Rifaximin (Xifaxan) Protocols for SIBO
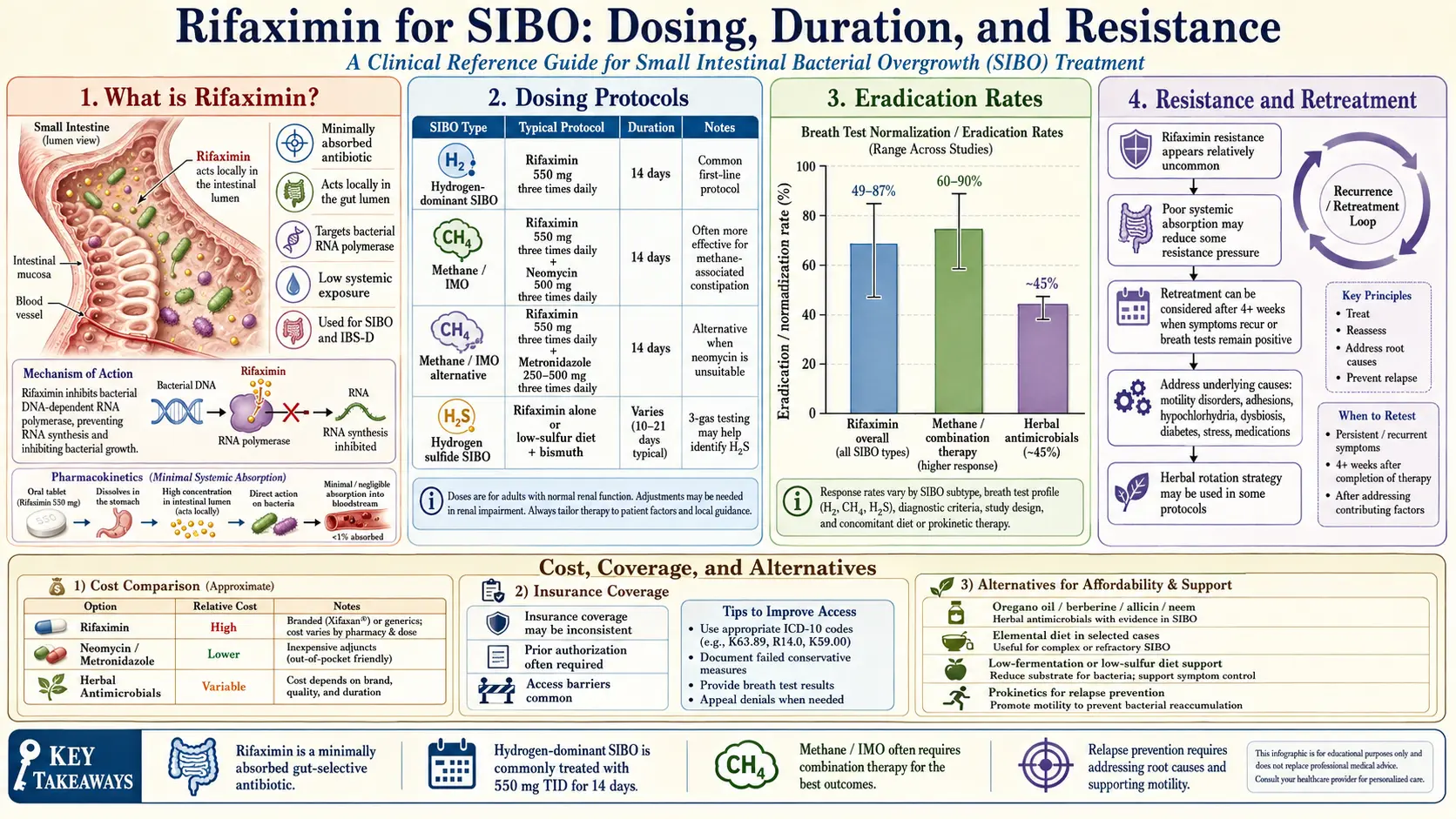
Table of Contents
- What Rifaximin Is (And Why It’s Different)
- The Standard Protocol
- How Effective Is It, Really?
