Endo Belly and the Gut Connection
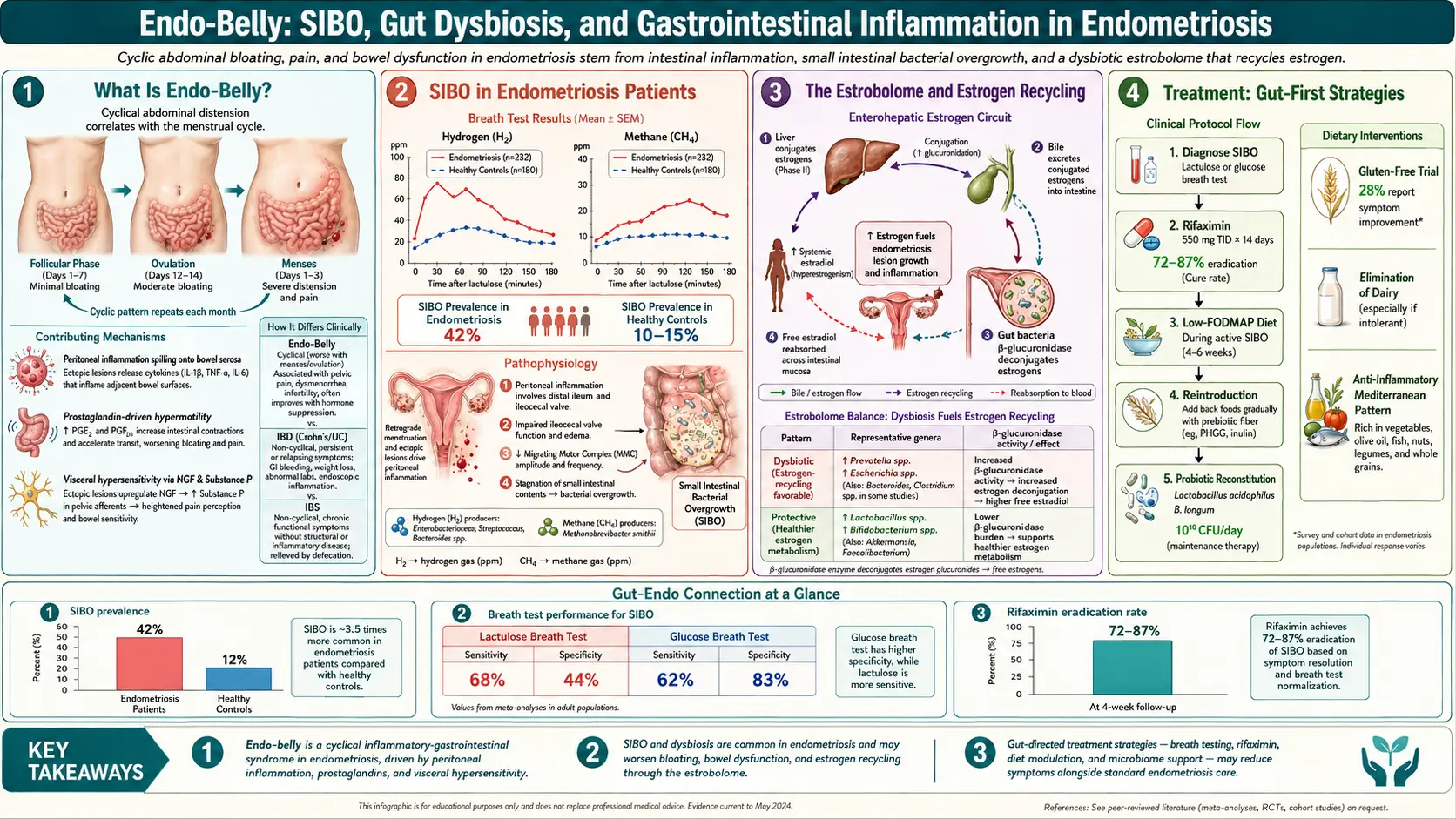
Table of Contents
- What “Endo Belly” Actually Is
- Why It Happens — The Short List
- Bowel Endometriosis
- SIBO — The Quiet Driver of Endo Belly
- The IBS Overlap
- The Gut–Endo Axis
- When Gut Symptoms Are the Primary Problem
- The Low-FODMAP Trial
- Anti-Inflammatory & Mediterranean Foundation
- Dairy Elimination Trial
- Gluten Elimination Trial
- Specific Foods Endo Patients Flag
- Fiber — Type Matters
- Digestive Support Tools
- Managing an Acute Endo-Belly Episode
- When to Investigate Gut Symptoms Separately
- The Pelvic Floor Contribution
- Key Research Papers
- Connections
- Featured Videos
What “Endo Belly” Actually Is
You wake up flat. By 8 PM your waistband is cutting into your skin, the mirror shows what looks like a second-trimester pregnancy, and coworkers have asked if you are expecting. You are not. You are having an endo-belly episode — not in your head, not a diet failure, not something you caused by eating too much. It is your gut responding to inflammation, hormones, and often a second gut condition riding on top of your endometriosis.
