves, and why false negatives are so common.
Low-FODMAP Diet
The complete food list, the three phases (elimination, reintroduction, personalization), and — importantly — why you should not stay on it long-term. A symptom-control tool, not a cure.
Elemental Diet
The 2-week liquid-only protocol that starves bacteria by absorbing in the first foot of small intestine. Commercial vs. homemade, cost, palatability hacks, and realistic success rates (80–85% in the Pimentel studies).
Rifaximin Protocols
Xifaxan dosing, why methane needs rifaximin plus neomycin, insurance hurdles, cash-pay options, and what to do when the first course doesn’t work.
Herbal Antimicrobials
Berberine, oregano oil, allicin, neem — the Chedid 2014 Johns Hopkins study showed they match rifaximin head-to-head. Dosing, rotation protocols, and when to pick herbs over prescription antibiotics.
Prokinetics & Relapse Prevention
Why SIBO comes back in ~45% of people within a year — and the migrating motor complex (MMC) you have to restore to stop it. Low-dose naltrexone, prucalopride, low-dose erythromycin, ginger, and the 4-hour meal-spacing rule.
Root Causes
Post-infectious IBS, anti-vinculin antibodies, Ehlers-Danlos/hypermobility, ileocecal valve issues, thyroid slowdown, PPIs, abdominal adhesions — treating SIBO without finding the root cause is why it keeps coming back.
IMO: Methane Overgrowth & Constipation
