Hydrogen vs. Methane vs. Hydrogen Sulfide SIBO
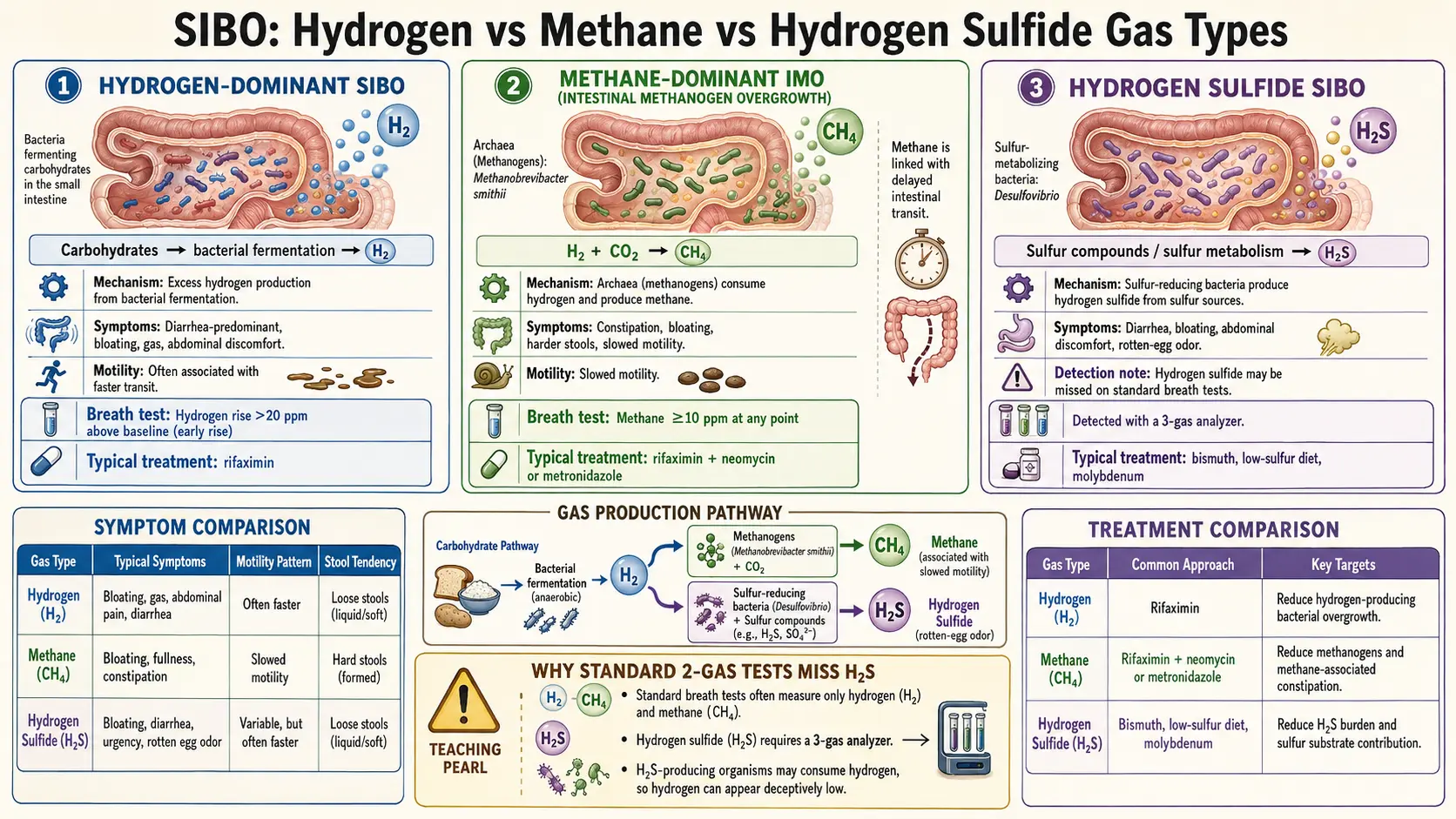
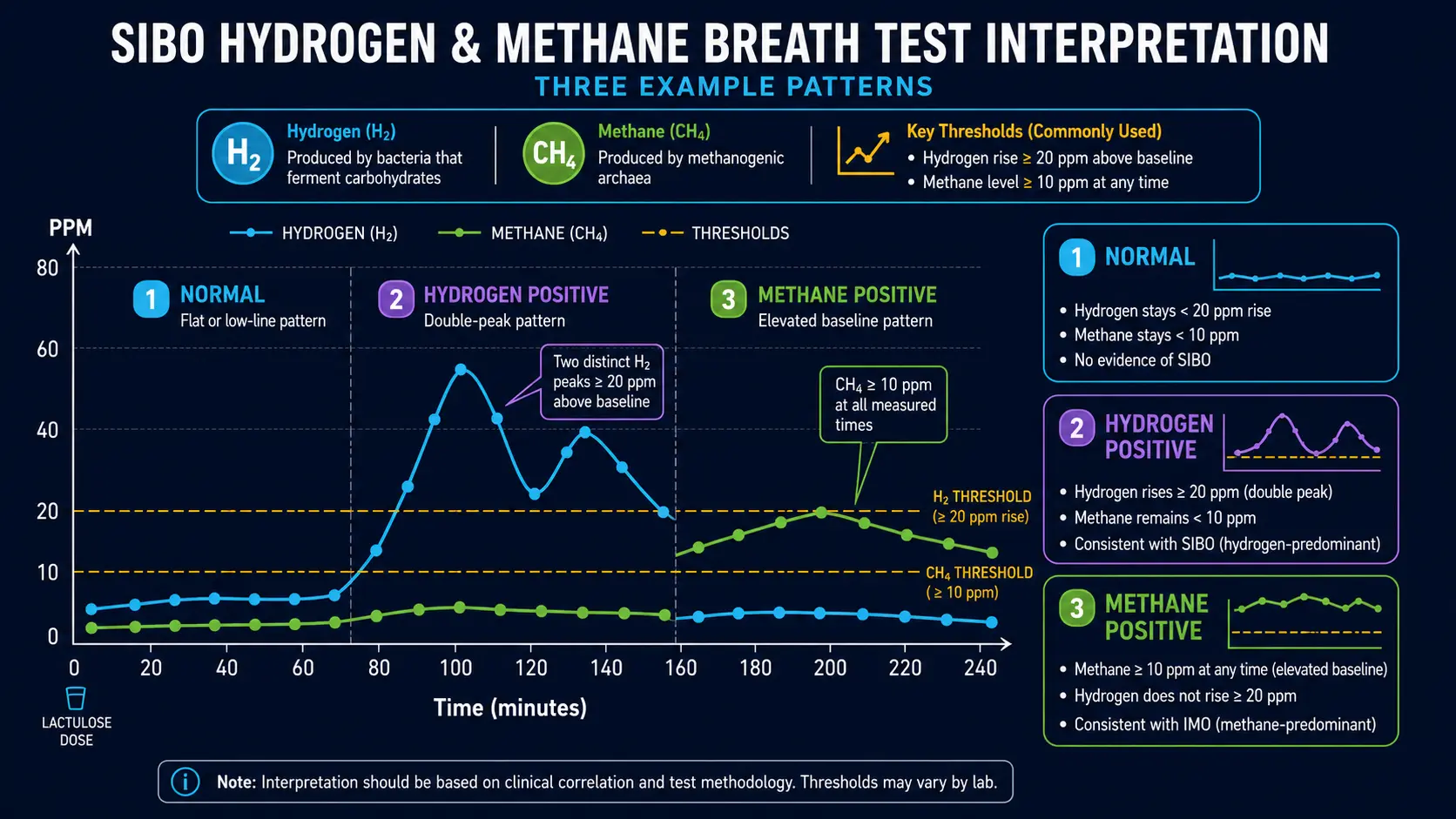
Table of Contents
- What the Three Gas Subtypes Mean for You
- Hydrogen-Dominant SIBO (the diarrhea one)
- Methane-Dominant SIBO / IMO (the constipation one)
- Hydrogen Sulfide SIBO (the rotten-egg one)
- How to Tell Which One You Have
- Why Treatment Differs Dramatically
- Can You Have More Than One Subtype?
