Constipation
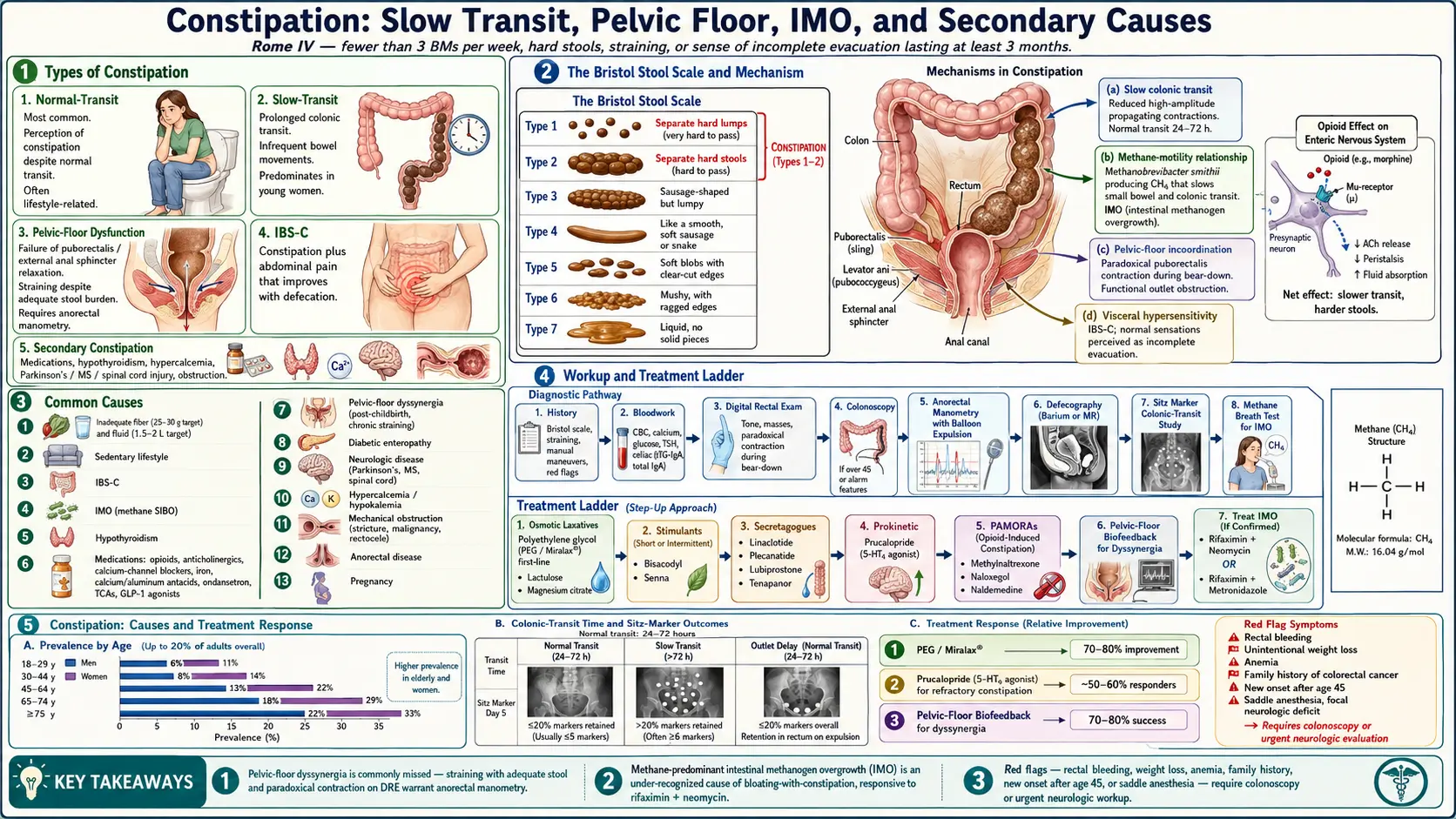

Table of Contents
- Overview
- Types of Constipation
- Common Causes
- Mechanisms
- Evaluation
- Management
- When to Seek Medical Care
- Connections
- References & Research
- Featured Videos
Overview
Constipation is one of the most common GI complaints, affecting up to 20 percent of adults at any given time. The Rome IV definition is fewer than three bowel movements per week, hard or lumpy stools, sense of incomplete evacuation, straining, or need for manual maneuvers, persisting at least three months. Constipation is rarely a single disease and often involves several contributors at once: slow colonic transit, pelvic-floor dysfunction, dietary factors, medications, and metabolic conditions like hypothyroidism. The most under-recognized cause in adults with bloating-prevalent constipation is methane-predominant intestinal methanogen overgrowth (IMO), the methane-driven cousin of SIBO.