Why rifaximin alone fails for methane, and the neomycin/lovastatin approaches.
Interactive Visualization The Gut Barrier & Your Microbiome Watch fibre become butyrate and butyrate tighten the gut wall — then starve the microbes and see them eat your mucus layer instead. Launch →
Table of Contents
- Deep-Dive Articles
- Overview
- Epidemiology
- Pathophysiology
- Etiology and Risk Factors
- Clinical Presentation
- Diagnosis
- Treatment
- Complications
- Prognosis
- Prevention
- Recent Research and Advances
- References & Research
- Featured Videos
1. Overview
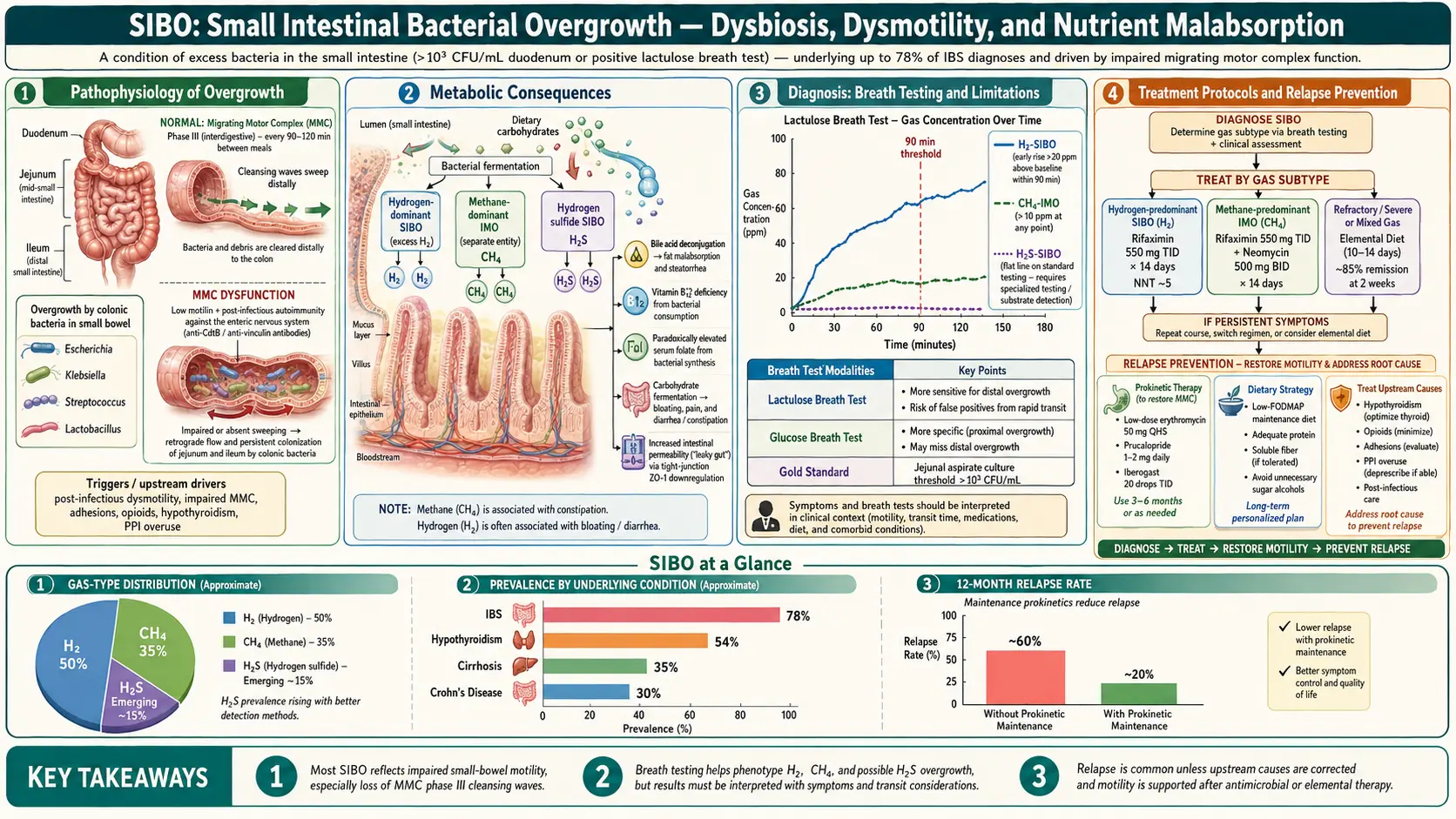
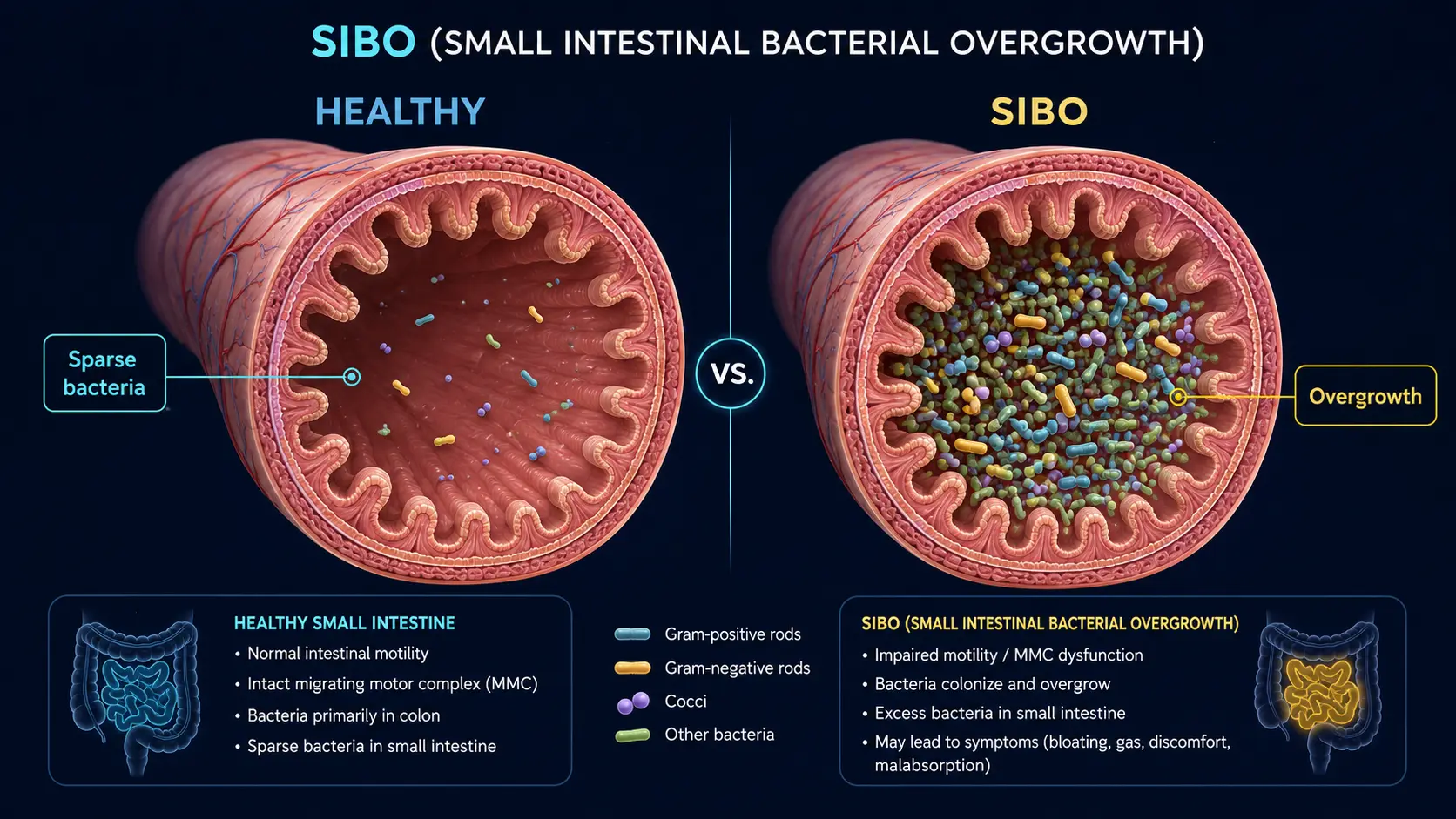
Small intestinal bacterial overgrowth (SIBO) is a clinical condition characterized by an abnormally excessive bacterial colonization of the small intestine, an area of the gastrointestinal tract that normally harbors relatively few microorganisms compared to the colon. Under normal physiological conditions, the small intestine contains fewer than 10^3 to 10^4 colony-forming units per milliliter (CFU/mL) of luminal fluid, primarily consisting of gram-positive aerobes and facultative anaerobes. SIBO is traditionally defined as the presence of ≥10^5 CFU/mL in a jejunal aspirate, though more recent consensus recommendations have proposed a lower threshold of ≥10^3 CFU/mL in the setting of colonic-type bacteria (anaerobes, gram-negative organisms) to improve diagnostic sensitivity.