- Key Research Papers
- Research Papers
- Connections
- Featured Videos
1. What the Three Gas Subtypes Mean for You
If you have been diagnosed with SIBO and nothing seems to be working, there is a good chance that nobody has told you which kind of SIBO you actually have. That one detail changes almost everything about treatment — which antibiotic works, which diet helps, and whether constipation or diarrhea will be your dominant symptom.
SIBO is not a single disease. It is a description of a pattern: too many microbes in the wrong part of your gut. Those microbes ferment food you eat and release gases. The particular gas they release depends on which microbes have moved in. There are three:
- Hydrogen — made by ordinary gut bacteria fermenting carbohydrates. Tends to drive diarrhea, urgency, and classic IBS-D symptoms.
- Methane — made by an archaeon (a non-bacterial microbe) called Methanobrevibacter smithii. Tends to drive stubborn constipation and hard, pellet-like stools. This subtype is now officially renamed IMO (intestinal methanogen overgrowth).
- Hydrogen sulfide — made by sulfate-reducing bacteria such as Desulfovibrio. Produces sulfurous, rotten-egg belches and diarrhea, sometimes with bladder or skin symptoms.
Almost every patient we hear from has tried one round of antibiotics, felt briefly better, and then relapsed. Usually this is because the wrong gas was targeted, or no one ever checked for methane and hydrogen sulfide in the first place. The rest of this article walks through each subtype and why the distinction matters.
2. Hydrogen-Dominant SIBO (the diarrhea one)
Hydrogen-dominant SIBO is the "classic" picture and the one most doctors know about. Ordinary gut bacteria — E. coli, Klebsiella, Enterococcus, Bacteroides, Proteus — migrate into the small intestine, where they should not be in large numbers. When they reach carbohydrates before you do, they ferment them and release hydrogen gas.
What it feels like
- Bloating that worsens through the day, especially after bread, onions, garlic, apples, dairy, or beans.
- Loose, urgent stools — often within an hour of eating.
- Abdominal cramping and gurgling (borborygmi).
- Foul-smelling gas, though not sulfurous.
- Sometimes fat in the stool (steatorrhea) because the bacteria deconjugate your bile acids before they can do their job.
The IBS-D overlap
If you have been told you have IBS-D (diarrhea-predominant irritable bowel syndrome), there is roughly a 50–60% chance you actually have hydrogen-dominant SIBO underneath. The two diagnoses are so intertwined that the FDA approved rifaximin specifically for IBS-D based on the TARGET trials — essentially acknowledging that a large share of "IBS" is really bacterial overgrowth in disguise.
What the breath test looks like
On a lactulose breath test, hydrogen-dominant SIBO shows a rise of at least 20 ppm above baseline within the first 90 minutes. Often you will see a sharp early peak while methane stays flat near zero. That early rise means bacteria are fermenting the test sugar up in your small intestine, long before it should have reached the colon.
3. Methane-Dominant SIBO / IMO (the constipation one)
Here is the twist most patients are never told: the microbe that causes methane-dominant SIBO is not a bacterium at all. It is Methanobrevibacter smithii, a member of a completely separate domain of life called archaea. Archaea look a bit like bacteria under a microscope, but biochemically they are as different from bacteria as you are from a mushroom.
This matters because most antibiotics are designed to kill bacteria. Archaea shrug them off. That is why so many people with methane SIBO take a course of rifaximin, feel nothing, and assume the diagnosis was wrong.
Because the problem organism is an archaeon and can colonize the colon as well as the small intestine, the condition was officially renamed in 2020. You will now see it called IMO (intestinal methanogen overgrowth) on newer lab reports.
Methane is a brake pedal
In a landmark 2006 study, Pimentel and colleagues showed that methane gas slows intestinal transit by roughly 59% in animal models. Methane does not just sit there. It directly tells the smooth muscle of your intestines to stop contracting forward and instead make useless non-propagating squeezes.
Think of methane as a brake pedal pressed against the floor of your small intestine. The harder the archaea work, the slower everything moves. The slower things move, the more time M. smithii has to grow. It is a self-reinforcing loop, which is exactly why methane SIBO is so hard to shake.
