MCAS Triggers and Flare Management
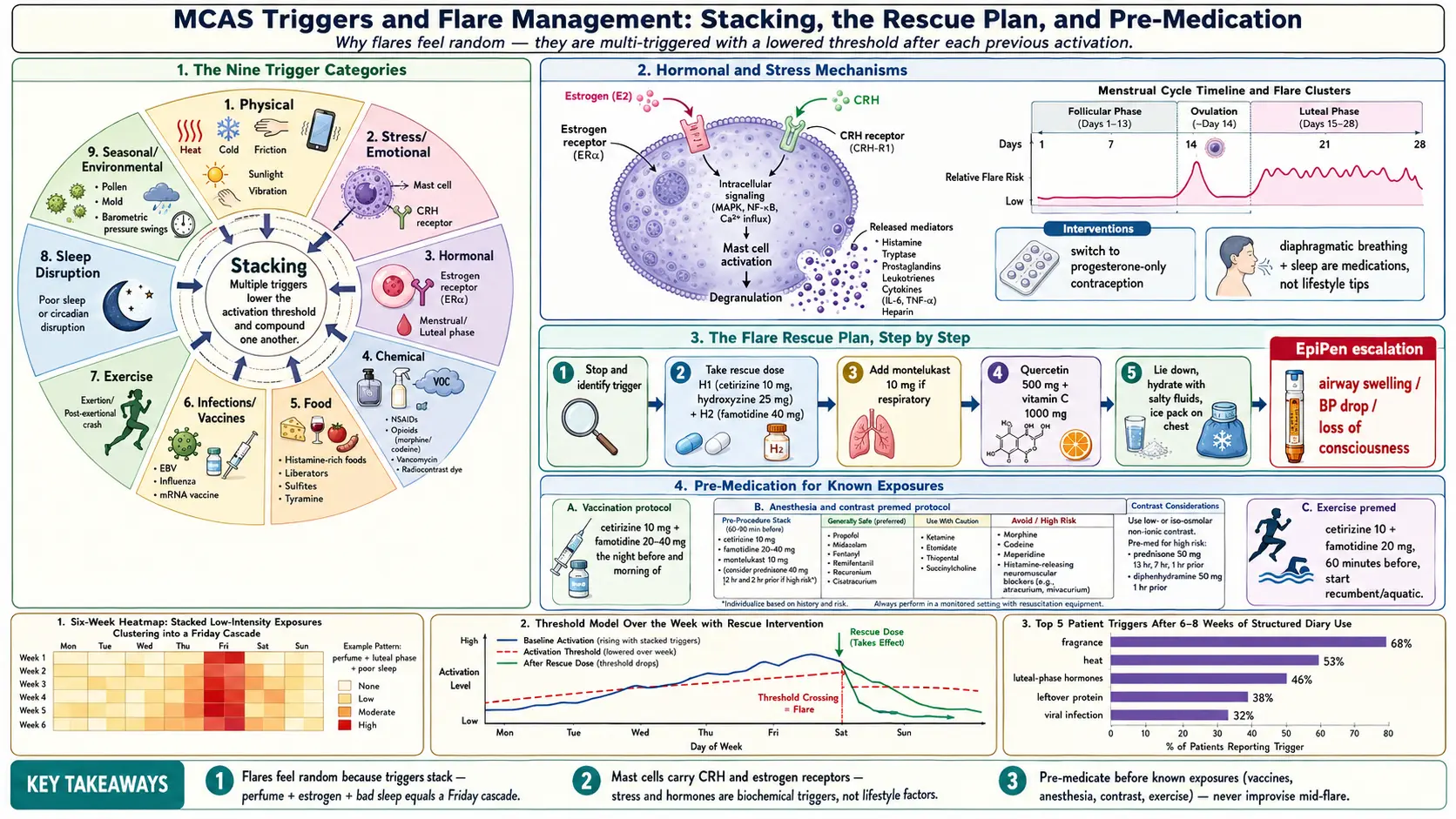
Table of Contents
- Triggers Aren’t Random
- Categories of MCAS Triggers
- Physical Triggers
- Stress & Emotional Triggers
- Hormonal Triggers
- Chemical Triggers
- Food & Drink Triggers
- Infections & Vaccines
- Exercise Triggers
- Sleep Disruption as a Trigger
- Building a Trigger Diary That Works
- The Flare Rescue Plan — Step-by-Step
- When to Use an EpiPen
- Pre-Medication Strategies for Known Trigger Events
- Chronic Baseline Management to Reduce Flare Frequency
- When to Escalate Care
- Key Research Papers
- Research Papers
- Connections
- Featured Videos
1. Triggers Aren’t Random
If your flares feel like they come out of nowhere, you are not imagining things — but you are also not right. MCAS flares almost always have patterns. The reason they feel random is that MCAS is multi-triggered, and mast cells that have already released mediators from one trigger have a lowered threshold for the next one. A perfume on Monday that would normally cause a minor flush can, layered on top of pre-menstrual estrogen and a poor night’s sleep, produce a full-body cascade on Friday.