- Methane-Dominant SIBO Needs a Combo
- Hydrogen Sulfide SIBO Is Different Again
- The Insurance Battle (Expect It)
- Retreatment Protocols
- Side Effects and Safety
- When Rifaximin Fails — What Next
- When You Can’t Get Rifaximin (Alternatives)
- Critical: Pair with a Prokinetic
- Key Research Papers
- Connections
- Featured Videos
1. What Rifaximin Is (And Why It’s Different)
Rifaximin is a semi-synthetic derivative of rifamycin, the same antibiotic family used against tuberculosis. In the US it’s sold as Xifaxan (made by Salix). In the EU it’s Normix. In the UK it’s Targaxan or Xifaxanta. Same drug, different label.
The reason rifaximin stands apart from every other antibiotic your gastroenterologist could write for is a single pharmacokinetic fact: less than 0.4% of the dose is systemically absorbed. More than 99% of what you swallow stays in the gut lumen, does its work locally, and is excreted essentially unchanged in the stool. It never really enters your bloodstream in meaningful concentrations.
That’s why rifaximin’s side-effect profile looks nothing like ciprofloxacin, metronidazole, or amoxicillin. You don’t get the tendon warnings, the alcohol interaction, the pervasive yeast overgrowth, or the whole-body microbiome devastation you expect from a 14-day course of a systemic antibiotic. It targets the small bowel lumen almost exclusively — which is exactly where SIBO lives.
2. The Standard Protocol
For hydrogen-dominant SIBO, the evidence-based dose is:
- 550 mg three times daily (TID) for 14 days
- Take with or without food — absorption is already negligible, so food doesn’t matter
- No special spacing required between doses and other medications
- No alcohol restriction (unlike metronidazole)
Most patients who are going to respond notice reduced bloating and diarrhea somewhere between day 4 and day 7. If you’re on day 10 and feel exactly the same, the drug probably isn’t working for your case — more on that below.
The total course is 42 tablets of the 550 mg strength. Fill the whole thing at once if you can; pharmacies sometimes only partial-fill, and discovering on day 7 that you can’t get the second half is the last thing you want.
3. How Effective Is It, Really?
The honest answer requires looking at the registration trials. Pimentel et al. ran the TARGET 1 and TARGET 2 trials (NEJM 2011) and later the TARGET 3 retreatment trial, which together became the FDA-approval dossier for IBS-D.
- SIBO eradication rate by breath test at 2 weeks post-treatment: roughly 64–74% in hydrogen-dominant cases.
- Adequate symptom relief in IBS-D: around 44% (this was the FDA primary endpoint — not eradication, but patient-reported relief).
- Median duration of response: about 10–12 weeks before symptoms start creeping back in responders who never address the underlying motility issue.
Read those numbers carefully. A 44% response in the IBS-D trial sounds modest until you remember the placebo arm got about 32% — the treatment effect is real, but it’s not a miracle cure. And the 10–12 week window matters: if you don’t have a relapse-prevention plan in place, you’ll be back in the gastroenterologist’s office by month four.
4. Methane-Dominant SIBO Needs a Combo
This is the single most important thing to understand if your breath test showed methane — now formally called intestinal methanogen overgrowth (IMO).
Rifaximin alone clears methane in only about 28% of IMO patients. That is a bad number. If your provider hands you a monotherapy rifaximin script for a methane-positive test, you are being undertreated.
The evidence-based combination is:
- Rifaximin 550 mg TID × 14 days, PLUS
- Neomycin 500 mg BID × 14 days
Methane normalization jumps to approximately 85% with the combination. The reason is mechanistic: methane is produced by Methanobrevibacter smithii, which is an archaeon, not a bacterium. Rifaximin’s spectrum of action on archaea is weak. Neomycin — an aminoglycoside with poor oral absorption, so it also stays in the gut lumen — picks up the slack.
If neomycin is refused or unavailable (some prescribers worry about ototoxicity even though oral doses make systemic levels vanishingly low), the evidence-supported alternative is rifaximin + metronidazole 250 mg TID × 14 days. It’s a harsher regimen on the gut and alcohol is absolutely contraindicated, but it works.
For more on why the gas subtype fundamentally changes the treatment choice, see Hydrogen vs. Methane vs. Hydrogen Sulfide.
