IBS and SIBO Overlap
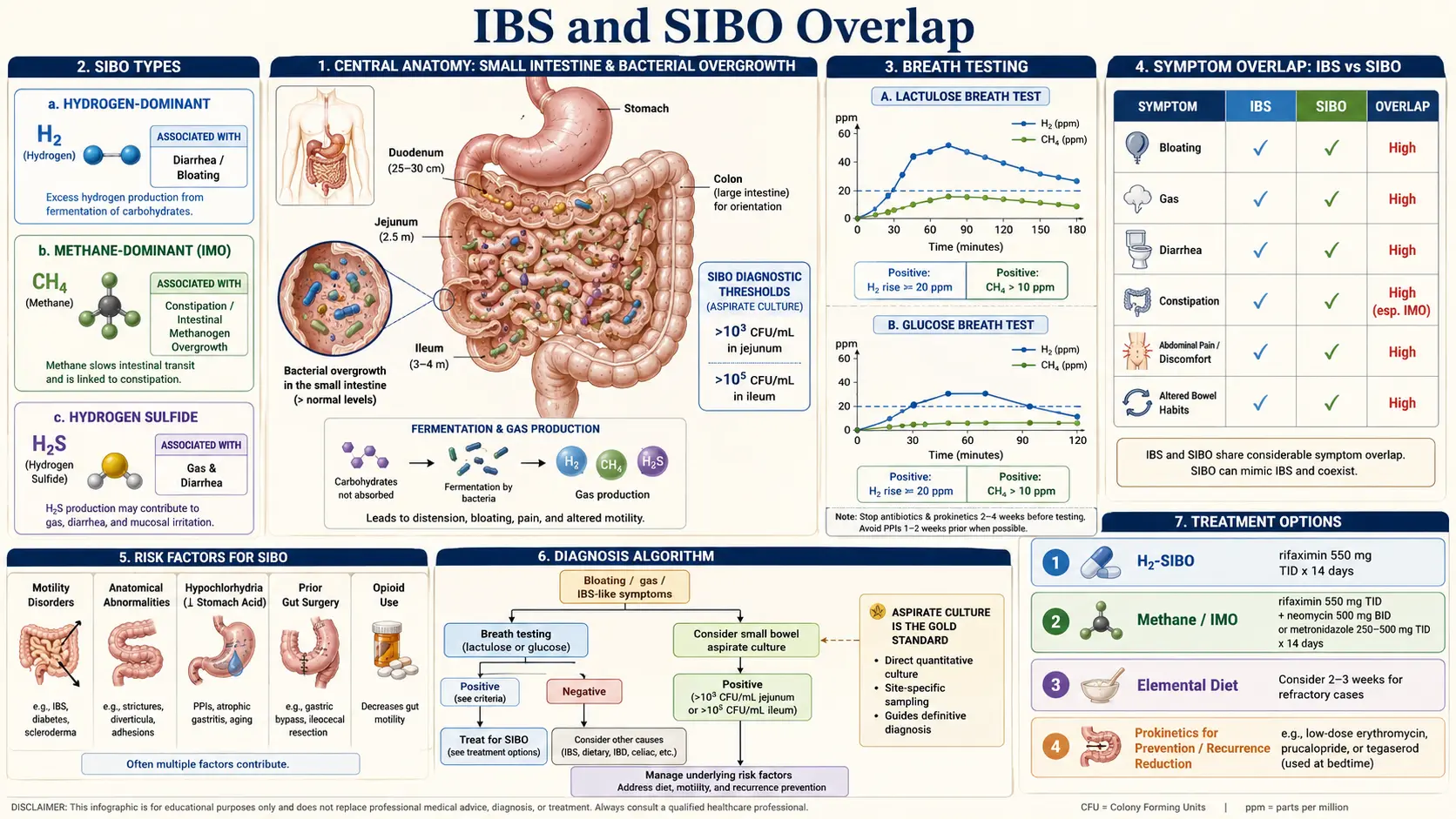
Table of Contents
- Why This Overlap Matters
- The Pimentel Studies — Where This All Started
- Cause, Consequence, or Co-Traveler?