This stacking is the core insight. Any single exposure might look harmless; it is the combination that tips you over. After a few weeks of careful, honest diary-keeping, the repeat offenders start to emerge. Most patients discover their top three to five triggers within six to eight weeks.
This article is the toolkit: how to catalog your triggers, how to build a diary that actually reveals your pattern, and a step-by-step flare rescue plan to use before and during an episode.
2. Categories of MCAS Triggers
Before the deep dives, here is the full map. Almost every MCAS trigger falls into one of these nine buckets.
- Physical — heat, cold, friction, pressure, sunlight, vibration
- Emotional / stress — acute arguments, performance anxiety, chronic stress load
- Hormonal — menstrual cycle, ovulation, pregnancy, peri-menopause, HRT
- Chemical — perfumes, cleaning products, medications, preservatives, fragrances, VOCs
- Food and drink — histamine-rich, histamine liberators, sulfites, tyramine
- Infections and vaccines — viral illnesses, mRNA and live vaccines, gut dysbiosis
- Exercise and exertion — including food-dependent exercise-induced anaphylaxis
- Sleep disruption — one bad night raises next-day activation
- Seasonal / environmental — pollen, mold, humidity, barometric pressure swings
3. Physical Triggers
Heat
Hot showers, saunas, summer heat, hot tubs, and even the fevers of minor infections all activate mast cells directly through thermal signaling. Many MCAS patients can time a flushing episode to the minute a hot shower starts.
Interventions: switch to tepid showers, avoid saunas, stay indoors during peak summer heat, and keep your home thermostat below 72°F. Cooling vests and neck-wrap ice packs are worth their weight in gold on bad-weather days.
Cold
Conversely, ice-water contact, winter wind, and abrupt temperature changes trigger cold-activated mast cells (cold urticaria is a well-recognized subtype). Dunking your face in ice water for vagus-nerve stimulation — a technique that helps POTS patients — can backfire badly in MCAS.
Interventions: layered clothing, warm-up period before cold exposure, gloves in freezer aisles, and a gradual acclimation rather than sudden shocks.
Friction and Pressure (Dermographism)
Tight waistbands, bra straps, backpacks, and even a firm massage can trigger cutaneous mast cells in patients with dermographism. Sexual activity is a common and under-discussed trigger.
Interventions: loose clothing, elastic-free waistbands, soft seamless bras, avoid deep-tissue massage until baseline is stable.
Sunlight (Solar Urticaria)
UV light directly activates a subset of cutaneous mast cells. Some patients can tolerate shade but flare within minutes of direct sun.
Interventions: broad-spectrum zinc oxide sunscreen, UV-blocking clothing (UPF 50+), wide-brimmed hats, and disciplined shade practice.
Vibration
Power tools, motorcycles, lawn mowers, and certain vibrating exercise platforms can trigger vibratory angioedema in susceptible patients. If your symptoms track with yard work or a particular commute, vibration deserves a line in the diary.
