Postural Orthostatic Tachycardia Syndrome (POTS): The Autonomic Syndrome Everyone Is Finally Talking About
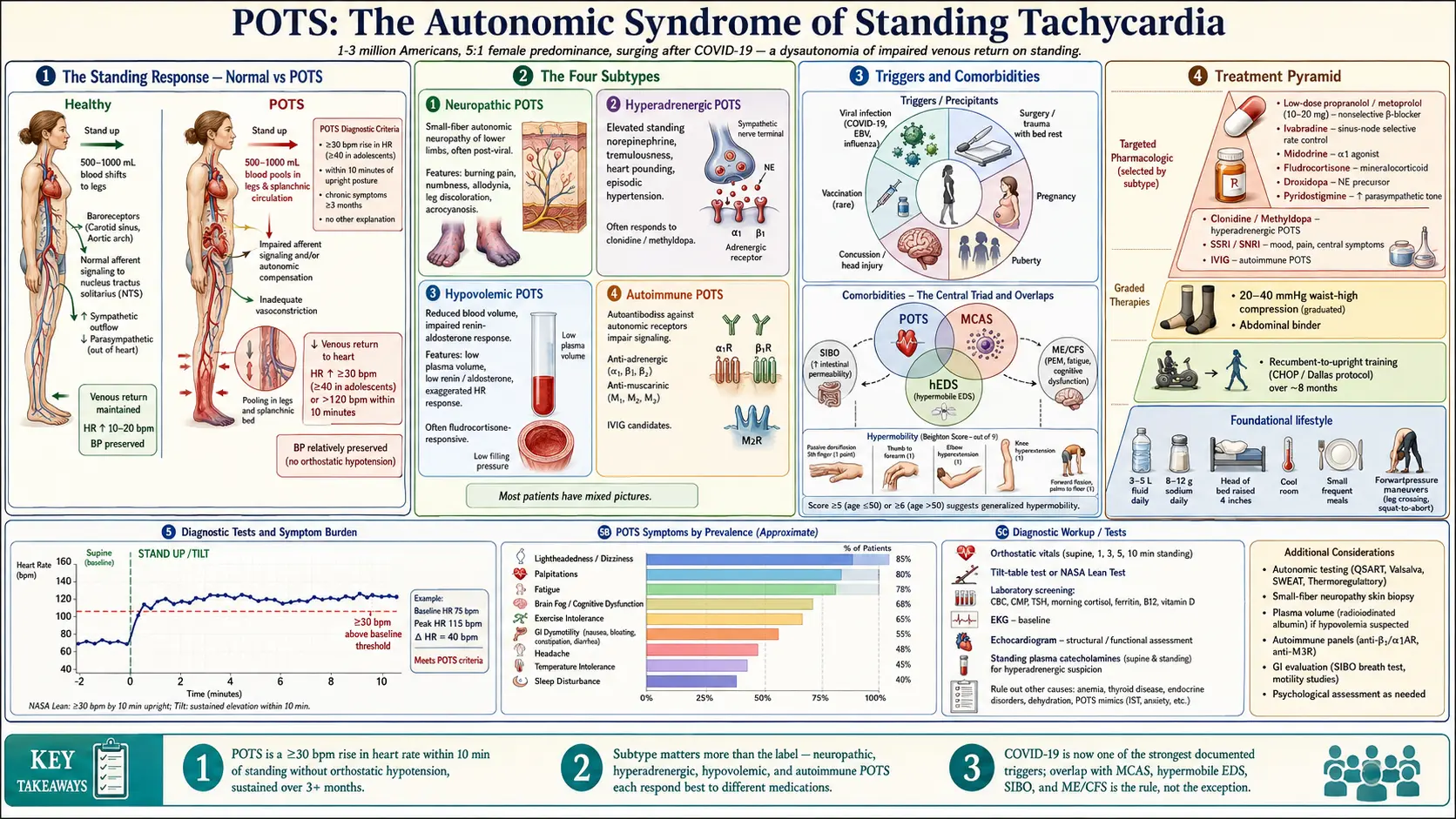

Postural orthostatic tachycardia syndrome (POTS) is a form of dysautonomia characterized by an abnormal increase in heart rate upon standing, accompanied by symptoms such as lightheadedness, palpitations, fatigue, cognitive impairment, and exercise intolerance. Estimates suggest 1 to 3 million Americans have POTS, with a sharp female predominance (5:1 to 10:1) and typical onset in the second to fourth decade. Diagnoses surged following COVID-19, which is now recognized as one of the strongest known triggers.