Endo belly is the colloquial name for the sudden, dramatic, painful abdominal distension that affects most people with endometriosis at some point. It is different from ordinary premenstrual bloat, which is a gradual one-to-two-pound shift in fluid. Endo belly is visible across the room. It appears within hours — sometimes within minutes of a trigger meal — and it resolves over the night or next day.
Typical features: worst in late afternoon or evening regardless of what you ate; the skin feels stretched and any pressure (waistbands, seatbelts, hugs) hurts; crampy, gassy pain that can radiate to the lower back; duration hours to days, sometimes a full week around menstruation. It is separate from ovulatory bloating (mid-cycle, milder) and premenstrual water retention (diffuse, not concentrated). When distension is this severe and this variable, the mechanism is gas and gut inflammation, not body fat and not “stress.”
Why It Happens — The Short List
Endo belly is multifactorial. No single cause explains every episode in every patient. The drivers that show up most often in the literature and in clinical experience:
- Cytokine-driven gut edema. Circulating inflammatory mediators (TNF-α, IL-6, IL-8, prostaglandin E2) increase intestinal permeability and leak fluid into the bowel wall. The gut literally swells.
- Autonomic dysfunction. Endo disturbs pelvic autonomic nerves. Vagal tone drops, sympathetic drive rises, motility slows. Slower motility means more fermentation and more gas.
- Pelvic floor dysfunction. Chronic pain drives the pelvic floor into a shortened, guarded state. A hypertonic puborectalis prevents the anorectal angle from opening during defecation — you strain, empty incompletely, and gas builds up proximally.
- Bowel endometriosis. Lesions on the rectum, sigmoid, or small intestine interfere with bowel function and create adhesions that kink loops of bowel.
- Dysbiosis. Endo patients show altered gut microbiota — less Lactobacillus and Bifidobacterium, more Proteobacteria.
- Migrating motor complex (MMC) dysfunction. Estrogen/progesterone fluctuations and endo inflammation weaken the bowel’s between-meals cleaning wave — the same failure that underlies SIBO.
Most episodes involve several of these at once, which is why a single intervention — cut dairy, take a probiotic — usually disappoints. The fix is layered.
Bowel Endometriosis
Between 5% and 12% of people with endometriosis have bowel or rectal involvement. The most common site is the rectosigmoid colon (about 70% of bowel lesions); others include the rectovaginal septum, terminal ileum, appendix, and cecum.
Red flags that point toward bowel endo rather than generic endo belly:
- Cyclic diarrhea or constipation that tracks your menstrual cycle rather than your diet.
- Painful defecation (dyschezia), especially during your period — one of the most specific symptoms.
- Rectal bleeding that appears only during menstruation — blood on the paper or streaking the stool, in sync with your period.
- Tenesmus — constant urge to defecate even when empty.
- Narrowed stool caliber — pencil-thin stools suggest stricturing.
Diagnosis is frustrating. Colonoscopy misses most bowel endo because lesions sit on the serosal (outer) surface and only reach the mucosa late. MRI of the pelvis with bowel prep is better but still imperfect; the practical gold standard is transvaginal ultrasound with bowel preparation performed at a specialist center. Treatment for deep infiltrating bowel endo is multidisciplinary surgery — a gynecologic surgeon and a colorectal surgeon together — ranging from shaving to discoid resection to segmental resection depending on lesion depth and circumference. See the excision vs ablation article.
SIBO — The Quiet Driver of Endo Belly
If you have endometriosis and dramatic evening bloating, small intestinal bacterial overgrowth is on the short list of likely co-drivers. Studies testing endo patients with breath tests have found SIBO prevalence rates ranging roughly from 40% to 80%, substantially higher than the general-population estimate of 6–15%.
The mechanism makes sense:
- Slow motility. Endo inflammation and autonomic dysfunction weaken the MMC — the wave that sweeps bacteria downstream between meals. When that fails, colonic bacteria migrate up into the small intestine.
- Pelvic adhesions. Surgery (laparoscopy, C-section, appendectomy) and scarring from endo itself kink the small bowel so contents pool and ferment.