The overgrowth of bacteria in the small intestine disrupts normal digestive and absorptive functions through multiple mechanisms, including deconjugation of bile salts (leading to fat malabsorption), competitive consumption of nutrients (particularly vitamin B12 and iron), damage to the intestinal epithelium (causing increased intestinal permeability, or "leaky gut"), and fermentation of undigested carbohydrates (producing hydrogen, methane, and hydrogen sulfide gases that cause bloating, distension, and altered bowel habits). SIBO has emerged as a significant clinical entity due to its strong association with irritable bowel syndrome (IBS), with studies suggesting that 30-78% of patients meeting Rome criteria for IBS have underlying SIBO.
SIBO is now recognized to exist in three distinct subtypes based on the predominant gas produced during fermentation: hydrogen-dominant SIBO (associated with diarrhea-predominant symptoms), methane-dominant SIBO (now termed intestinal methanogen overgrowth, or IMO, associated with constipation-predominant symptoms), and hydrogen sulfide-dominant SIBO (recently characterized, associated with diarrhea and sulfurous eructation). This subtyping has important therapeutic implications, as different gas-producing organisms respond to different antimicrobial strategies.
2. Epidemiology
The true prevalence of SIBO in the general population is difficult to determine due to variability in diagnostic methods and thresholds, but estimates range from 0.5-6% in healthy, asymptomatic individuals to much higher rates in specific populations. Among patients with irritable bowel syndrome (IBS), SIBO prevalence ranges from 30-78% depending on the diagnostic modality used, with breath testing consistently showing higher rates than jejunal aspirate culture. SIBO disproportionately affects the elderly, with prevalence increasing to 15-33% in individuals over age 60, attributed to age-related declines in gastric acid production, intestinal motility, and immune function.
Specific high-risk populations demonstrate markedly elevated SIBO prevalence: chronic pancreatitis (30-40%), liver cirrhosis (30-73%), celiac disease (9-55%), Crohn's disease (18-30%), diabetes mellitus (8-44%), systemic sclerosis/scleroderma (43-55%), chronic kidney disease (27-36%), hypothyroidism (54%), Parkinson's disease (25-55%), morbid obesity (17-41%), and patients on chronic proton pump inhibitor (PPI) therapy (50%). Post-surgical populations are also at high risk, particularly after Roux-en-Y gastric bypass (40-52%), ileocecal valve resection, and any surgery creating blind loops or altered intestinal anatomy.
Women are affected more frequently than men, with a female-to-male ratio of approximately 2-3:1, which parallels the sex distribution of IBS. The economic burden of SIBO is substantial, with patients utilizing significantly more healthcare resources, undergoing more diagnostic testing, and reporting lower quality-of-life scores than matched controls without the condition.
3. Pathophysiology
Normal Protective Mechanisms
The small intestine maintains its low bacterial count through several interconnected defense mechanisms. Disruption of any of these mechanisms predisposes to bacterial overgrowth:
- Gastric acid: Hydrochloric acid (pH 1-3) serves as the first barrier against ingested microorganisms. Conditions that reduce gastric acid (achlorhydria, PPI use, atrophic gastritis) remove this protective barrier.
- Migrating motor complex (MMC): The MMC is a cyclical pattern of gastrointestinal motor activity that occurs during fasting, approximately every 90-120 minutes. Phase III of the MMC produces high-amplitude propulsive contractions that sweep residual bacteria, debris, and undigested material from the small intestine into the colon. This "intestinal housekeeper" function is considered the most important defense mechanism against SIBO.
- Ileocecal valve: This anatomical sphincter prevents retrograde migration of the dense colonic microbiota into the distal ileum. Surgical removal, incompetence, or anatomical disruption of the ileocecal valve significantly increases SIBO risk.
- Intestinal secretory immunoglobulin A (sIgA): sIgA binds to bacteria and prevents adherence to the intestinal epithelium, promoting clearance.
- Bile acids and pancreatic enzymes: Conjugated bile acids have bacteriostatic properties. Pancreatic enzymes, particularly lipase and proteases, contribute to bacterial clearance.
Mechanism of Bacterial Overgrowth
When protective mechanisms fail, colonic-type bacteria (predominantly Escherichia coli, Klebsiella, Proteus, Enterococcus, and obligate anaerobes such as Bacteroides and Clostridium) colonize the small intestine in excessive numbers. The overgrowth bacteria generate pathology through several interconnected mechanisms:
- Carbohydrate fermentation: Bacteria ferment dietary carbohydrates and endogenous mucus glycoproteins, producing hydrogen (H2), carbon dioxide (CO2), and short-chain fatty acids. Hydrogen is subsequently utilized by methanogenic archaea (Methanobrevibacter smithii) to produce methane (CH4), or by sulfate-reducing bacteria (Desulfovibrio spp.) to produce hydrogen sulfide (H2S). These gases cause abdominal bloating, distension, flatulence, and altered motility.
- Bile salt deconjugation: Overgrowth bacteria possess bile salt hydrolase enzymes that deconjugate bile acids prematurely in the small intestine. Deconjugated bile acids are less effective at forming micelles, leading to fat malabsorption, steatorrhea, and malabsorption of fat-soluble vitamins (A, D, E, K). Free bile acids are also directly toxic to enterocytes, causing mucosal inflammation.