Deep-Dive Articles
POTS is complicated, and generic advice rarely gets anyone better. The eight guides below each tackle one piece of the puzzle — the subtype you actually have, the tests that confirm it, the daily protocols that move the needle, the medications that help and the ones that don’t, and the overlap conditions (MCAS, Ehlers-Danlos) you may also need to investigate. Start with whichever piece matches where you are right now.
POTS Subtypes
Hyperadrenergic, neuropathic, and hypovolemic POTS explained in plain language. Each one has different root causes and different best treatments — knowing your subtype is the single most useful thing you can learn about your own POTS.
Tilt Table & NASA Lean Test
What to expect during a tilt table test, how to do the at-home NASA Lean Test if you can’t get a specialist appointment, how to read the heart-rate/blood-pressure curve, and why the timing matters.
Salt & Hydration Protocol
The 10g sodium / 2–3 L fluid target — why it works, how to actually hit it without feeling sick, homemade ORS recipes, commercial options (Liquid IV, LMNT, Normalyte), and when salt tablets beat food-based salt.
Compression & Exercise Program
Compression garments (abdominal binders vs. thigh-high stockings), and the CHOP/Dallas recumbent exercise protocol that reverses deconditioning without triggering post-exertional crashes. Week-by-week progression.
Medications Guide
Beta-blockers vs. ivabradine vs. midodrine vs. fludrocortisone vs. pyridostigmine — what each one does, who it helps, the tradeoffs, typical dosing, and how they stack. The honest medication map most doctors don’t have time to explain.
POTS/MCAS/EDS Triad
If you’re flexible, bloated, and dizzy, you may have all three. How to recognize the triad, the Beighton hypermobility score, when to screen for mast cell activation, and why treating only one condition often fails.
Low-Dose Naltrexone for POTS
The 1.5–4.5 mg bedtime protocol that’s quietly become one of the most-used off-label POTS treatments. How it works (microglial modulation, not opioids), titration, cost, and what the case-series evidence actually shows.
Vagus Nerve & Autonomic Retraining
Cold-water face dunks, humming, slow diaphragmatic breathing, DNRS and Primal Trust brain-retraining programs. The non-pharmaceutical lane — cheap, safe, and for many people genuinely effective.
Diet: Small Frequent Meals & Postprandial Crashes
Splanchnic pooling, low-GI carbs, electrolytes, and meal timing for POTS.
What POTS Is
When a healthy person stands up, roughly 500–1000 mL of blood shifts toward the legs. Baroreceptors detect the transient drop in blood return, and the autonomic nervous system compensates through vasoconstriction and a modest rise in heart rate (10–20 bpm). In POTS this response is exaggerated: heart rate rises by 30 bpm or more (or to >120 bpm) within 10 minutes of standing, without a substantial drop in blood pressure. The body is functionally struggling to keep blood returning to the heart and brain when upright.
Diagnostic Criteria
- Heart rate increase of ≥30 bpm (≥40 in adolescents aged 12–19) within 10 minutes of standing or head-up tilt, OR sustained heart rate >120 bpm.
- Without orthostatic hypotension (no drop of >20/10 mmHg).
- Chronic symptoms of orthostatic intolerance for at least 3 months.
- Absence of another explanation such as dehydration, medications, or primary autonomic failure.
Symptoms
- Lightheadedness, pre-syncope, occasional syncope
- Palpitations
- Exercise intolerance
- Fatigue (often profound)
- Brain fog and concentration difficulty
- Headache
- Nausea and GI dysmotility
- Temperature intolerance, flushing
- Pooling of blood in legs with standing — blue/purple discoloration
- Tremulousness, anxiety-like symptoms
- Sleep disturbance
- Menstrual worsening of symptoms
Subtypes
- Neuropathic POTS. Small-fiber autonomic neuropathy with impaired lower-extremity vasoconstriction. Often post-viral.