- When to Get a Breath Test
- How the Test Actually Works
- Interpreting Your Results
- Why IBS-D Maps to Hydrogen and IBS-C Maps to Methane
- Rifaximin in IBS-D — The TARGET Trials
- Treating Methane-Dominant IMO
- When to Treat the SIBO vs. Treat the IBS
- Finding the Root Cause
- Realistic Expectations — Why Relapse Is the Rule
- Why You Should Not Cycle Antibiotics Forever
- Key Research Papers
- Connections
- Featured Videos
Why This Overlap Matters
If you have been told you have irritable bowel syndrome and the standard advice — fiber, peppermint oil, an antispasmodic, maybe an antidepressant — has not fixed you, the question worth asking is whether part of your IBS is actually small intestinal bacterial overgrowth (SIBO) hiding under the IBS label. For a sizable fraction of IBS patients, it is. Treating the overgrowth changes the game — sometimes dramatically, sometimes only for a while, but often enough that missing the diagnosis is one of the costliest oversights in GI care.
IBS is a syndrome, which means it is defined by symptoms, not by a cause. SIBO is a diagnosis, defined by an abnormal bacterial population in a place (the small intestine) where bacteria should be relatively sparse. The two labels describe different things, and a person can carry both. The question is how often, and what to do about it.
The Pimentel Studies — Where This All Started
The modern IBS-SIBO story begins at Cedars-Sinai in Los Angeles, with a gastroenterologist named Mark Pimentel. In a landmark 2000 paper and a series of follow-ups through the 2000s, Pimentel and colleagues took consecutive IBS patients and put them through a lactulose breath test. The results reshaped an entire field:
- Roughly 60–80% of patients with diarrhea-predominant IBS (IBS-D) produced an abnormal hydrogen rise on breath testing — the fingerprint of a hydrogen-producing bacterial overgrowth in the small bowel.
- Patients with constipation-predominant IBS (IBS-C) overwhelmingly produced excess methane instead — the signature of archaeal overgrowth, now formally called intestinal methanogen overgrowth (IMO).
- When the overgrowth was treated with antibiotics, IBS symptoms improved in parallel with the breath-test numbers — for many, the first real relief in years.
The 2003 American Journal of Gastroenterology paper that formalized these findings became one of the most-cited pieces of IBS research of the decade. It also ignited a debate that is still simmering — because not every group has been able to reproduce the 60–80% figure. Later studies using glucose breath tests (which sample only the proximal small bowel) landed closer to 30–40%. Study design, test choice, and diagnostic cutoffs all matter.
Cause, Consequence, or Co-Traveler?
There are three camps in the medical literature, and they still argue at conferences.
Camp 1 — SIBO causes IBS. This is the Pimentel position. If you fix the overgrowth, the syndrome resolves; therefore the bacteria were driving the symptoms all along. Antibiotics help because they treat the actual disease.
Camp 2 — SIBO is a downstream consequence. In this view the underlying problem is slow or disordered motility in the small intestine, perhaps autoimmune. Bacteria accumulate because the small bowel is not sweeping itself clean. Kill the bacteria and they come back, because the motility defect is still there.
Camp 3 — It is a co-traveler, not the same disease. Some IBS is truly about visceral hypersensitivity and the brain-gut axis (see the visceral hypersensitivity article). Some is post-infectious autoimmunity. Some is pelvic-floor dyssynergia. SIBO is one of several overlapping conditions, not the umbrella diagnosis.
The practical truth is probably that all three camps are partially right for different patients. That is exactly why breath testing matters — it tells you which camp you belong in, so the treatment can follow the biology instead of guessing.
When to Get a Breath Test
You are a reasonable candidate for a SIBO breath test if you have IBS-type symptoms plus one or more of these features:
- Bloating that dominates your day — a flat abdomen in the morning that distends dramatically by afternoon, often visibly, often painfully.
- Symptoms that flare within 30–90 minutes of eating, especially carbohydrate-rich meals.
- Diarrhea with foul gas (suggests hydrogen-sulfide overgrowth).
- Unexplained constipation, particularly slow-transit constipation that does not respond to fiber or standard laxatives (suggests methane/IMO).
- A known risk factor: past food poisoning, abdominal surgery, opiate use, proton-pump-inhibitor use over months or years, hypothyroidism, diabetes, scleroderma, or a diagnosis of POTS or Ehlers-Danlos.
- A previous good-enough trial of standard IBS therapy (fiber, antispasmodic, low-FODMAP, an SSRI/TCA) that did not work.