Types of Constipation
- Normal-transit constipation — the most common type; transit time is normal but the patient perceives constipation. Often functional, related to lifestyle.
- Slow-transit constipation — prolonged colonic transit, infrequent bowel movements, often resistant to fiber and laxatives. Predominates in young women.
- Pelvic-floor dysfunction (defecatory disorders) — failure of the pelvic-floor muscles to relax during defecation; presents with straining and incomplete evacuation despite adequate stool. Often missed without anorectal manometry.
- IBS with constipation (IBS-C) — constipation plus abdominal pain that improves with defecation.
- Secondary constipation — from medications, hypothyroidism, hypercalcemia, neurologic disease (Parkinson's, MS, spinal cord injury), bowel obstruction, anorectal disease.
Common Causes
- Inadequate fiber and fluid intake — the most common modifiable cause.
- Sedentary lifestyle — movement promotes colonic motility.
- IBS-C — functional disorder with constipation and abdominal pain.
- Intestinal methanogen overgrowth (IMO / methane SIBO) — methane production from Methanobrevibacter smithii slows colonic transit and produces constipation, often with bloating.
- Hypothyroidism — classic cause of constipation along with fatigue and cold intolerance.
- Medications — opioids (universal), anticholinergics, calcium-channel blockers, iron, calcium and aluminum antacids, ondansetron, tricyclics, GLP-1 agonists.
- Pelvic-floor dyssynergia — abnormal coordination of the pelvic-floor muscles; common after childbirth and in chronic straining.
- Diabetic enteropathy — autonomic neuropathy slows colonic motility.
- Neurologic disease — Parkinson's, MS, spinal cord injury, autonomic dysfunction.
- Hypercalcemia and hypokalemia — both impair smooth-muscle function.
- Mechanical obstruction — colonic stricture, malignancy, hernia, rectocele.
- Anorectal disease — fissure, hemorrhoid pain causing voluntary withholding.
- Pregnancy — progesterone slows GI motility; iron supplementation aggravates.
Mechanisms
- Slow colonic transit — reduced high-amplitude propagating contractions; normal transit is roughly 24–72 hours from mouth to anus.
- Methane and the methane-motility relationship — methane gas produced by archaea slows small-bowel and colonic transit; explains the bloating-with-constipation pattern.
- Pelvic-floor incoordination — failure to relax the puborectalis or external anal sphincter during defecation; produces functional outlet obstruction.
- Visceral hypersensitivity — in IBS-C; normal sensations are perceived as constipation or incomplete evacuation.
- Reduced colonic water absorption — the chloride-channel activators (linaclotide, plecanatide) and prostaglandin agonists (lubiprostone) all work by increasing intestinal fluid secretion to soften stool.
- Opioid receptor activation in the gut — opioid receptors in the enteric nervous system slow motility independently of central effects; treated with peripherally acting mu-opioid receptor antagonists (PAMORAs).
Evaluation
- History — stool frequency and form (Bristol scale), straining, incomplete evacuation, manual maneuvers, blood in stool, weight loss, medications, family history.
- Bloodwork — CBC, calcium, glucose, TSH; consider celiac serology if other GI symptoms.
- Digital rectal exam — checks tone, masses, presence of stool; helps screen for pelvic-floor dyssynergia (paradoxical contraction with bear-down).
- Colonoscopy — recommended at age 45 and earlier with alarm features (rectal bleeding, weight loss, anemia, family history).
- Anorectal manometry with balloon expulsion — for refractory constipation; identifies dyssynergia.
- Defecography (barium or MR) — for suspected rectocele, intussusception, dyssynergia.
- Sitz markers (radiopaque markers) study — measures colonic transit time.
- Hydrogen / methane breath test — for IMO when bloating is prominent. See the Breath Test Guide.
Management
- Diet and lifestyle — 25–30 g of fiber daily, 1.5–2 L of fluid, regular physical activity, scheduled bowel routine after meals (gastrocolic reflex).
- Osmotic laxatives — polyethylene glycol (Miralax) is first-line; lactulose, magnesium citrate.
- Stimulant laxatives — bisacodyl, senna; safe for short- to medium-term use despite older concerns.
- Secretagogues — linaclotide, plecanatide, lubiprostone, tenapanor for chronic idiopathic constipation and IBS-C.
- Prokinetic — prucalopride (5-HT4 agonist) for slow-transit constipation refractory to laxatives.