- Nutrient competition: Bacteria consume vitamin B12 (cobalamin) before it can be absorbed by the host in the terminal ileum, leading to vitamin B12 deficiency. Paradoxically, overgrowth bacteria produce folate, so folate levels may be normal or elevated. Bacterial consumption of dietary iron contributes to iron deficiency.
Intestinal Permeability and Systemic Effects
SIBO damages the intestinal epithelial barrier through bacterial metabolite-induced inflammation, disruption of tight junction proteins (occludin, claudins, ZO-1), and villous blunting. This increased intestinal permeability ("leaky gut") allows translocation of bacterial endotoxins (lipopolysaccharide, LPS) and food antigens into the systemic circulation, triggering low-grade systemic inflammation, immune activation, and potentially contributing to extraintestinal manifestations including rosacea, restless legs syndrome, fibromyalgia, interstitial cystitis, and non-alcoholic fatty liver disease (NAFLD).
Methane and Motility
Methane gas, produced by the archaeon Methanobrevibacter smithii, is not merely an inert byproduct of fermentation. Research has demonstrated that methane directly slows intestinal transit by 59% in animal models, acting through augmentation of non-propagating ileal contractions and reduction of serotonin-mediated peristalsis. This methane-mediated slowing of motility creates a vicious cycle: slow motility promotes bacterial overgrowth, and the resultant methane production further slows motility, perpetuating the condition. This mechanism explains the strong association between methane-positive breath tests and constipation-predominant IBS (IBS-C).
4. Etiology and Risk Factors
Impaired Motility (Most Common Predisposing Factor)
- Diabetic gastroparesis and enteropathy (autonomic neuropathy affecting MMC)
- Scleroderma/systemic sclerosis (smooth muscle fibrosis and atrophy)
- Hypothyroidism (reduced intestinal motility)
- Chronic opioid use (mu-receptor mediated motility suppression)
- Parkinson's disease (vagal nerve dysfunction and alpha-synuclein deposition in the enteric nervous system)
- Post-infectious gastroparesis (following viral or bacterial gastroenteritis)
- Ehlers-Danlos syndrome (connective tissue disorders affecting intestinal wall compliance)
- Chronic intestinal pseudo-obstruction
Anatomical Abnormalities
- Surgically created blind loops (Billroth II, Roux-en-Y reconstruction)
- Ileocecal valve resection or incompetence
- Small intestinal diverticulosis (stasis within diverticula)
- Strictures (Crohn's disease, radiation enteritis, surgical adhesions)
- Small intestinal obstruction (partial)
- Gastric bypass surgery (Roux-en-Y gastric bypass)
Reduced Gastric Acid
- Proton pump inhibitors (PPIs): Chronic PPI use increases SIBO risk by 2-8 fold by raising gastric pH above 4, eliminating the acid barrier to ingested bacteria
- Atrophic gastritis (including autoimmune/pernicious anemia)
- Vagotomy
- Advanced age (age-related hypochlorhydria)
Immune Deficiency
- IgA deficiency (selective or common variable immunodeficiency)
- HIV/AIDS
- Combined variable immunodeficiency (CVID)
- Chronic immunosuppressive therapy
Other Predisposing Conditions
- Celiac disease (reduced MMC activity even after gluten-free diet)
- Chronic pancreatitis (loss of bacteriostatic pancreatic secretions)
- Liver cirrhosis (portal hypertension, reduced bile acid secretion, impaired motility)
- End-stage renal disease
- Fibromyalgia
- Chronic fatigue syndrome
- Mast cell activation syndrome
5. Clinical Presentation
Gastrointestinal Symptoms
The clinical presentation of SIBO is highly variable and overlaps significantly with IBS and other functional gastrointestinal disorders:
- Bloating and abdominal distension: The most common and often most distressing symptom, typically worsening throughout the day and after meals, particularly those high in fermentable carbohydrates (FODMAPs). Present in 70-85% of SIBO patients.
- Flatulence and excessive gas: Due to bacterial fermentation of carbohydrates in the small intestine, producing hydrogen, methane, and carbon dioxide.
- Abdominal pain and cramping: Diffuse or periumbilical discomfort, often postprandial, caused by gas distension and visceral hypersensitivity.
- Diarrhea: Characteristic of hydrogen-dominant SIBO. Results from bile acid malabsorption, osmotic effects of unabsorbed nutrients, and bacterial enterotoxin-mediated secretion. May be watery, frequent, and foul-smelling.
- Constipation: Characteristic of methane-dominant SIBO (IMO). Methane gas directly inhibits intestinal peristalsis and transit.
- Nausea: Particularly common in severe cases or those with concurrent gastroparesis.
- Steatorrhea: Fatty, malodorous stools due to fat malabsorption from bile acid deconjugation.
- Belching: Particularly sulfurous belching in hydrogen sulfide-dominant SIBO.
Nutritional Deficiencies
- Vitamin B12 deficiency: Bacteria in the proximal small intestine consume vitamin B12 before it reaches its absorption site in the terminal ileum. Can lead to megaloblastic anemia, peripheral neuropathy, and cognitive impairment.
- Iron deficiency: Bacterial consumption and impaired absorption.