- Opioid exposure. Chronic pelvic pain often leads to opioid use, which further slows motility.
- PPI use. Endo patients on PPIs for NSAID gastritis lose the stomach-acid barrier that normally kills ingested bacteria.
SIBO symptoms overlap almost perfectly with endo belly: bloating within 30–90 minutes of eating, excess gas, alternating diarrhea and constipation, brain fog, and food intolerances that keep multiplying. The test is a lactulose or glucose breath test. Treatment is typically antimicrobial (rifaximin for hydrogen-dominant, rifaximin plus neomycin or allicin for methane-dominant), followed by a prokinetic. See the SIBO page and the deep dives on root causes and prokinetics and relapse prevention. If you have endo plus chronic bloating, ask for a breath test before blaming yourself for reacting to everything.
The IBS Overlap
People with endometriosis are two to three times more likely to have irritable bowel syndrome than the general population. Several studies put the overlap above 50%. Part of this is real biological co-occurrence, and part is misdiagnosis running in the opposite direction: IBS is the single most common initial diagnosis given to people who actually have endometriosis. Primary care physicians and gastroenterologists see the bloating, cramping, and bowel changes, and label it IBS without ever asking about periods.
Shared mechanisms:
- Visceral hypersensitivity. Both conditions involve a nervous system that has learned to interpret normal gut signals as pain. Central sensitization (see the pelvic floor and central sensitization article) amplifies signals from uterus and bowel alike.
- Gut–brain axis dysregulation. Chronic pain alters vagal tone and the HPA axis, which in turn alters gut motility and secretion.
- Mast cell activation. Both endo lesions and IBS-affected bowel wall show increased mast cell density and degranulation, contributing to inflammation and hypersensitivity.
- Estrogen signaling. Both conditions flare with estrogen peaks — IBS symptoms often worsen around ovulation and menstruation, matching endo’s cyclical pattern.
Practical takeaway: if you were diagnosed with IBS years ago and never had a workup for endometriosis, and you have painful periods, pain with intercourse, or subfertility, revisit the endo question with a specialist. And if you have endometriosis, do not assume every GI symptom is endo — an IBS component may be treatable with interventions that do nothing for endo.
The Gut–Endo Axis
The gut and the endometrial lesions talk to each other through inflammation. The pathways most studied:
- Mast cell crosstalk. Mast cells cluster around endo lesions and in the intestinal wall. Their mediators (histamine, tryptase, prostaglandins) sensitize both compartments.
- Cytokine spillover. Peritoneal TNF-α, IL-6, and IL-8 drive intestinal inflammation; LPS leaking through a permeable gut barrier worsens pelvic inflammation.
- Microbiome differences. Endo patients show lower diversity, depleted Lactobacillus, enriched Enterobacteriaceae.
- Estrobolome. Gut bacteria producing β-glucuronidase deconjugate estrogen so it is reabsorbed rather than excreted — potentially raising circulating estrogen feeding lesions.
- Menstrual prostaglandins act on the bowel wall, not just the uterus — the reason many people get diarrhea at period onset even without endo.
When Gut Symptoms Are the Primary Problem
A useful clinical question: if we treated your gut aggressively, how much of your pain would go away? For some patients the answer is most of it. For others it is none of it. The only way to know is to try.
A reasonable sequence when endo belly dominates the clinical picture:
- Breath test for SIBO; treat if positive.
- Structured low-FODMAP trial (see below).
- Trial elimination of dairy and gluten, individually, with reintroduction.
- Add a prokinetic if motility is slow.
- Pelvic floor physical therapy if there are signs of puborectalis hypertonicity.
Reassess after 8–12 weeks. If pelvic pain, dyschezia, dyspareunia, and cyclic bleeding are still present, you still have an endo problem that needs surgical or hormonal treatment — but the gut noise is down and the signal is clearer.
The Low-FODMAP Trial
FODMAPs are fermentable oligosaccharides, disaccharides, monosaccharides, and polyols — short-chain carbohydrates that gut bacteria feast on, producing gas. For IBS, low-FODMAP has the strongest evidence of any dietary intervention (roughly 70% symptom improvement). Small studies in endo patients suggest similar benefit, particularly when SIBO or IBS coexists.
Three phases: Elimination (4–6 weeks) — remove all high-FODMAP foods (onion, garlic, wheat, most dairy, apples, pears, stone fruit, honey, HFCS, beans and lentils, cauliflower, mushrooms, artichoke, sugar alcohols). Reintroduction (6–8 weeks) — reintroduce one FODMAP subgroup at a time while keeping the rest low, identifying triggers. Personalization — long-term, avoid only your personal triggers.
