IBD Diagnostic Workup: Calprotectin, Colonoscopy, and MR Enterography
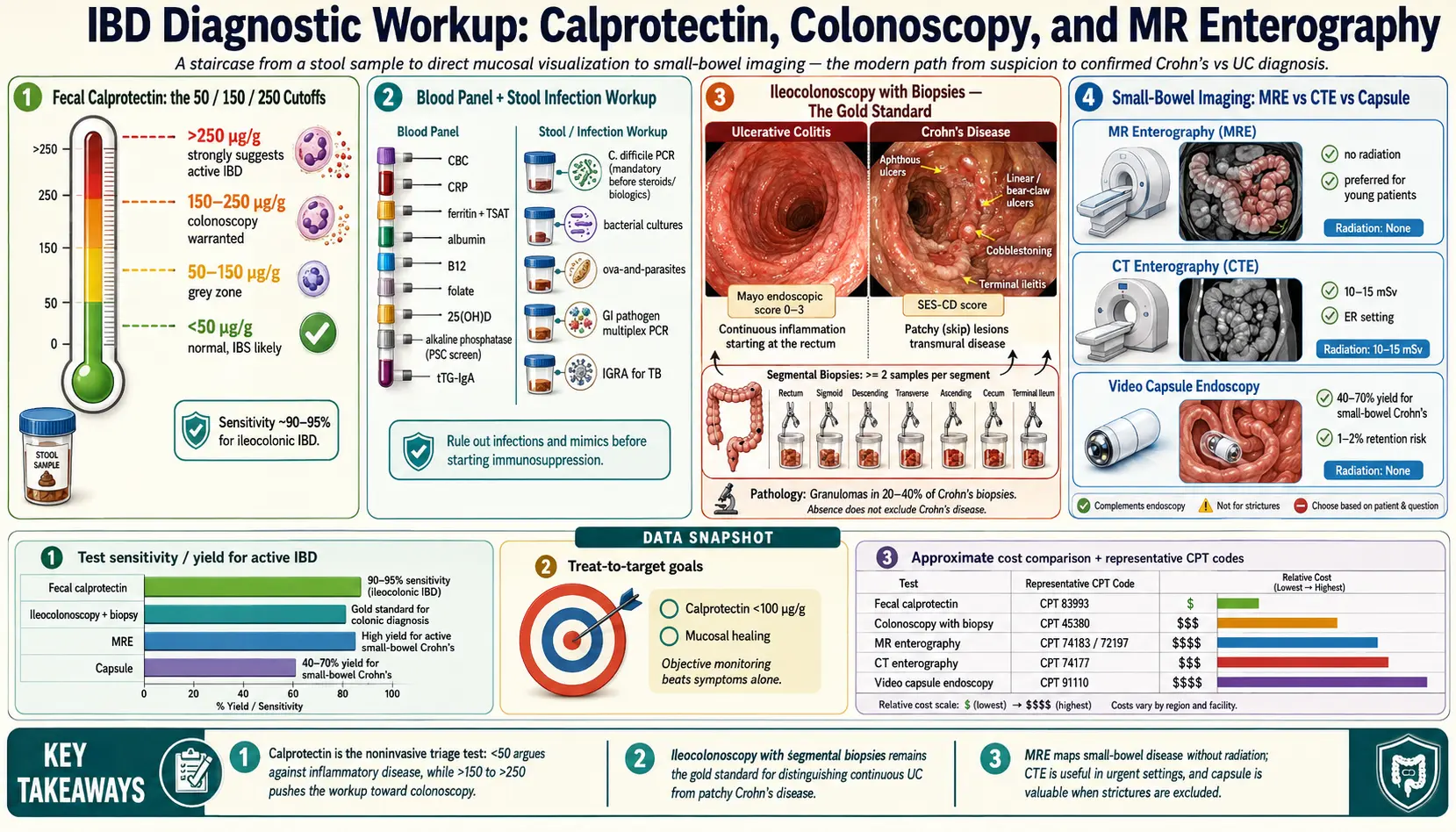
Table of Contents
- Why the Workup Matters
- Fecal Calprotectin — The 50/150/250 Cutoffs
- Calprotectin: IBD vs IBS
- Blood Panels — CBC, CRP, Iron, Albumin
- Stool Testing to Rule Out Infection
- Ileocolonoscopy with Biopsy — The Gold Standard
- CT Enterography vs MR Enterography
- Small-Bowel Capsule Endoscopy
- Upper Endoscopy (EGD) for Crohn's
- Serology — ASCA, pANCA, anti-OmpC Limits
- How to Prep and What to Expect
- Insurance and Cost Tactics
- Key Research Papers
- Connections
- Featured Videos
Why the Workup Matters
Inflammatory bowel disease is a diagnosis you do not want guessed. Crohn's disease and ulcerative colitis are lifelong conditions that shape your medication choices, insurance claims, surgery risk, cancer surveillance schedule, and pregnancy planning for the next fifty years. At the same time, the symptoms — diarrhea, cramping, blood in the stool, weight loss, fatigue — overlap with irritable bowel syndrome, celiac disease, microscopic colitis, bile acid diarrhea, lactose intolerance, and half a dozen infections. Getting the label right is everything.