- Fat-soluble vitamin deficiencies (A, D, E, K): Due to bile acid deconjugation and fat malabsorption. Can cause night blindness (A), osteoporosis (D), neuropathy (E), and coagulopathy (K).
- Protein malabsorption: In severe cases, hypoalbuminemia from protein-losing enteropathy.
- Elevated folate: Paradoxically, bacterial production of folate may elevate serum levels, which combined with low B12 is a characteristic pattern suggestive of SIBO.
Extraintestinal Manifestations
- Fatigue and brain fog: Among the most common extraintestinal complaints, potentially related to systemic endotoxemia and D-lactic acidosis from bacterial fermentation.
- Rosacea: Strong epidemiological association; SIBO eradication has been shown to improve or resolve rosacea in clinical studies.
- Restless legs syndrome: Association with SIBO, possibly mediated through iron deficiency or systemic inflammation.
- Joint pain and arthralgia: Related to immune complex formation and systemic inflammation.
- Skin conditions: Acne, eczema, and urticaria have been associated with SIBO and intestinal permeability.
- Depression and anxiety: Gut-brain axis disruption through altered neurotransmitter production, vagal signaling, and systemic inflammation.
6. Diagnosis
Small Bowel Aspirate and Culture (Gold Standard)
Jejunal aspirate culture obtained during upper endoscopy (esophagogastroduodenoscopy, EGD) is considered the traditional gold standard for SIBO diagnosis. Fluid is aspirated from the proximal jejunum and cultured quantitatively. A bacterial count of ≥10^5 CFU/mL is the classic diagnostic threshold, though the 2017 North American Consensus recommends ≥10^3 CFU/mL when colonic-type organisms are identified. Limitations include its invasive nature, cost, risk of oropharyngeal contamination during scope passage, inability to sample the distal small intestine, and the fact that up to 30% of SIBO-causing organisms may not grow on standard culture media.
Hydrogen and Methane Breath Testing
Breath testing is the most widely used diagnostic modality due to its non-invasive nature, accessibility, and relatively low cost. The test measures exhaled hydrogen (H2) and methane (CH4) gases produced by bacterial fermentation of an ingested substrate:
- Lactulose breath test (LBT): The patient ingests 10 grams of lactulose (a non-absorbable synthetic disaccharide), and breath samples are collected every 15-20 minutes for 120-180 minutes. A positive test shows a rise in hydrogen of ≥20 ppm above baseline within the first 90 minutes (indicating small intestinal fermentation, as lactulose normally reaches the cecum at 90-120 minutes). Sensitivity: 52-68%; specificity: 44-86%.
- Glucose breath test (GBT): The patient ingests 50-75 grams of glucose, with breath samples collected similarly. Since glucose is completely absorbed in the proximal small intestine, any early rise in hydrogen indicates bacterial fermentation in the proximal small bowel. A rise in hydrogen of ≥12-20 ppm above baseline within 120 minutes is positive. Sensitivity: 20-93%; specificity: 30-86%. More specific but less sensitive than lactulose, as glucose may not detect distal small bowel overgrowth.
- Methane measurement: A methane level of ≥10 ppm at any point during the test is diagnostic for intestinal methanogen overgrowth (IMO). Methane production indicates the presence of Methanobrevibacter smithii and is strongly associated with constipation.
Preparation protocol: Patients must follow a 12-24 hour preparatory diet (white rice, plain chicken, eggs, clear broth only), fast for 12 hours before the test, avoid antibiotics for 4 weeks prior, avoid prokinetics and laxatives for 1 week, and brush teeth without swallowing mouthwash before testing. Non-fermentable toothpaste should be used on the morning of the test.
Trio-Smart Breath Test
The trio-smart breath test is a newer breath testing modality that simultaneously measures all three fermentation gases: hydrogen, methane, and hydrogen sulfide. The addition of hydrogen sulfide measurement addresses the approximately 15-20% of SIBO cases that produce a "flat-line" (non-hydrogen, non-methane) breath test pattern, previously classified as false negatives. Hydrogen sulfide levels ≥3 ppm are considered elevated and associated with diarrhea-predominant symptoms.
Adjunctive Laboratory Testing
- Vitamin B12 level: Low in SIBO due to bacterial consumption (unlike in short bowel syndrome where folate is low)
- Folate level: Normal or elevated due to bacterial production
- Iron studies: Iron deficiency pattern from malabsorption
- Fat-soluble vitamins (A, D, E, K): May be reduced
- Complete blood count: Macrocytic anemia (B12 deficiency) or microcytic anemia (iron deficiency) or combined
- Fecal fat testing: Elevated in cases with significant bile acid deconjugation
- D-xylose absorption test: Abnormal in SIBO due to mucosal damage and bacterial metabolism of the substrate
- Anti-vinculin and anti-CdtB antibodies: Biomarkers for post-infectious IBS/SIBO, measuring autoantibodies against the interstitial cells of Cajal and cytolethal distending toxin B
7. Treatment
Antibiotic Therapy
Antimicrobial therapy is the cornerstone of SIBO treatment, with the choice of antibiotic guided by the dominant gas pattern:
- Rifaximin (Xifaxan) 550 mg three times daily for 14 days: The most extensively studied and preferred antibiotic for hydrogen-dominant SIBO. Rifaximin is a non-absorbable antibiotic that acts locally in the gastrointestinal tract with minimal systemic absorption (<0.4%), resulting in an excellent safety profile. The landmark TARGET study demonstrated an overall eradication rate of 64-74% with a single 2-week course. Rifaximin is also FDA-approved for IBS-D based on the TARGET 1, 2, and 3 trials.