What it feels like
- Constipation that laxatives barely touch. You can swallow a glass of Miralax and still not go for three days — because the problem is not dehydrated stool, it is a paralyzed bowel.
- Hard, dry, pellet-like stools (Bristol type 1 or 2).
- Incomplete evacuation — the feeling that something is still up there.
- Rock-hard bloating, often visibly distended by evening.
- Weight gain or difficulty losing weight, because methanogens also help humans extract extra calories from food (this has been studied in obesity research).
The IBS-C link
If you have been diagnosed with IBS-C, there is a very high chance methane is involved. Studies consistently find that 75–85% of methane-positive patients have the constipation phenotype. Why Miralax does not fix it: osmotic laxatives pull water into the bowel, but they cannot force peristalsis to happen. If methane has jammed the motor, more water just sits there.
4. Hydrogen Sulfide SIBO (the rotten-egg one)
For years, clinicians saw a frustrating subset of SIBO patients whose breath tests came back with flat lines on both hydrogen and methane — but whose symptoms were unmistakably SIBO. These cases were written off as false negatives or as "non-responders." They were neither. They had hydrogen sulfide SIBO, and there was simply no test for it.
The organisms involved are sulfate-reducing bacteria, primarily Desulfovibrio and some Fusobacterium species. These microbes eat hydrogen produced by other bacteria and convert it into hydrogen sulfide (H2S) — the same gas that gives rotten eggs and warm swamps their smell.
What it feels like
- Sulfurous, rotten-egg belches — a symptom patients almost always remember clearly, because it is embarrassing.
- Gas and stool with a distinct sulfur smell.
- Diarrhea, often explosive.
- Visceral hypersensitivity — everything hurts more than it should.
- A harder-to-explain cluster: bladder urgency, skin flushing, brain fog, sulfur-food intolerance (eggs, garlic, cruciferous vegetables, red wine).
Why it was missed for so long
On an old-style two-gas breath test, hydrogen sulfide SIBO looks like nothing. The hydrogen curve is flat because sulfate-reducing bacteria consume hydrogen as fast as it is produced. Methane is flat because there are no methanogens. A "flat-line" breath test was historically reported as negative — which is how thousands of symptomatic patients got sent home without a diagnosis.
The modern trio-smart breath test (Gemelli Biotech) measures all three gases and flags H2S at levels ≥3 ppm. If your two-gas test was negative but you know something is wrong, this is the test to ask for.
The bismuth angle
One of the more interesting emerging therapies is plain old bismuth subsalicylate (Pepto-Bismol). Bismuth binds hydrogen sulfide directly in the gut lumen, neutralizing it. Research protocols are still being worked out, but many practitioners now add bismuth alongside standard antimicrobials when H2S is the dominant gas.
5. How to Tell Which One You Have
Before you can pick a treatment, you need a breath test — ideally one that measures all three gases. Very quickly, here is how each pattern looks:
- Hydrogen-dominant: H2 rises at least 20 ppm in the first 90 minutes. Methane stays low. H2S low or absent.
- Methane-dominant (IMO): Methane reaches ≥10 ppm at any point during the test, often as a flat, persistent elevation from baseline onward.
- Hydrogen sulfide: H2S ≥3 ppm at any point. Hydrogen may be flat or suppressed (because H2S producers eat the hydrogen).
- Mixed: Two or three gases elevated together. Much more common than people realize.
For a deeper dive on how to prepare for the test, how to read the curves, and why false negatives happen, see our full Breath Test Guide.
6. Why Treatment Differs Dramatically
This is the part that really matters. The same drug that cures one subtype can be completely useless for another.
Hydrogen-dominant: rifaximin alone
Rifaximin (Xifaxan) 550 mg three times daily for 14 days is the standard. The TARGET trials reported an eradication rate of around 64–74% in hydrogen-predominant disease. Because rifaximin is barely absorbed from the gut (<0.4%), it acts almost entirely where you want it and has a very clean side-effect profile.