- PAMORAs — methylnaltrexone, naloxegol, naldemedine for opioid-induced constipation.
- Pelvic-floor biofeedback — the treatment of choice for pelvic-floor dyssynergia.
- Methane-targeted therapy — combination rifaximin + neomycin (or rifaximin + metronidazole) for confirmed IMO; herbal antimicrobials as an alternative; see Rifaximin Protocols and Herbal Antimicrobials.
- Treat the underlying cause — levothyroxine for hypothyroidism, magnesium correction, medication review.
- Surgery — subtotal colectomy is a last resort for severe slow-transit constipation refractory to all medical therapy.
When to Seek Medical Care
- Rectal bleeding, melena, or persistent change in bowel habits in someone over 45.
- Unintentional weight loss greater than 5 percent of body weight.
- Anemia or iron deficiency without obvious source.
- Family history of colon cancer or IBD.
- Severe abdominal pain, distension, or vomiting (rule out obstruction).
- New constipation in an older adult that does not respond to standard measures.
- Constipation with neurologic symptoms (saddle anesthesia, leg weakness) — rule out cauda equina.
Connections
- Lactulose — How the Laxative Actually Works (In-Depth)
- IMO & Methane Constipation
- Irritable Bowel Syndrome
- Thyroid Disorders
- SIBO
- Bloating
- Herbal Antimicrobials
- Abdominal Pain
- SIBO Breath Test Guide
- Rifaximin Protocols
- Magnesium
- Prunes (Natural Laxative)
- Prunes for Constipation Relief
- Pears (Natural Laxative)
- Pears for Constipation Relief
- Hashimoto's Thyroiditis
- Chronic Diarrhea
- Diabetes
- Parkinson's Disease
- IBS Subtypes (Rome IV)
- SIBO Root Causes
- Prokinetics and Relapse Prevention
- IBS Medications Guide
- Hemorrhoids
References & Research
Historical Background
Constipation has been described in medical literature for millennia, but the modern era of evidence-based therapy began with the 1960s development of polyethylene glycol, the 2008 approval of lubiprostone, and the 2012 approval of linaclotide. Pelvic-floor biofeedback emerged from anorectal manometry research in the 1980s. The 2020 ACG guideline on SIBO recognized methane-predominant overgrowth (IMO) as a discrete entity contributing to constipation.
Key Research Papers
- Pimentel M, Saad RJ, Long MD, Rao SSC. ACG clinical guideline: small intestinal bacterial overgrowth. American Journal of Gastroenterology. 2020;115(2):165-178.
- Bharucha AE, Lacy BE. Mechanisms, evaluation, and management of chronic constipation. Gastroenterology. 2020;158(5):1232-1249.
- Lembo AJ, Schneier HA, Shiff SJ, et al. Two randomized trials of linaclotide for chronic constipation. New England Journal of Medicine. 2011;365(6):527-536.
- Camilleri M, Kerstens R, Rykx A, Vandeplassche L. A placebo-controlled trial of prucalopride for severe chronic constipation. New England Journal of Medicine. 2008;358(22):2344-2354.
- Rao SSC, Welcher KD, Leistikow JS. Obstructive defecation: a failure of rectoanal coordination. American Journal of Gastroenterology. 1998;93(7):1042-1050.
- Chassany O, Bonaz B, Bruley DesVarannes S, et al. Acute exacerbation of pain in irritable bowel syndrome: efficacy of phloroglucinol/trimethylphloroglucinol. Alimentary Pharmacology & Therapeutics. 2007;25(9):1115-1123.
- Mearin F, Lacy BE, Chang L, et al. Bowel disorders. Gastroenterology. 2016;150(6):1393-1407.
- Locke GR, Pemberton JH, Phillips SF. American Gastroenterological Association medical position statement: guidelines on constipation. Gastroenterology. 2000;119(6):1761-1766.
- Sharma A, Rao SSC. Constipation: pathophysiology and current therapeutic approaches. Handbook of Experimental Pharmacology. 2017;239:59-74.
- Pimentel M, Lin HC, Enayati P, et al. Methane, a gas produced by enteric bacteria, slows intestinal transit and augments small intestinal contractile activity. American Journal of Physiology-Gastrointestinal and Liver Physiology. 2006;290(6):G1089-G1095.
PubMed Topic Searches
- Chronic constipation management
- Pelvic-floor dyssynergia biofeedback
- Methane (IMO) and constipation
- Linaclotide for IBS-C / chronic constipation
- Opioid-induced constipation
- Slow-transit constipation