- Rifaximin plus neomycin for methane-dominant SIBO (IMO): Rifaximin 550 mg TID plus neomycin 500 mg BID for 14 days. Combination therapy is necessary because rifaximin alone is poorly effective against methanogens. The combination achieves methane normalization in approximately 85% of patients, compared to 28% with rifaximin alone. Alternative methanogen-targeting agents include metronidazole 250 mg TID or partially hydrolyzed guar gum (PHGG) as an adjunct.
- Other antibiotics: Metronidazole (250 mg TID for 7-10 days), ciprofloxacin (500 mg BID for 7 days), amoxicillin-clavulanate (875/125 mg BID for 14 days), and trimethoprim-sulfamethoxazole may be used in resource-limited settings or when rifaximin is unavailable.
Herbal Antimicrobial Therapy
A landmark study by Chedid et al. (2014) published in Global Advances in Health and Medicine demonstrated that herbal antimicrobials are as effective as rifaximin for SIBO eradication, with a 46% eradication rate for herbal protocols versus 34% for rifaximin. Commonly used herbal protocols include:
- Allicin (garlic extract) 450 mg BID-TID: Particularly effective against methanogens; allicin is one of the few natural compounds with demonstrated anti-archaeal activity against Methanobrevibacter smithii.
- Berberine (500 mg TID): Broad-spectrum antimicrobial from goldenseal, Oregon grape, and barberry. Also has prokinetic and anti-inflammatory properties.
- Oregano oil (200 mg BID): Contains carvacrol and thymol with broad-spectrum antibacterial activity.
- Neem (300 mg TID): Traditional Ayurvedic antimicrobial with activity against gram-negative organisms.
- FC Cidal and Dysbiocide (Biotics Research): Combination herbal formulation used in the Chedid study protocol.
- Candibactin-AR and Candibactin-BR (Metagenics): Commercial herbal antimicrobial combinations used in the Chedid study.
Elemental Diet
The elemental diet is a liquid formula containing pre-digested nutrients (amino acids, simple sugars, medium-chain triglycerides, and micronutrients) that are absorbed in the proximal jejunum, effectively starving bacteria in the mid and distal small intestine. A 2004 study by Pimentel et al. demonstrated an 80-85% normalization rate of lactulose breath tests after 14 days of exclusive elemental diet, and 85% after 21 days. The elemental diet is considered the most effective single intervention for SIBO but is limited by poor palatability, high cost, and difficulty with compliance. Semi-elemental diets with partially hydrolyzed proteins offer an alternative with improved palatability.
Prokinetic Therapy (Preventing Recurrence)
Because impaired motility (particularly reduced MMC activity) is the most common underlying cause of SIBO, prokinetic agents that restore the MMC are critical for preventing relapse after antibiotic eradication:
- Low-dose erythromycin (50-100 mg at bedtime): Acts as a motilin receptor agonist at sub-antimicrobial doses, stimulating Phase III of the MMC. One of the most effective prokinetic agents for SIBO prevention.
- Low-dose naltrexone (LDN, 2.5-4.5 mg at bedtime): Opioid receptor antagonist that has been shown to improve MMC activity and reduce SIBO recurrence.
- Prucalopride (1-2 mg daily): Selective 5-HT4 receptor agonist that stimulates high-amplitude propagating contractions and MMC activity.
- Iberogast (STW 5): Herbal prokinetic containing nine botanical extracts with demonstrated effects on gastric and intestinal motility.
- Ginger extract (Zingiber officinale, 1000 mg daily): Stimulates gastric emptying and intestinal motility through 5-HT3 and 5-HT4 receptor modulation.
Dietary Management
- Low-FODMAP diet: Restriction of fermentable oligosaccharides, disaccharides, monosaccharides, and polyols reduces substrate for bacterial fermentation and provides symptomatic relief, though it does not eradicate SIBO. Best used as an adjunct to antimicrobial therapy and during the treatment phase.
- Specific Carbohydrate Diet (SCD): Eliminates complex carbohydrates and disaccharides, allowing only monosaccharides. Some practitioners combine SCD principles with low-FODMAP restrictions.
- Bi-Phasic Diet (Dr. Nirala Jacobi): A structured dietary protocol specifically designed for SIBO treatment, progressing from a restrictive to a more liberal phase over 8 weeks.
- Meal spacing: Allowing 4-5 hours between meals and avoiding snacking enables the MMC to cycle through Phase III, performing its "housekeeping" sweep of the small intestine. The MMC is inhibited by food intake.
8. Complications
- Severe malnutrition: Prolonged untreated SIBO can cause clinically significant malabsorption of macronutrients and micronutrients, leading to weight loss, muscle wasting, and sarcopenia.
- Vitamin B12 deficiency neuropathy: Chronic B12 depletion can cause subacute combined degeneration of the spinal cord, peripheral neuropathy, and irreversible neurological damage if untreated.
- Osteoporosis and osteomalacia: From vitamin D and calcium malabsorption.