4. Stress & Emotional Triggers
Stress is not a character flaw in MCAS — it is a biochemical trigger. Acute stress releases corticotropin-releasing hormone (CRH), and mast cells carry CRH receptors on their surface. That receptor is well-documented; activating it degranulates the cell directly. Arguments, job interviews, public speaking, and even anticipation of a medical appointment are all documented precipitants.
Chronic stress is worse in a different way: it keeps baseline mast cell activation elevated, so every other trigger packs a bigger punch.
Interventions: slow diaphragmatic breathing (see Vagus Nerve and Autonomic Retraining), meditation, trauma-informed therapy, and an uncompromising approach to sleep. None of these are “nice-to-haves” — in MCAS they are medications.
5. Hormonal Triggers
Mast cells carry estrogen receptors, and estrogen amplifies mediator release. This is the mechanism behind why the majority of MCAS patients are women, and why flares cluster at predictable points in the cycle.
Expect worse symptoms in the luteal phase (the week before menstruation), at ovulation, in pregnancy (especially first trimester), during peri-menopause when estrogen swings wildly, and on estrogen-containing HRT or birth control.
Interventions: discuss with your gynecologist switching to progesterone-only contraceptives such as the Mirena IUD or norethindrone, avoid systemic estrogen where possible, and time supplement and medication escalations so that a new agent is on board before the luteal phase begins.
6. Chemical Triggers
Fragrances are the most universal MCAS trigger of all. Perfumes, scented candles, dryer sheets, plug-in air fresheners, and scented personal care products are all mast-cell degranulators in sensitive patients. Cleaning chemicals (bleach, ammonia), off-gassing from new carpet and furniture, airborne mold spores, and VOCs round out the list.
High-Risk Medications
Several drug classes are direct histamine liberators or known mast cell degranulators. Any one of them can precipitate a severe flare.
- NSAIDs (ibuprofen, naproxen) — aspirin is paradoxically tolerated by some patients and actively helpful, but introduce only with supervision
- Opioids, especially morphine and codeine — classic histamine liberators
- Succinylcholine — used in anesthesia
- Vancomycin — causes “red man syndrome” through direct mast cell activation
- Radiocontrast dye — CT with contrast, angiograms
- General anesthesia agents — always pre-medicate with antihistamines
Interventions: a fragrance-free household, HEPA air purifiers in bedroom and living areas, and a pre-anesthesia protocol letter from your physician that you carry to every procedure. The letter should list your MCAS diagnosis, your safe and unsafe medications, and the premedication regimen required before any anesthesia or contrast.
7. Food & Drink Triggers
Food triggers deserve their own article — see Low-Histamine Diet. Briefly, four overlapping food categories cause trouble:
- Histamine-rich foods — aged cheese, cured meats, fermented foods (sauerkraut, kombucha, vinegar), and anything left over. Histamine accumulates in protein foods from the moment they are cooked.
- Histamine liberators — tomato, strawberry, pineapple, citrus, chocolate, alcohol. These do not contain histamine themselves but cause mast cells to release it.
- Preservatives — sulfites in wine, dried fruit, and restaurant salads; benzoates; nitrates; MSG
- Tyramine-rich foods — aged cheese, cured meats, fava beans. Tyramine triggers a similar cascade and often overlaps with histamine sources.
The single highest-yield food rule: do not eat protein leftovers. Cook, eat, freeze immediately.
8. Infections & Vaccines
Viral infections — EBV, influenza, even the common cold — trigger a mast cell surge that can last for days to weeks after the acute illness resolves. Many MCAS patients trace their initial diagnosis to a specific viral illness that “never quite went away.”
Vaccines commonly trigger flares, especially mRNA and live vaccines. This is not an argument against vaccination — it is an argument for planned pre-medication. Work with your allergist on a protocol: typically cetirizine 10 mg + famotidine 20–40 mg the night before and morning of, sometimes with hydroxyzine 25 mg for higher-risk patients, and where possible choose staggered single-component vaccinations rather than combination shots.