The modern workup is a staircase. A stool test (fecal calprotectin) and a handful of blood labs tell your gastroenterologist whether real inflammation is happening somewhere in your gut. If the answer is yes, an ileocolonoscopy with biopsies is the gold-standard next step because it actually looks at the tissue and takes samples. If Crohn's disease is on the table, cross-sectional imaging of the small bowel — usually MR enterography — maps out disease above the reach of the colonoscope. A few specialized tests (capsule endoscopy, upper endoscopy, serology) fill in remaining gaps.
This article walks through each piece — what it measures, what the numbers mean, how it feels, what it costs, and how to push back if your insurance company drags its feet.
Fecal Calprotectin — The 50/150/250 Cutoffs
Calprotectin is a calcium-binding protein that lives inside neutrophils, the white blood cells that rush into inflamed tissue. When neutrophils spill into the gut lining, they leak calprotectin into stool. The concentration you measure in a single stool sample correlates tightly with the amount of neutrophilic inflammation in the bowel wall.
You collect a small stool sample at home in a plastic scoop, package it per lab instructions, and drop it off. Results come back in 2–5 days. Most U.S. labs report in micrograms per gram of stool (µg/g).
Three numbers matter:
- Under 50 µg/g — Normal. Very low probability of active IBD. This result essentially rules out Crohn's disease or ulcerative colitis as the driver of your symptoms. Irritable bowel syndrome becomes the leading explanation.
- 50–150 µg/g — Indeterminate ("grey zone"). Could be mild IBD, could be a non-IBD cause (NSAID damage, an enteric infection, reflux, a polyp, even intense exercise). Usually retested in 4–6 weeks; if it stays elevated, push for colonoscopy.
- 150–250 µg/g — Elevated. Inflammation is real. Colonoscopy is warranted. In a known IBD patient, this range suggests low-grade active disease or early relapse.
- Over 250 µg/g — Clearly abnormal. Strongly suggests active IBD (or occasionally severe infectious colitis, NSAID colopathy, or colorectal cancer). Colonoscopy is urgent.
Different labs use slightly different cutoff values and different assay kits, so always look at your lab's reference range rather than assuming a universal number. For IBD monitoring — tracking a patient already diagnosed — many gastroenterologists aim for a target below 150 µg/g on therapy, and values under 100 µg/g correlate well with endoscopic remission (mucosal healing).
Calprotectin is stable at room temperature for several days, which makes home collection practical. It costs $100–$250 out of pocket at commercial labs (LabCorp, Quest) and is usually covered by insurance when ordered for the evaluation of chronic diarrhea, blood in stool, or suspected IBD. Billing code: CPT 83993.
Calprotectin: IBD vs IBS
The single most useful thing calprotectin does is separate inflammatory gut disease from functional gut disease. Irritable bowel syndrome, which affects roughly 10–15% of adults, causes very similar symptoms — cramping, bloating, altered bowel habits — but does not involve mucosal inflammation. Calprotectin in true IBS is almost always under 50 µg/g. Calprotectin in untreated active IBD is almost always over 150 µg/g and frequently over 500.
For a patient with chronic diarrhea and normal routine labs, a calprotectin in the normal range lets you and your gastroenterologist confidently pursue an IBS workup (food triggers, FODMAPs, low-FODMAP elimination, SIBO evaluation, bile acid testing) rather than a colonoscopy. That is not laziness — it is pattern-appropriate medicine. See the Irritable Bowel Syndrome page for the parallel workup.