- Coagulopathy: Vitamin K malabsorption can cause bleeding diathesis, particularly in patients on anticoagulants.
- D-lactic acidosis: In severe cases, particularly following bariatric surgery, bacterial production of D-lactic acid can cause episodic encephalopathy, ataxia, and metabolic acidosis.
- Intestinal permeability and systemic inflammation: Chronic SIBO increases intestinal permeability, facilitating bacterial translocation and endotoxemia, contributing to hepatic steatosis (NAFLD) and systemic inflammatory conditions.
- Autoimmune conditions: Increased intestinal permeability and molecular mimicry have been implicated in the development or exacerbation of autoimmune diseases including Hashimoto's thyroiditis and rheumatoid arthritis.
- High recurrence rate: SIBO has a recurrence rate of 44-46% within 9-12 months after successful antibiotic eradication, necessitating identification and treatment of underlying predisposing factors.
9. Prognosis
The prognosis for SIBO depends heavily on the underlying cause and the ability to address predisposing factors. In patients with correctable underlying causes (such as discontinuing PPIs, treating hypothyroidism, or surgical correction of anatomical abnormalities), SIBO can often be permanently eradicated. However, in patients with irreversible predisposing conditions (such as systemic sclerosis, diabetic autonomic neuropathy, or surgical blind loops), SIBO tends to be a chronic, relapsing condition requiring long-term management strategies.
With appropriate antibiotic therapy, the initial eradication rate is 51-74% for rifaximin and 80-85% for the elemental diet. However, the recurrence rate remains high at 44-46% within 9-12 months, underscoring the importance of addressing the root cause. Patients who are placed on prokinetic therapy after antibiotic eradication show significantly lower recurrence rates. A study of low-dose erythromycin (50 mg nightly) demonstrated a recurrence rate reduction to approximately 20% at 12 months compared to 46% without prokinetic therapy.
For patients with IBS-SIBO overlap, successful eradication of SIBO leads to significant improvement in IBS symptoms in 48-75% of cases. The identification and treatment of SIBO in patients previously labeled with refractory IBS represents a major advance in functional gastroenterology. Long-term management typically involves a combination of dietary modifications (low-FODMAP, meal spacing), prokinetic therapy, periodic breath test monitoring, and retreatment with antibiotics or herbal antimicrobials as needed.
10. Prevention
- Restore and maintain MMC function: The MMC is the body's primary defense against SIBO. Strategies to support MMC include avoiding unnecessary snacking (allow 4-5 hours between meals), considering prokinetic agents when motility is impaired, and maintaining regular meal timing.
- Minimize PPI use: Use proton pump inhibitors only when clearly indicated (documented GERD, Barrett's esophagus, Zollinger-Ellison syndrome) and at the lowest effective dose. Consider step-down to H2 receptor antagonists when appropriate.
- Address hypothyroidism: Optimize thyroid hormone levels, as hypothyroidism significantly impairs intestinal motility.
- Glycemic control in diabetes: Optimize blood glucose management to prevent or slow progression of diabetic autonomic neuropathy and gastroparesis.
- Judicious antibiotic use: While antibiotics treat SIBO, repeated or prolonged courses can disrupt the protective commensal microbiome and potentially create resistant organisms.
- Post-gastroenteritis vigilance: Acute gastroenteritis (particularly from Campylobacter jejuni, Salmonella, Shigella, and E. coli) can damage the interstitial cells of Cajal and produce autoantibodies against vinculin, leading to chronic MMC impairment and SIBO. Prompt and complete treatment of acute gastroenteritis may reduce this risk.
- Avoid unnecessary opioids: Opioids powerfully inhibit intestinal motility and MMC function.
- Regular physical activity: Moderate exercise promotes intestinal motility and may reduce SIBO risk.
- Stress management: Chronic psychological stress impairs MMC function through sympathetic nervous system activation and cortisol-mediated effects on intestinal motility.
11. Recent Research and Advances
The understanding and management of SIBO has evolved rapidly in recent years. The reclassification of methane-dominant SIBO as intestinal methanogen overgrowth (IMO) by Pimentel et al. (2020) reflects the recognition that methanogens (Methanobrevibacter smithii) are archaea, not bacteria, and that methanogen overgrowth can occur throughout the intestine, not just the small bowel. This reclassification has important implications for treatment algorithms and ongoing research.
The development of the trio-smart breath test for simultaneous measurement of hydrogen, methane, and hydrogen sulfide represents a significant diagnostic advance. Research has identified hydrogen sulfide-producing bacteria (primarily Desulfovibrio and Fusobacterium species) as a distinct cause of SIBO symptoms, with specific associations with diarrhea, visceral hypersensitivity, and sulfurous eructation. Bismuth subsalicylate has shown promise as a targeted therapy for hydrogen sulfide-dominant SIBO by binding hydrogen sulfide in the gut lumen.
The anti-vinculin and anti-CdtB antibody tests (marketed as ibs-smart) have emerged as biomarkers for post-infectious IBS/SIBO, providing an objective tool to identify patients whose SIBO developed as a consequence of acute gastroenteritis with autoimmune damage to the interstitial cells of Cajal. This has opened new avenues for understanding the pathogenesis of post-infectious functional gastrointestinal disorders. Lovastatin lactone, a statin derivative, has demonstrated specific anti-methanogenic activity by inhibiting the enzyme HMG-CoA reductase in M. smithii, and phase II clinical trials are underway (SYN-010). Research into the small intestinal microbiome using capsule-based sampling devices and metagenomic sequencing is providing unprecedented insights into the composition and metabolic activity of the small intestinal microbial community in health and SIBO.