You can order a breath test through a gastroenterologist or directly through an at-home kit. The two most widely used U.S. labs are Aerodiagnostics (lactulose and glucose two-gas tests) and Gemelli Biotech's Trio-Smart (a three-gas test measuring hydrogen, methane, and hydrogen sulfide — the only commercial test for the third gas). In-clinic testing is also available at many GI practices and hospital GI labs; the logistics are identical, just the kit sits in a clinic rather than your kitchen.
How the Test Actually Works
The principle is simple. Bacteria in your small intestine ferment carbohydrate. The gases they produce — hydrogen, methane, and hydrogen sulfide — are absorbed into the bloodstream, carried to the lungs, and exhaled. If you drink a standardized sugar and then measure breath gas every 15–20 minutes, you get a time-course that shows when and how much gas is being produced along your gut.
Two substrates are in common use:
- Lactulose — a non-absorbable sugar that travels the full length of the small bowel. Better for detecting distal overgrowth. More prone to false positives from rapid transit reaching the colon.
- Glucose — absorbed in the first 60–90 cm of the small bowel. More specific for proximal overgrowth but misses distal disease.
The collection window is 2 to 3 hours, with samples every 15 or 20 minutes. Preparation matters: a 24-hour low-fermentable-carbohydrate prep the day before, a 12-hour overnight fast, no antibiotics for four weeks prior, no probiotics or laxatives for a week, no smoking or exercise the morning of the test. Skip the prep and your result is unreadable.
Interpreting Your Results
The 2017 North American Consensus (Rezaie and colleagues, American Journal of Gastroenterology) set the cutoffs most modern labs use:
- Hydrogen-positive SIBO — a rise of ≥20 ppm above baseline within 90 minutes of substrate ingestion.
- Intestinal methanogen overgrowth (IMO) — any methane value ≥10 ppm at any time point. Methane does not need a "rise" the way hydrogen does; methanogens are slow and steady producers, so a flat elevated line counts.
- Hydrogen sulfide (Trio-Smart only) — a rise of ≥3 ppm, or a flat-line elevation pattern. Often correlates with severe diarrhea and foul-smelling gas.
A "double peak" pattern on a lactulose test — an early peak in the small bowel and a later peak in the colon — was once taught as the classic SIBO signature. The 2017 consensus largely dropped the two-peak requirement and moved to the simpler 20-ppm/90-minute rule because the double peak was inconsistent and hard to score reliably.
Why IBS-D Maps to Hydrogen and IBS-C Maps to Methane
This is the piece that makes the biology click. Hydrogen is produced by many kinds of bacteria. When hydrogen builds up in the small bowel, it increases osmotic pull, accelerates transit, and — combined with the bacterial metabolites that go with it — causes watery, urgent diarrhea with bloating. Hence the IBS-D pattern.
Methane is produced by a single dominant group of microbes — archaea, primarily Methanobrevibacter smithii. Methane is itself a motility inhibitor. Animal and human studies have shown that methane gas slows small-bowel and colonic transit, contributing to constipation. The more methane on your breath test, the slower your gut tends to move. This is why IBS-C so often maps to methane/IMO — the gas is not a side effect of the constipation, it is part of what causes it.
Hydrogen sulfide is the newest of the three. It is produced by sulfate-reducing bacteria and by the breakdown of sulfur-containing foods (eggs, garlic, cruciferous vegetables). Clinically it tracks with diarrhea and the "rotten egg" gas that patients describe with embarrassment. It was invisible to testing until Trio-Smart launched in 2020.
Rifaximin in IBS-D — The TARGET Trials
The single most important set of IBS-D treatment data of the past 20 years is the TARGET program — three large randomized controlled trials of rifaximin. TARGET-1 and TARGET-2 were published together in The New England Journal of Medicine in 2011. TARGET-3 followed.
The protocol is straightforward: rifaximin 550 mg orally three times a day for 14 days. Rifaximin is a non-absorbed antibiotic — over 99% of the dose stays in the gut lumen, so systemic side effects are minimal. In TARGET-1 and TARGET-2, roughly 40–41% of rifaximin-treated patients reported adequate relief of global IBS symptoms in the month after treatment, versus 31–32% on placebo. Bloating response was similar. The drug received FDA approval for IBS-D on the strength of these data.