The test's sensitivity for ileocolonic IBD is in the 90–95% range. The one meaningful blind spot is isolated small-bowel Crohn's disease, especially high in the jejunum, where the inflammation may not shed enough neutrophils into stool to lift the number reliably. If small-bowel symptoms persist despite a normal calprotectin, imaging (MR enterography) is still worth pursuing.
Blood Panels — CBC, CRP, Iron, Albumin
A focused blood panel rounds out the initial screen. The key tests:
- Complete blood count (CBC). Anemia is one of the most common objective findings in IBD. A low hemoglobin with a low mean corpuscular volume (MCV) points toward iron-deficiency anemia from chronic blood loss. Elevated platelets (thrombocytosis) and elevated white cell count are nonspecific signs of inflammation.
- C-reactive protein (CRP). An acute-phase protein made by the liver in response to inflammatory cytokines. Elevated CRP (>5 mg/L) supports active inflammation. About 20–30% of patients with active IBD have a normal CRP, particularly in limited ulcerative colitis, so a normal CRP does not rule out disease.
- Erythrocyte sedimentation rate (ESR). Older, slower marker — often ordered alongside CRP. Less specific but occasionally useful when CRP is borderline.
- Iron studies. Serum iron, total iron-binding capacity (TIBC), transferrin saturation, and ferritin. Ferritin is an acute-phase reactant and rises in inflammation, so it can look falsely "normal" even when iron stores are depleted. Transferrin saturation under 20% combined with a ferritin under 100 µg/L in an IBD patient is considered iron-deficient by modern guidelines.
- Albumin. A low serum albumin (under 3.5 g/dL) in an IBD patient suggests protein-losing enteropathy from severe inflammation, and it predicts worse outcomes in hospitalized ulcerative colitis.
- Vitamin B12, folate, 25-OH vitamin D. Ileal Crohn's disease impairs B12 absorption. Both Crohn's and UC patients frequently run low in vitamin D. Folate deficiency can develop with sulfasalazine or methotrexate therapy.
- Liver enzymes (AST, ALT, alkaline phosphatase, GGT). Elevated alkaline phosphatase raises the question of primary sclerosing cholangitis, a bile-duct disease with a strong association to ulcerative colitis.
- Tissue transglutaminase IgA (tTG-IgA) and total IgA. Screen for celiac disease, which can mimic or coexist with IBD. See the celiac disease page for a full workup.
Stool Testing to Rule Out Infection
Before anyone labels you with IBD, infection has to come off the table. Several bacterial and parasitic gut infections cause bloody diarrhea and elevated calprotectin that looks exactly like ulcerative colitis on first presentation. Equally important, infections — especially Clostridioides difficile — commonly trigger flares in patients already diagnosed with IBD.
The standard panel:
- C. difficile PCR or GDH/toxin EIA. Essential before starting steroids or biologics. Missed C. diff in an IBD flare can be catastrophic.
- Stool culture for Salmonella, Shigella, Campylobacter, Yersinia, and shiga-toxin-producing E. coli.
- Ova and parasites — particularly Giardia and Entamoeba histolytica, which cause chronic diarrhea that can be mistaken for Crohn's.
- GI pathogen PCR panel (e.g., BioFire, Verigene). One stool sample tests for 20+ bacterial, viral, and parasitic pathogens at once. Faster and more sensitive than culture, though more expensive.
In patients with a travel history or immigration history from endemic regions, tuberculosis screening (interferon-gamma release assay) is also essential, because intestinal TB mimics Crohn's disease on imaging and biopsy — and starting an anti-TNF biologic for presumed Crohn's in someone who actually has TB can disseminate the infection catastrophically.
Ileocolonoscopy with Biopsy — The Gold Standard
Nothing replaces a direct look at the bowel lining. An ileocolonoscopy — a colonoscopy extended into the terminal ileum (the last 10–20 cm of small bowel before the colon) — is the definitive test for diagnosing IBD and distinguishing Crohn's disease from ulcerative colitis.
What the gastroenterologist is looking for:
- Pattern of inflammation. Ulcerative colitis causes continuous inflammation starting at the rectum and extending proximally for a variable distance. Crohn's disease causes patchy "skip lesions" with normal mucosa between inflamed segments, and it very often involves the terminal ileum.