12. References & Research
Historical Background
The concept of bacterial overgrowth in the small intestine was first described in the context of surgically created blind loops in the early 20th century, with Faber reporting macrocytic anemia associated with intestinal stasis in 1897. The "blind loop syndrome" was formally characterized in the 1960s and 1970s by researchers including Tabaqchali and Booth, who demonstrated that bacterial overgrowth in surgically created blind loops caused vitamin B12 malabsorption and steatorrhea. The modern understanding of SIBO as a widespread clinical entity beyond the surgical context was significantly advanced by the work of Mark Pimentel at Cedars-Sinai Medical Center beginning in the early 2000s, whose research established the connection between SIBO and IBS, developed lactulose breath testing protocols, and demonstrated the efficacy of rifaximin for treatment.
Key Research Papers
- Pimentel M, Saad RJ, Long MD, Rao SSC. ACG Clinical Guideline: Small Intestinal Bacterial Overgrowth. American Journal of Gastroenterology. 2020;115(2):165-178.
- Rezaie A, et al. Hydrogen and methane-based breath testing in gastrointestinal disorders: the North American Consensus. American Journal of Gastroenterology. 2017;112(5):775-784.
- Pimentel M, et al. Rifaximin therapy for patients with irritable bowel syndrome without constipation (TARGET 1 and TARGET 2). New England Journal of Medicine. 2011;364(1):22-32.
- Ghoshal UC, Shukla R, Ghoshal U. Small intestinal bacterial overgrowth and irritable bowel syndrome: a bridge between functional organic dichotomy. Gut and Liver. 2017;11(2):196-208.
- Chedid V, et al. Herbal therapy is equivalent to rifaximin for the treatment of small intestinal bacterial overgrowth. Global Advances in Health and Medicine. 2014;3(3):16-24.
- Pimentel M, et al. A 14-day elemental diet is highly effective in normalizing the lactulose breath test. Digestive Diseases and Sciences. 2004;49(1):73-77.
- Pimentel M, et al. A link between irritable bowel syndrome and fibromyalgia may be related to findings on lactulose breath testing. Annals of the Rheumatic Diseases. 2004;63(4):450-452.
- Lin HC. Small intestinal bacterial overgrowth: a framework for understanding irritable bowel syndrome. JAMA. 2004;292(7):852-858.
- Pimentel M, et al. Methane, a gas produced by enteric bacteria, slows intestinal transit and augments small intestinal contractile activity. American Journal of Physiology. 2006;290(6):G1089-G1095.
- Bures J, et al. Small intestinal bacterial overgrowth syndrome. World Journal of Gastroenterology. 2010;16(24):2978-2990.
- Dukowicz AC, Lacy BE, Levine GM. Small intestinal bacterial overgrowth: a comprehensive review. Gastroenterology and Hepatology. 2007;3(2):112-122.
- Pimentel M, et al. Autoimmunity links vinculin to the pathophysiology of chronic functional bowel changes following Campylobacter jejuni infection in a rat model. Digestive Diseases and Sciences. 2015;60(5):1195-1205.
- Takakura W, Pimentel M. Small intestinal bacterial overgrowth and irritable bowel syndrome: an update. Frontiers in Psychiatry. 2020;11:664.
- Singer-Englar T, et al. Validation of a hydrogen and methane and hydrogen sulfide breath test device. Clinical Gastroenterology and Hepatology. 2022;20(7):e1488-e1497.
Research Papers
Curated PubMed topic searches of peer-reviewed literature on Small Intestinal Bacterial Overgrowth (SIBO). Each link opens a live PubMed query so you always see the most current studies.
- PubMed: SIBO diagnosis
- PubMed: Rifaximin for SIBO
- PubMed: Hydrogen breath testing
- PubMed: SIBO and IBS overlap
- PubMed: Methane/IMO
- PubMed: PPI and SIBO
- PubMed: Prokinetics and motility
- PubMed: Elemental diet for SIBO
- PubMed: Low-FODMAP diet and SIBO
- PubMed: SIBO recurrence
- PubMed: SIBO in scleroderma
- PubMed: Short bowel syndrome and SIBO
Connections
- The Gut Barrier & Your Microbiome — interactive animation
- IMO and Constipation
- Elemental Diet
- Herbal Antimicrobials
- Rifaximin Protocols
- Root Causes
- Breath Test Guide
- Prokinetics and Relapse Prevention
- Low-FODMAP Diet
- Hydrogen vs Methane vs Hydrogen Sulfide
- Irritable Bowel Syndrome
- IBS and SIBO Overlap
- Celiac Disease
- Inflammatory Bowel Disease
- POTS
- MCAS
- Thyroid Disorders
- Berberine
- Elimination Diet
- High Resistant Starch Foods — food rankings by RS grams per serving, the cook-and-cool RS3 protocol, a daily ~20g meal plan, and butyrate/SCFA mechanism.
- Yeast Infections