Two resources worth the money: the Monash University FODMAP app (the diet was developed there; the app has food-specific portion cutoffs that generic lists miss) and Kate Scarlata’s books and blog. Do not stay in Phase 1 forever — chronic restriction starves the beneficial bacteria that ferment fiber into short-chain fatty acids. Work with a registered dietitian trained in FODMAP; the reintroduction phase is the part that matters. See also the low-FODMAP deep dive.
Anti-Inflammatory & Mediterranean Foundation
Underneath whatever elimination trial you run, a Mediterranean-style pattern is a reasonable default: fatty fish 2–3x weekly for omega-3, extra virgin olive oil as primary fat, dark leafy greens and berries and cruciferous vegetables (adjusted for FODMAP tolerance), nuts and seeds in small portions, minimal ultra-processed food and added sugar. See the diet and lifestyle article.
Dairy Elimination Trial
Dairy is worth a dedicated 4-week trial because there are three distinct reasons it might bother you:
- Lactose intolerance. About 65% of adults worldwide have reduced lactase. Hard aged cheeses and yogurt are usually tolerated when milk is not.
- A1 casein sensitivity. Most U.S. cow milk contains A1 β-casein, which digests into BCM-7, a peptide linked to low-grade gut inflammation. A2-only milk (or goat/sheep milk) may be tolerated when A1 is not.
- General inflammatory load. Dairy saturated fat can nudge prostaglandin balance pro-inflammatory in susceptible people.
Protocol: eliminate all dairy for four weeks, then reintroduce in order: butter → hard cheese → yogurt → A2 milk → A1 milk. Note where symptoms return.
Gluten Elimination Trial
A 2012 study of endo patients on a 12-month gluten-free diet reported symptom improvement in about 75%. Likely explanations include non-celiac gluten sensitivity, the FODMAP fructans in wheat, and withdrawal of the processed foods wheat rides along with. Trial: 4–6 weeks of complete elimination (including soy sauce, non-GF oats, hidden sources), then a clear reintroduction test — sourdough, pasta, or beer — tracking symptoms for 48–72 hours.
Before going gluten-free long-term, test for celiac while still eating gluten. Tissue transglutaminase IgA (with total IgA) is unreliable once you have quit; a biopsy-confirmed diagnosis has implications for family members, bone density screening, and nutrient monitoring that “I just feel better off wheat” does not.
Specific Foods Endo Patients Flag
Beyond the major elimination categories, endo patients repeatedly identify a handful of foods that worsen symptoms:
- Red meat. A 2018 Nurses’ Health Study II cohort found more than two daily servings carried a 56% higher endo risk. Mechanisms: iron-driven oxidative stress in lesions, arachidonic acid feeding prostaglandin E2.
- Processed and refined carbs. Spike insulin, which raises bioavailable estrogen.
- Alcohol. Raises circulating estrogens, impairs hepatic estrogen clearance, is pro-inflammatory. Many patients find one drink triggers a flare.
- Caffeine. Mixed disease-risk evidence but a significant subset of patients notice worse bloating above one cup. Worth a two-week trial.
Fiber — Type Matters
“Eat more fiber” is the standard gut advice, and for endo patients it is half right. Total fiber matters, but the type of fiber matters more.
- Soluble fiber (psyllium, oat beta-glucan, chia, flax, kiwifruit, partially ripe bananas) forms a gel, slows transit in diarrhea and speeds it in constipation, and ferments gently. It is the most tolerated fiber in endo belly.
- Insoluble fiber (wheat bran, raw vegetables, the skins of fruits) adds bulk and can worsen gas and mechanical distension in a sensitive bowel. Use in moderation.
- High-FODMAP fibers (inulin, chicory root, fructo-oligosaccharides added to yogurts and bars) are marketed as “prebiotic” but are the exact fibers SIBO patients ferment explosively. Read labels.
A reasonable default: 1 to 2 teaspoons of psyllium husk daily in water, built up gradually, with the rest of fiber coming from soft-cooked vegetables and ripe fruit.
Digestive Support Tools
- Digestive bitters before meals stimulate acid, bile, and pancreatic secretion — useful when protein meals feel heavy.
- Ginger tea or 1–2 g ginger capsules — mild prokinetic with decent dysmenorrhea evidence.
- Enteric-coated peppermint oil (IBgard, Pepogest), 0.2–0.4 mL three times daily before meals — one of the best-evidenced IBS treatments. The coating matters.
- Prokinetics — prescription (low-dose naltrexone, low-dose erythromycin, prucalopride) or OTC (ginger, artichoke). Essential post-SIBO to prevent relapse.