- Ulcer appearance. UC tends to produce superficial ulcers, granular mucosa, and loss of the normal vascular pattern. Crohn's produces deeper, linear or "aphthous" ulcers, cobblestoning, and strictures.
- Biopsies. At least 2 samples from each anatomical segment (terminal ileum, cecum, ascending, transverse, descending, sigmoid, rectum), including visibly normal-appearing areas. Microscopy reveals crypt architectural distortion, crypt abscesses, basal plasmacytosis (UC), or granulomas (Crohn's, in about 20–40% of cases).
See Crohn's vs Ulcerative Colitis: Key Differences for a side-by-side breakdown of every distinguishing feature.
Colonoscopy also stages the disease: the Mayo score (UC) and the Simple Endoscopic Score for Crohn's Disease (SES-CD) are used to classify severity and to compare before-and-after treatment. Mucosal healing on repeat colonoscopy — not just symptom relief — is the modern treatment goal, because it predicts fewer flares, fewer hospitalizations, and less surgery long-term.
CT Enterography vs MR Enterography
The colonoscope reaches the last bit of the small intestine, but it cannot see the 20-plus feet of jejunum and ileum above it. For suspected or confirmed Crohn's disease, cross-sectional imaging of the small bowel is standard. Two options dominate: CT enterography (CTE) and MR enterography (MRE).
Both involve drinking 1–1.5 liters of a neutral-density oral contrast (usually a flavored polyethylene glycol or mannitol solution) over 45–60 minutes before the scan to distend the small bowel. Without that distension, the loops collapse and you cannot see the wall properly.
CT enterography is faster (a 30-second breath-hold scan after oral prep), widely available, and excellent at detecting bowel-wall thickening, active inflammation, abscesses, fistulae, and strictures. The downside is ionizing radiation — roughly 10–15 mSv per exam, equivalent to 3–5 years of background exposure. Young IBD patients typically have cumulative imaging needs over decades, so radiation dose adds up.
MR enterography uses magnetic resonance imaging instead of X-rays. No radiation. The scan is longer — 30–45 minutes inside the scanner, multiple breath-holds, intravenous gadolinium contrast, and often an antispasmodic injection (glucagon or hyoscine) to freeze bowel motion. Image quality for mucosal detail and active inflammation is at least equal to CTE and often superior. MRE is the preferred choice for:
- Patients under 40, especially young women.
- Patients with established Crohn's who need repeated imaging.
- Evaluation of perianal fistulizing disease (a dedicated pelvic MRI is the standard for perianal Crohn's).
- Pregnancy (no gadolinium in the first trimester, but MRI without contrast is still safer than CT).
CTE is preferred when speed matters — in the emergency department for suspected obstruction or abscess, or in patients with implanted metal (certain pacemakers, cochlear implants) or severe claustrophobia. CTE typically costs $800–$2,000; MRE runs $1,500–$4,500. Both are usually covered by insurance with prior authorization when ordered for IBD workup.
Small-Bowel Capsule Endoscopy
Video capsule endoscopy (VCE) is a vitamin-sized camera you swallow. Over 8–10 hours it snaps around 50,000 images as it moves through your small intestine, and it transmits them to a recorder worn on a belt. The capsule passes naturally in stool 1–3 days later.
VCE excels at detecting subtle small-bowel mucosal disease that MR enterography and CT enterography can miss — tiny aphthous ulcers, mild erythema, early Crohn's lesions in the proximal jejunum. Its diagnostic yield for suspected small-bowel Crohn's disease in patients with normal ileocolonoscopy and normal cross-sectional imaging is roughly 40–70%.
The main risk is capsule retention — the camera getting stuck behind a stricture, which happens in about 1–2% of IBD patients. A retained capsule may require surgical or endoscopic removal. For this reason, anyone with suspected or confirmed Crohn's typically has either an MR enterography first (to identify strictures) or a patency capsule — a dissolvable dummy capsule — before the real camera. If the patency capsule passes cleanly in 30 hours, the VCE is considered safe.
VCE is not usually first-line; it is a second-tier test when routine workup is normal but clinical suspicion of small-bowel disease persists, or for monitoring known small-bowel Crohn's under therapy.