TARGET-3 then answered the harder question: what happens when symptoms come back? The trial showed that repeat rifaximin courses worked in patients who had responded to the first course, and the effect held up over multiple cycles. That is the realistic clinical pattern for most IBS-D patients with hydrogen-positive breath tests — responders respond again, typically several months between courses.
Cost is the real-world obstacle. Branded Xifaxan in the United States runs roughly $2,000–$2,500 for a 14-day course. With prior authorization (usually after documenting IBS-D plus a failed trial of standard therapy) most major insurers cover it. Manufacturer copay programs and international pharmacies can cut costs substantially for uninsured patients. See the rifaximin protocols article for dosing details, insurance tactics, and combination regimens.
Treating Methane-Dominant IMO
Methane responds differently. Rifaximin alone clears methane in only a minority of IMO patients because archaea are genetically and metabolically distinct from bacteria. The standard regimen for methane-positive overgrowth is rifaximin 550 mg TID + neomycin 500 mg BID for 14 days. Neomycin targets the archaea that rifaximin alone leaves behind. Response rates in the IMO literature hover around 85% for the combination versus 30–40% for rifaximin monotherapy.
An alternative to neomycin is metronidazole 250–500 mg TID for 14 days, often chosen because it is cheaper and more easily prescribed. Some clinicians pair rifaximin with allicin (a concentrated garlic extract) as a natural antimicrobial with anti-archaeal activity. Both approaches have supportive case series but less trial data than the rifaximin-neomycin pairing.
For details on herbal antimicrobials as a standalone or adjunctive approach, see the herbal antimicrobials article. For the nuclear option — an elemental diet — see the elemental diet article.
When to Treat the SIBO vs. Treat the IBS
If your breath test is positive and your symptoms match, treating the SIBO first is usually the right move — and sometimes the IBS dissolves entirely once the overgrowth is gone. But not always. Three realistic scenarios:
Scenario A — SIBO treatment fixes everything. Roughly a third of breath-test-positive IBS patients get a complete or near-complete response to a properly dosed rifaximin course and stay well for months. These are the clearest wins. The diagnosis was SIBO; the IBS label was a placeholder.
Scenario B — SIBO treatment helps a lot but not completely. The bloating drops, the diarrhea eases, but residual pain and urgency remain. This is very common. It means you have two things going on — the overgrowth and an underlying visceral-hypersensitivity or brain-gut component. You still need the standard IBS toolkit: low-FODMAP (see the low-FODMAP guide), an antispasmodic or peppermint oil, gut-directed hypnotherapy, maybe a low-dose TCA.
Scenario C — SIBO treatment helps little. Either the test was a false positive, or your symptoms were never primarily SIBO-driven. Pivot back to IBS-focused treatment and do not keep pounding antibiotics at a target that is not there.
Finding the Root Cause
If you have SIBO, you got it for a reason. The single most productive question in a SIBO work-up is why. The leading root causes (covered in depth in the SIBO root causes article):
- Post-infectious autoimmunity. An episode of food poisoning triggers antibodies against a bacterial toxin called CdtB. Because CdtB resembles a human protein called vinculin that lives in the interstitial cells of Cajal (the pacemaker cells of the gut), the immune system cross-reacts and damages your own motility machinery. The Cedars-Sinai team developed the anti-CdtB and anti-vinculin blood test (ibs-smart) to identify this subtype. Anywhere from a third to two-thirds of IBS-D cases appear to be post-infectious. See the post-infectious IBS article.
- Migrating motor complex (MMC) dysfunction. The MMC is the "housekeeper wave" that sweeps the small intestine clean between meals. When it is weak or absent, bacteria accumulate. The MMC is damaged by post-infectious autoimmunity, opiates, and chronic stress.
- Ileocecal valve dysfunction. A leaky or incompetent valve between small bowel and colon lets colonic bacteria back-flow upstream.
- Adhesions and structural issues. Scarring from surgery, endometriosis, or inflammatory bowel disease can create pockets where bacteria stagnate.
- Hypothyroidism. Low thyroid slows gut transit. Correcting thyroid levels often reduces SIBO recurrence.
- Scleroderma and other connective-tissue diseases. Smooth-muscle damage in the small bowel leads to severe, relapsing SIBO that is notoriously hard to clear.
- Chronic PPI use. Stomach acid is an important bacterial filter. Long-term acid suppression removes that filter.
Identifying your root cause does not always give you a clean fix, but it tells you what you are up against and which long-term strategies matter.