Chronic gut dysbiosis is a persistent, often-invisible trigger. Lipopolysaccharide (LPS) from gram-negative bacteria and other bacterial metabolites continuously prime mast cells through the gut-immune axis. If you have unexplained, unrelenting baseline activation, investigate SIBO and broader dysbiosis.
9. Exercise Triggers
Exercise is a paradoxical territory: gentle movement calms mast cells in the long run, but acute exertion can trigger them in the short run. Two distinct patterns matter.
Exercise-Induced Anaphylaxis
Rare but serious. Often food-dependent (FDEIA): anaphylaxis occurs only when the patient exercises within 2–4 hours of eating a specific food, most commonly wheat or shellfish. Neither the food alone nor the exercise alone triggers the reaction — only the combination does. If you have had a mystery anaphylaxis after a run or a bike ride, ask about FDEIA testing.
Post-Exertional Mast Cell Activation
A delayed flare appearing 12–48 hours after a workout, often mimicking a POTS crash: fatigue, brain fog, flushing, headache, GI upset. This is common in the MCAS/POTS/hEDS triad.
Interventions: pre-medicate 60 minutes before exercise with cetirizine 10 mg + famotidine 20 mg, start with recumbent or aquatic exercise (swimming, recumbent bike), avoid known food-exercise combos, and keep sessions short until you know your threshold.
10. Sleep Disruption as a Trigger
A single bad night raises next-day mast cell activation substantially. Patients who log their sleep often find that their “mystery flares” cluster on days following poor sleep.
Sleep hygiene for MCAS: cool bedroom below 68°F, blackout curtains, white noise, a consistent schedule (same bedtime and wake time, weekends included), no screens in bed, and a serious workup for sleep apnea if you snore or wake unrefreshed. CPAP-treated apnea reduces mast cell activation in patients who needed it.
11. Building a Trigger Diary That Works
The single highest-yield activity in MCAS management is a structured trigger diary. The problem is that most patients abandon theirs in a week because they set them up wrong.
Track for a minimum of six weeks before expecting patterns. Triggers stack across days; a pattern that takes four weeks to reveal itself will never show up in a seven-day log.
Variables to Log Every Day
- Date and time
- Symptoms and severity on a 0–10 scale
- Location (home, office, outdoors)
- Weather (temperature, humidity, barometric pressure)
- Menstrual cycle day
- Every food and drink in the last 4 hours
- Medications and supplements taken, with doses
- Stress level (0–10)
- Sleep quality and duration the night before
- Physical activity
- Chemical or fragrance exposures
Tools
Apps that work well: MCAS Tracker, Bearable, Waterlogue, or a structured paper diary if you prefer pen and paper. Cronometer pairs well with the SIGHI histamine list to estimate the total histamine load of each meal.
Review Weekly
On a fixed day each week, sit down and look for repeated correlations. Do not trust single incidents; trust patterns that appear three or more times. Over six to eight weeks, three to five top triggers almost always emerge for each individual patient.
12. The Flare Rescue Plan — Step-by-Step
Build this plan when you are well, print it, and tape it inside a kitchen cupboard. Nobody can reason through a rescue protocol while flaring.
Pre-Flare (you know something is coming)
You smell the perfume in the elevator, you are about to walk into a hot kitchen, you know a stressful meeting is in an hour. Pre-medicate 60 minutes before exposure: extra dose of cetirizine 10 mg + famotidine 20–40 mg, and if you run hot, hydroxyzine 25 mg. Diphenhydramine (Benadryl) 25–50 mg if the exposure is acute and unavoidable.
Early Flare (symptoms starting)
- Remove yourself from the exposure first — leave the scented room, stop eating the offending food
- Extra H1 antihistamine: cetirizine 10 mg or Benadryl 25–50 mg
- Extra H2 antihistamine: famotidine 20–40 mg
- Hydrate with a low-histamine electrolyte drink — flushing costs fluid
- Lie flat if orthostatic; many MCAS flares drop blood pressure
- Cool (not cold) shower if heat-triggered; warm blanket if cold-triggered
Moderate Flare (full symptom cascade)
- Layer on everything above
- Ketotifen or cromolyn rescue dose if prescribed
- Aspirin 325 mg if you are aspirin-tolerant and flushing is dominant
- Short course oral prednisone 20–40 mg if severe and you have it on hand from your physician
Severe Flare / Anaphylaxis
Throat swelling, severe wheeze, loss of consciousness, or blood pressure crash. EpiPen and 911 immediately. Do not wait. Epinephrine is safer than a delayed decision.