Upper Endoscopy (EGD) for Crohn's
Crohn's disease can involve any part of the GI tract from mouth to anus, including the esophagus, stomach, and duodenum. Roughly 5–15% of Crohn's patients have upper-tract involvement, and children with Crohn's much more often. For that reason, guidelines recommend upper endoscopy (esophagogastroduodenoscopy, EGD) at initial diagnosis in:
- All pediatric patients with suspected IBD.
- Adults with upper-GI symptoms (dysphagia, persistent nausea, upper abdominal pain, unexplained weight loss).
- Adults where the diagnosis is unclear after colonoscopy — upper-tract granulomas clinch Crohn's disease.
EGD is a 10–15 minute outpatient procedure with light sedation, often combined with colonoscopy in the same visit so you only prep and recover once.
Serology — ASCA, pANCA, anti-OmpC Limits
Three antibodies occasionally come up in IBD evaluation:
- ASCA (anti-Saccharomyces cerevisiae antibodies). Positive in 50–60% of Crohn's patients, 5–15% of UC patients.
- pANCA (perinuclear anti-neutrophil cytoplasmic antibodies). Positive in 60–70% of UC patients, 10–20% of Crohn's.
- Anti-OmpC, anti-CBir1, anti-I2. Antibodies to bacterial proteins; elevated in subsets of Crohn's patients.
The pattern ASCA-positive / pANCA-negative favors Crohn's disease; ASCA-negative / pANCA-positive favors ulcerative colitis. Commercial panels (e.g., Prometheus IBD sgi Diagnostic) combine these with genetic markers.
The honest limit is that these tests do not diagnose IBD. Their sensitivity is too low to rule disease in or out, and the false-positive rate in healthy populations is meaningful. Major guidelines (AGA, ACG, ECCO) explicitly recommend against using serology as a primary diagnostic tool. It can occasionally help when colonoscopy findings are ambiguous — indeterminate colitis that could be either Crohn's or UC — but even there it shifts probabilities rather than delivering an answer. If your doctor orders one of these panels, ask what decision it will actually change. Often the answer is "not much."
How to Prep and What to Expect
Calprotectin. No dietary restrictions. Some labs advise avoiding NSAIDs (ibuprofen, naproxen) for 4–7 days beforehand because NSAIDs cause low-level gut inflammation that raises the number falsely. Collect a walnut-sized sample per the lab's kit instructions, refrigerate, and deliver within 24–48 hours.
Colonoscopy prep. The day before the procedure you go on a clear-liquid diet (broth, apple juice, Jell-O, Gatorade — nothing red or purple). In the afternoon or evening you start drinking a laxative solution — typically a split-dose 4-liter polyethylene glycol (GoLytely, NuLytely) or a lower-volume option (SuPrep, Plenvu, MiraLAX plus Gatorade). Half goes down the evening before, half in the early morning of the procedure, finishing at least 2–3 hours before the scope. The goal is clear, yellow-tinged rectal output. The procedure itself takes 30–45 minutes under moderate sedation; you wake up in 15–30 minutes. Drive home with someone else; no alcohol and no important decisions for 24 hours. Tips that help: stay relentlessly hydrated the day before, chill the prep in the refrigerator (cold is more palatable than room temperature), drink through a straw, chase each glass with a lemon wedge or a clear-broth shot, and plan to stay near a bathroom for 4–6 hours once the prep kicks in.
MR enterography. Light breakfast is fine; stop eating 4 hours before the scan. At the imaging center you drink the oral contrast over 45–60 minutes. Then you lie in the scanner, usually prone (face down), with an IV for gadolinium and sometimes an injection of an antispasmodic. Expect 30–45 minutes inside the magnet with multiple breath-holds. Drink extra water afterward to flush the contrast. If you are claustrophobic, ask your physician in advance for a single dose of oral lorazepam 30–60 minutes before the scan, or request an open MRI scanner (though image quality is sometimes lower).
Capsule endoscopy. Clear-liquid diet the day before and a short bowel-prep dose (often half a standard colonoscopy prep). You swallow the capsule with a glass of water, wear the recorder for 8–10 hours, and can resume clear liquids 2 hours after swallowing and solids after 4 hours. Return the recorder that evening or the next morning.