- Hyperadrenergic POTS. Elevated standing norepinephrine, tremulousness, episodic hypertension.
- Hypovolemic POTS. Reduced blood volume with impaired renin-aldosterone response.
- Autoimmune POTS. Antibodies against adrenergic or muscarinic receptors; overlap with autoimmune conditions.
- Most patients have mixed pictures.
Triggers
- Viral infection — COVID-19, Epstein-Barr virus, influenza, and others.
- Surgery or trauma, particularly with prolonged bed rest.
- Pregnancy.
- Puberty — many cases emerge in teens.
- Concussion or head injury.
- Ehlers-Danlos/hypermobility spectrum disorders — common overlap.
- Vaccination — rare but documented.
Clinical Evaluation
- Detailed orthostatic vitals or 10-minute active stand test.
- Tilt-table test (gold standard) for definitive diagnosis or atypical cases.
- CBC, CMP, TSH, cortisol (to exclude adrenal insufficiency), ferritin, B12, vitamin D.
- EKG and echocardiogram to exclude structural heart disease.
- Standing catecholamines in hyperadrenergic subtype.
- Assessment for mast-cell activation, autoimmunity, and hypermobility where clinical suspicion warrants.
Treatment
- Volume expansion. 3–5 L fluid daily, 8–12 g sodium per day (if no contraindication).
- Compression garments. Waist-high 20–40 mmHg compression reduces venous pooling substantially.
- Beta-blockers. Low-dose propranolol or metoprolol for tachycardia.
- Ivabradine. Selective sinoatrial-node blocker, particularly effective in inappropriate sinus tachycardia overlap.
- Midodrine. Alpha-1 agonist increasing vascular tone.
- Fludrocortisone. Mineralocorticoid for volume expansion.
- Droxidopa. Synthetic norepinephrine precursor.
- Pyridostigmine. Enhances parasympathetic tone.
- Clonidine or methyldopa in hyperadrenergic subtype.
- SSRIs/SNRIs in some cases.
- IVIG or immune modulation in autoimmune POTS.
Lifestyle and Daily Strategies
- Reclined aerobic exercise — recumbent bike, rowing, or swimming — to rebuild cardiovascular conditioning without triggering upright symptoms. The Dallas/CHOP protocols specifically use 3–6 months of graded reclined exercise.
- Raise head of bed by 4 inches to reduce morning symptoms.
- Counterpressure maneuvers — leg crossing, squatting — to abort presyncope.
- Cool room temperature, avoid hot showers and saunas.
- Small, frequent meals to avoid postprandial pooling.
- Pacing analogous to ME/CFS if post-exertional worsening is present.
Table of Contents
- Deep-Dive Articles
- What POTS Is
- Diagnostic Criteria
- Symptoms
- Subtypes
- Triggers
- Clinical Evaluation
- Treatment
- Lifestyle and Daily Strategies
- Research Papers
- Connections
- Featured Videos
Research Papers
Curated PubMed topic searches on POTS (Postural Orthostatic Tachycardia Syndrome). Each link opens a live PubMed query so the result set stays current as new studies are indexed.
- PubMed topic search: Postural orthostatic tachycardia syndrome review
- PubMed topic search: POTS diagnostic criteria consensus
- PubMed topic search: POTS hyperadrenergic
- PubMed topic search: POTS neuropathic hypovolemic
- PubMed topic search: Tilt table test POTS
- PubMed topic search: Midodrine POTS
- PubMed topic search: Ivabradine POTS
- PubMed topic search: Fludrocortisone POTS
- PubMed topic search: Ehlers-Danlos POTS
- PubMed topic search: Compression garments orthostatic
- PubMed topic search: POTS salt fluid loading
- PubMed topic search: POTS dysautonomia review
Connections
- POTS Subtypes
- POTS/MCAS/EDS Triad
- Medications Guide
- Compression & Exercise
- Salt & Hydration
- Vagus Nerve & Retraining
- LDN for POTS
- Tilt Table Test
- POTS Diet
- MCAS
- ME/CFS
- Ehlers-Danlos Syndrome
- Fibromyalgia
- Hashimoto's Thyroiditis
- SIBO
- Lightheadedness on Standing
- Brain Fog
- Magnesium