Methane-dominant (IMO): rifaximin PLUS neomycin
Rifaximin by itself normalizes methane in only about 28% of cases — because, again, archaea are not bacteria and rifaximin is a bacterial drug. The combination of rifaximin 550 mg TID plus neomycin 500 mg BID for 14 days pushes that number to roughly 85%. Alternative or additive approaches:
- Allicin (stabilized garlic extract) is one of the very few natural compounds with documented activity against Methanobrevibacter smithii. Typical dose: 450 mg two to three times daily.
- Metronidazole can substitute for neomycin if neomycin is not tolerated.
- Lovastatin lactone (SYN-010) is in trials as a methane-specific therapy.
For the full protocol including dosing details, see Rifaximin Protocols.
Hydrogen sulfide: a different playbook
There is no approved first-line regimen for H2S SIBO yet, but practitioner consensus is converging on:
- Rifaximin 550 mg TID for 14 days, often combined with bismuth subsalicylate.
- A low-sulfur diet during treatment — reducing eggs, garlic, onions, cruciferous vegetables, red meat, and high-sulfite wines for a short window.
- Molybdenum as a cofactor to help the body clear residual sulfide.
Herbal options cross all three subtypes
The Chedid 2014 Johns Hopkins study showed herbal antimicrobial protocols matched rifaximin head-to-head. Berberine, oregano oil, and neem hit a broad range of organisms, and allicin adds methane coverage. See Herbal Antimicrobials for the full comparison.
7. Can You Have More Than One Subtype?
Yes — in fact, it is the rule rather than the exception. The trio-smart validation data suggests that somewhere between a third and a half of SIBO patients have two or more gases elevated at the same time. Common combinations:
- Hydrogen + methane: alternating diarrhea and constipation, often matching an IBS-M label.
- Hydrogen + hydrogen sulfide: diarrhea-predominant with the characteristic sulfur belches.
- All three elevated: the most severe phenotype, usually after multiple failed treatment rounds.
How treatment is sequenced
When more than one gas is driving symptoms, the usual strategy is to treat methane first (because it will paralyze motility and sabotage everything else if you ignore it), then hit hydrogen and hydrogen sulfide in a second round. Some clinicians do it all at once with rifaximin + neomycin + bismuth for two weeks; others sequence two courses a month apart.
Whatever the order, prokinetic therapy after eradication is non-negotiable if you want to stop the relapses. Without restoring the migrating motor complex, SIBO comes back within a year in roughly half of patients. See Prokinetics & Relapse Prevention and Root Causes for the rest of the puzzle.
8. Key Research Papers
- Pimentel M, et al. Methane, a gas produced by enteric bacteria, slows intestinal transit and augments small intestinal contractile activity. Am J Physiol. 2006;290(6):G1089-G1095.
- Singer-Englar T, et al. Validation of a hydrogen and methane and hydrogen sulfide breath test device. Clin Gastroenterol Hepatol. 2022;20(7):e1488-e1497.
- Takakura W, Pimentel M. Small intestinal bacterial overgrowth and irritable bowel syndrome: an update. Frontiers in Psychiatry. 2020;11:664.
- Pimentel M, Saad RJ, Long MD, Rao SSC. ACG Clinical Guideline: Small Intestinal Bacterial Overgrowth. Am J Gastroenterol. 2020;115(2):165-178.
9. Research Papers
Live PubMed searches on the specific microbes and mechanisms discussed in this article. Each link opens a fresh query, so the results stay current.
- PubMed: Intestinal methanogen overgrowth (IMO)
- PubMed: Hydrogen sulfide SIBO
- PubMed: Methanobrevibacter smithii and constipation
- PubMed: Desulfovibrio and IBS
- PubMed: Rifaximin + neomycin for methane
- PubMed: Allicin and methanogens
- PubMed: Bismuth subsalicylate and hydrogen sulfide
- PubMed: Trio-smart breath test
Connections
- The Gut Barrier & Your Microbiome — interactive animation
- SIBO Overview
- Rifaximin Protocols
- Root Causes
- Herbal Antimicrobials
- Breath Test Guide
- Prokinetics and Relapse Prevention
- Elemental Diet
- Low-FODMAP Diet
- IMO and Constipation
- Irritable Bowel Syndrome
- Oregano
- Berberine
- Probiotics
- POTS
- Constipation
- Sulfur
- Bloating
- Gut Microbiome