Realistic Expectations — Why Relapse Is the Rule
Here is the part that patients deserve to hear up front: roughly half of successfully treated SIBO patients relapse within 9–12 months. The published figure in the long-term follow-up literature is about 44% at nine months. In patients with a strong post-infectious or scleroderma root cause, the relapse rate is higher. In patients with a modifiable cause (PPI use, opiates, hypothyroidism) that gets fixed, the relapse rate is much lower.
Relapse is not failure. It is the natural history of a condition whose root cause — usually a motility problem — has not been cured, only treated. The goal of long-term management is to stretch the interval between treatments and to reduce symptom burden in between. The tools that do that work:
- Prokinetics. Low-dose medications that restore the migrating motor complex. Prucalopride (2 mg nightly), low-dose erythromycin (50–100 mg nightly), or low-dose naltrexone are the mainstays. Taken nightly, they measurably reduce relapse rates. See the prokinetics article.
- Meal spacing. Four to five hours between meals, no constant snacking. The MMC only runs when you are not eating.
- Targeted diet. A moderately-reduced-fermentable-carb diet (not lifelong strict low-FODMAP) during symptom flares.
- Root-cause maintenance. Optimize thyroid, come off chronic PPIs if possible, address adhesions, keep moving.
Why You Should Not Cycle Antibiotics Forever
It is tempting, after the first rifaximin course works, to simply re-run it every time symptoms come back. Some patients do exactly that for years. The problem is that antibiotic cycling without root-cause work has diminishing returns.
With each round, you are dosing the same bacteria with the same drug. Resistance is not yet a large-scale problem with rifaximin because so little is absorbed, but response rates do tend to slip for some patients over multiple cycles. More importantly, you are spending thousands of dollars and disrupting your microbiome repeatedly to treat a condition whose driver — a motility defect or an immune-mediated process — you have never addressed. The same reason it came back last time is the reason it will come back next time.
The smart approach is to pair any antibiotic course with two parallel efforts: identify the root cause (post-infectious serology, thyroid, structural imaging if indicated) and start a prokinetic after the course finishes. Patients who do both stretch their remission intervals from months to years. Patients who just re-run antibiotics stay stuck in a three-month cycle.
If you have done three cycles and you are still relapsing fast, that is the signal to stop cycling and dig for the root cause with a gastroenterologist who does this work seriously — not to request a fourth course.
Key Research Papers
- Pimentel M, Chow EJ, Lin HC. Normalization of lactulose breath testing correlates with symptom improvement in irritable bowel syndrome: a double-blind, randomized, placebo-controlled study. Am J Gastroenterol. 2003.
- Pimentel M, et al. Rifaximin therapy for patients with irritable bowel syndrome without constipation (TARGET-1 and TARGET-2). N Engl J Med. 2011.
- Rezaie A, et al. Hydrogen and methane-based breath testing in gastrointestinal disorders: the North American Consensus. Am J Gastroenterol. 2017.
- Pimentel M, et al. Development and validation of a biomarker for diarrhea-predominant irritable bowel syndrome in human subjects (anti-CdtB and anti-vinculin). PLoS One. 2015.
Live PubMed Searches
For further reading, the following PubMed topic searches return current peer-reviewed work on the IBS–SIBO overlap, breath testing, and treatment:
- IBS and SIBO breath testing
- Rifaximin and the TARGET trials
- Methane, constipation, and intestinal methanogen overgrowth
- Hydrogen sulfide SIBO and diarrhea
- Anti-CdtB, anti-vinculin, and post-infectious IBS
- Migrating motor complex and SIBO
- Prokinetics and SIBO relapse prevention
- Lactulose vs. glucose breath testing for SIBO
Connections
- Gastroenterology
- The Gut Barrier & Your Microbiome — interactive animation
- Irritable Bowel Syndrome
- SIBO
- Elemental Diet
- SIBO Root Causes
- Herbal Antimicrobials
- Rifaximin Protocols
- Prokinetics and Relapse Prevention
- Low-FODMAP Diet for SIBO
- SIBO Breath Test Guide
- Hydrogen vs Methane vs Hydrogen Sulfide
- Post-Infectious IBS
- Rome IV Subtypes
- Low-FODMAP Diet for IBS
- Visceral Hypersensitivity and Brain-Gut Axis
- IBS Medications Guide
- POTS
- Constipation
- Bloating