13. When to Use an EpiPen
Any one of the following is an indication to inject:
- Any airway swelling — tongue, lips, throat tightness, stridor
- Severe wheeze with hypotension
- Loss of consciousness
- Severe abdominal pain with vomiting and hypotension
- Rapidly progressing symptoms across two or more body systems
Err on the side of using it. The downside of an unnecessary injection is transient tachycardia; the downside of a missed one is death.
14. Pre-Medication Strategies for Known Trigger Events
Medical procedures, flights, weddings, big social gatherings, new restaurants — any predictable high-risk event deserves a written premedication plan.
- 24 hours prior: extra H1 antihistamine dose in the evening
- 1 hour prior: cetirizine 10 mg + famotidine 40 mg + hydroxyzine 10–25 mg
- Emergency supplies on your person: EpiPen (two, if possible), Benadryl 50 mg, hydrocortisone tabs if prescribed, a small bottle of water
Carry a card or phone note listing your diagnosis, safe and unsafe medications, and emergency contacts. Tell one person at the event about your MCAS before it starts.
15. Chronic Baseline Management to Reduce Flare Frequency
The best flare plan is fewer flares. Solid rescue protocols buy you safety; good baseline control buys you your life back.
Build the baseline step by step: see H1 and H2 Blocker Stacks, Cromolyn and Ketotifen Protocols, Low-Histamine Diet, and Natural Mast Cell Stabilizers. Layered together, a stable baseline can drop flare frequency by 50–80% within six months.
16. When to Escalate Care
Get back in front of your specialist when any of the following happens:
- Flares increasing in frequency, severity, or duration
- Any anaphylaxis episode, even a mild one that resolved on its own
- Poor response to a fully optimized baseline medication stack
- New symptoms suggesting autoimmune overlap (joint swelling, rash, new cytopenias)
- Unexplained weight loss, new GI bleeding, persistent fever
If your current clinician cannot help, seek an MCAS-literate immunologist or allergist. The field is small but growing, and the right specialist changes the trajectory of this disease.
17. Key Research Papers
- Afrin LB, et al. Diagnosis of mast cell activation syndrome: a global “consensus-2.” Diagnosis. 2020.
- Valent P, et al. Proposed diagnostic algorithm for patients with suspected mast cell activation syndrome. Journal of Allergy and Clinical Immunology. 2019.
- Afrin LB, et al. Characterization of mast cell activation syndrome presentations and treatments. Journal of Internal Medicine. 2017.
- Cardet JC, et al. Mast cell activation syndrome: a practical evidence-based review. Annals of Allergy, Asthma & Immunology. 2019.
18. Research Papers
Curated PubMed topic searches for MCAS triggers and flare management. Each link opens a live PubMed query.
- PubMed: MCAS triggers and flare
- PubMed: Mast cells and estrogen
- PubMed: Exercise-induced anaphylaxis
- PubMed: Food-dependent exercise-induced anaphylaxis
- PubMed: Mast cells and heat activation
- PubMed: MCAS and infection triggers
- PubMed: Pre-medication protocols for mast cell disease
Connections
- MCAS Overview
- Cromolyn & Ketotifen Protocols
- Natural Mast Cell Stabilizers
- H1 and H2 Blocker Stacks
- Low-Histamine Diet
- SIBO
- POTS
- Testing Guide
- Mediators & Symptom Map
- Hereditary Alpha-Tryptasemia
- Alpha-Gal Syndrome
- Allergies
- Vagus Nerve & Autonomic Retraining
- Sulfites
- Hormone Sensitivity: Estrogen & Menstrual Flares