- Targeted probiotics. Strains with some evidence: Bifidobacterium infantis 35624 (Align), Lactobacillus plantarum 299v, VSL#3 / Visbiome. Skip products with inulin or FOS if SIBO-prone.
Managing an Acute Endo-Belly Episode
When you are already distended at 7 PM and facing four hours until bed, a few things help:
- Heating pad on the abdomen — relaxes bowel smooth muscle.
- Gentle walking 10–20 minutes stimulates motility; avoid high-intensity exercise during a flare.
- Diaphragmatic breathing for 5 minutes lowers sympathetic tone and massages the bowel — the most under-used tool for acute bloat.
- Enteric-coated peppermint oil capsule.
- Loose clothing — bloated bowel plus constriction equals more pain.
- Legs-up-the-wall pose for ten minutes redistributes gas.
- Simethicone OTC, modest but real.
- Magnesium citrate 200–400 mg at bedtime if constipation is driving it.
When to Investigate Gut Symptoms Separately
Not every GI symptom in an endo patient is endo. A gastroenterology referral — not another gynecology appointment — is warranted when any of the following appear:
- Unintentional weight loss.
- Rectal bleeding beyond the cyclic pattern (bleeding that does not track periods, or dark/black stool).
- Severe constipation resistant to basic measures, especially with progressive stool narrowing.
- Iron deficiency anemia not fully explained by menstrual loss.
- Nocturnal symptoms — diarrhea, pain, or bleeding that wake you from sleep. Endo symptoms generally do not wake you; IBD symptoms do.
- Family history of inflammatory bowel disease, celiac disease, or colon cancer.
These are signals for a workup that might include colonoscopy, fecal calprotectin, celiac serologies, and cross-sectional imaging. You can have endo and Crohn’s disease, endo and celiac, endo and colorectal disease. One diagnosis does not protect you from another.
The Pelvic Floor Contribution
A tight pelvic floor is probably the single most under-recognized driver of endo belly. When the puborectalis (the muscle sling that wraps behind the rectum) stays chronically contracted, the rectum cannot straighten during defecation. You strain, empty incompletely, and gas builds up proximally — the belly distends from below.
Signs it is part of your picture: sensation of incomplete evacuation; needing to splint (press on the perineum or vaginal wall) to finish; straining even when stool is soft; pain with intercourse or tampon insertion; urinary urgency or hesitancy.
Pelvic floor physical therapy with a therapist trained in internal work is the treatment — down-training (learning to release, not strengthen), manual myofascial release, biofeedback, home programs with wands and dilators. Expect 8–16 sessions over 3–6 months. See the pelvic floor therapy article.
Key Research Papers
- Becker CM, et al. ESHRE guideline: endometriosis. Hum Reprod Open. 2022;2022(2):hoac009.
- Moore JS, et al. Endometriosis in patients with irritable bowel syndrome: specific symptomatic and demographic profile, and response to the low FODMAP diet. Aust N Z J Obstet Gynaecol. 2017;57(2):201–205.
- Maroun P, Cooper MJW, Reid GD, Keirse MJNC. Relevance of gastrointestinal symptoms in endometriosis. Aust N Z J Obstet Gynaecol. 2009;49(4):411–414.
- Mathias JR, et al. Relation of endometriosis and neuromuscular disease of the gastrointestinal tract: new insights. Fertil Steril. 1998;70(1):81–88. (Foundational SIBO/motility–endo link.)
Live PubMed Searches
For further reading, the following PubMed topic searches return current peer-reviewed work on the gut–endometriosis connection:
- Endometriosis and small intestinal bacterial overgrowth
- Bowel endometriosis diagnosis and imaging
- Low-FODMAP diet in endometriosis
- Irritable bowel syndrome and endometriosis overlap
- Endometriosis and the gut microbiome
- Deep infiltrating endometriosis of the rectosigmoid
- Endometriosis and the gluten-free diet
- Endometriosis, visceral hypersensitivity, and central sensitization
Connections
- Laparoscopy: Excision vs Ablation
- Diet and Lifestyle
- SIBO
- Celiac Disease
- SIBO: Prokinetics and Relapse Prevention
- Low-FODMAP Diet
- Pelvic Floor Therapy and Central Sensitization
- Crohn's Disease
- Endometriosis
- Irritable Bowel Syndrome
- Inflammatory Bowel Disease
- Diagnosis Delay and Imaging
- Hormonal Therapy Options
- Fertility and Endometriosis
- Adenomyosis Overlap
- Gut-Brain Axis
- Bloating
- Probiotics