Insurance and Cost Tactics
Diagnostic workups add up fast. A handful of tactics keep costs down and avoid denials:
- Diagnostic vs screening coding matters. A colonoscopy billed as screening (CPT 45378, Z12.11) is typically covered at 100% under preventive-care rules. A colonoscopy billed as diagnostic (for symptoms like bleeding or chronic diarrhea) is subject to your deductible and coinsurance. Ask the billing office how it will be coded before the procedure; the answer hinges on your symptoms and your referral note.
- Prior authorization for MR enterography. Almost always required. Your gastroenterologist's office should submit the request with documentation of symptoms and prior workup. If denied, ask for a peer-to-peer review — a phone call between your specialist and the insurance medical director. These flip denials roughly half the time.
- Calprotectin pushback. Some plans require the test to be billed with a specific diagnosis code (chronic diarrhea, hematochezia, abdominal pain with diarrhea) to pay. If denied, your physician can resubmit with an expanded diagnosis list.
- Facility-fee shopping. A hospital-outpatient colonoscopy can cost 2–5× the same procedure at a freestanding ambulatory surgery center. Ask your gastroenterologist whether they have privileges at a surgery center and request that option.
- Cash pricing. For imaging, cash prices at independent imaging centers often undercut what insurance would bill (and what you would pay toward your deductible). MR enterography self-pay can be $800–$1,500 at independent facilities versus $3,000+ at a hospital.
- Appeal letters work. A denied capsule endoscopy or MRE appealed with a letter from your gastroenterologist citing American Gastroenterological Association or American College of Gastroenterology guidelines is reversed more often than not. Insurance counts on you giving up; do not.
- Patient assistance for endoscopy. If you are uninsured, many academic centers have sliding-scale GI clinics and research protocols that include free or reduced-cost colonoscopy and imaging.
Finally, keep copies of every report — endoscopy photos, pathology, calprotectin values, MRE images on CD. You will move, switch insurance plans, change gastroenterologists, and maybe seek a second opinion over the decades you live with this disease. A well-organized binder or shared cloud folder saves you from repeating tests and from the slow drift of diagnostic clarity that happens when nobody has the baseline data.
Key Research Papers
- Lichtenstein GR, et al. ACG Clinical Guideline: Management of Crohn's Disease in Adults. Am J Gastroenterol. 2018.
- Rubin DT, et al. ACG Clinical Guideline: Ulcerative Colitis in Adults. Am J Gastroenterol. 2019.
- Maaser C, et al. ECCO-ESGAR Guideline for Diagnostic Assessment in IBD Part 1: Initial Diagnosis, Monitoring of Known IBD, Detection of Complications. Gut. 2019.
- van Rheenen PF, et al. Faecal calprotectin for screening of patients with suspected inflammatory bowel disease: diagnostic meta-analysis. BMJ. 2010.
- Turner D, et al. STRIDE-II: An Update on the Selecting Therapeutic Targets in Inflammatory Bowel Disease (STRIDE) Initiative. Gastroenterology. 2021.
- Bruining DH, et al. Consensus Recommendations for Evaluation, Interpretation, and Utilization of CT and MR Enterography in Patients with Small Bowel Crohn's Disease. Radiology. 2018.
Live PubMed Searches
For further reading, the following PubMed topic searches return current peer-reviewed work on each component of the IBD diagnostic workup:
- Fecal calprotectin in IBD diagnosis and monitoring
- Calprotectin differentiating IBS from IBD
- Ileocolonoscopy and biopsy protocols for IBD
- MR enterography in Crohn's disease
- CT enterography for small-bowel evaluation
- Capsule endoscopy in suspected small-bowel Crohn's
- ASCA, pANCA, and IBD serology
- Mucosal healing as a treatment target in IBD
Connections
- Inflammatory Bowel Disease Overview
- Crohn's vs Ulcerative Colitis: Key Differences
- Biologics: TNF, IL-23, and Integrin Inhibitors
- Diet for IBD: SCD and Mediterranean
- IBD Surgery Decisions
- Extraintestinal Manifestations: Joints, Skin, Eyes
- IBD Fatigue, Anemia, and Nutrient Deficiencies
- Pregnancy and IBD
- JAK Inhibitors and S1P Modulators
- Crohn's Disease
- Ulcerative Colitis
- Endoscopy, Biopsy, and Marsh Classification
- Full-Body MRI Screening
- Ankylosing Spondylitis