5. Hydrogen Sulfide SIBO Is Different Again
The third subtype — hydrogen sulfide-dominant SIBO, driven primarily by Desulfovibrio and Fusobacterium species — has no established, trial-validated rifaximin protocol. This is recent territory. The trio-smart breath test only became commercially available in 2021.
What SIBO-focused practitioners are doing in practice: rifaximin 550 mg TID × 14 days plus bismuth subsalicylate (Pepto-Bismol, 2 caplets four times daily). The bismuth binds hydrogen sulfide in the gut lumen, converting it to relatively inert bismuth sulfide and physically removing the toxic gas. Evidence is still emerging, case-series quality, not randomized trials. It’s a reasonable empirical approach but ask your provider for informed expectations.
6. The Insurance Battle (Expect It)
Brace yourself. Xifaxan retail is roughly $2000–2500 for a single 14-day course. Salix’s patent protections and lack of a US generic have kept prices extraordinary. Insurance coverage is hit-or-miss because the FDA approval is for IBS-D and hepatic encephalopathy — not SIBO. Many plans will reject an Rx written with “SIBO” as the indication because it’s technically off-label.
Tactics that actually work:
- Have the Rx written with IBS-D as the indication. Most SIBO patients easily meet Rome IV criteria for IBS-D, which means this isn’t fraudulent — it’s accurate coding that matches what insurers will cover.
- Salix manufacturer copay assistance. Sign up at xifaxan.com. Eligible insured patients can drop their copay to roughly $5–$15 per month. Uninsured patients are usually ineligible (this is how most pharma copay cards are structured).
- Prior authorization with breath test results attached. A positive lactulose or trio-smart test is powerful documentation. Many denials are overturned on the first PA if the paper trail is strong.
- Appeal letters citing the ACG Clinical Guideline (2020), which explicitly recommends rifaximin for SIBO. This is peer-reviewed, society-endorsed guidance that insurers have a hard time ignoring on second appeal.
- Cash-pay options. GoodRx and Mark Cuban’s Cost Plus Drugs periodically bring the price down to roughly $1600–1800. Still brutal, but a thousand dollars less.
- International pharmacies. Canadian, UK, and Turkish pharmacies legally dispense generic rifaximin (Normix, Xifaxanta, or simple INN-labeled rifaximin) for $200–500 per course. US Customs generally tolerates personal-use importation of <90-day supplies of non-controlled prescription medications, but this is a legal gray area — understand you’re making an informed risk calculation.
None of this should be your job. But it is your job, so go in with the playbook.
7. Retreatment Protocols
Based on the TARGET 3 trial, the FDA approved up to 2 retreatments of rifaximin for patients who respond initially and then relapse. The typical real-world schedule is straightforward: retreat when symptoms return, usually 10–16 weeks after the initial course ends.
Each retreatment typically matches the first course in efficacy — there is no clear evidence of rapid resistance development, likely because rifaximin’s local, concentrated action in the gut lumen overwhelms resistance mechanisms that would defeat systemic antibiotics at equivalent doses.
Some SIBO-focused practitioners use pulsed quarterly dosing (14 days every 3 months) in patients with refractory underlying motility disorders — systemic sclerosis, severe diabetic enteropathy, surgical blind loops. This is off-label, expensive, and should be reserved for cases where the root cause genuinely cannot be corrected.
8. Side Effects and Safety
Rifaximin’s side-effect profile is unusually mild for an antibiotic, and the reason is — again — that <0.4% systemic absorption. If the drug isn’t in your bloodstream, it can’t do much to the rest of you.
Most commonly reported in trials:
- Headache (~8%)
- Abdominal discomfort
- Nausea
- Dizziness (less common)
Clostridioides difficile association exists but is substantially lower than with systemic antibiotics like clindamycin or fluoroquinolones. Rifaximin is actually one of the safer antibiotics from a C. diff standpoint.
It’s safe in liver disease — in fact it’s a first-line treatment for hepatic encephalopathy in cirrhosis. Drug-drug interactions are minimal for the same low-absorption reason. It’s compatible with most cardiovascular, psychiatric, and endocrine medications without dose adjustment.
9. When Rifaximin Fails — What Next
Roughly a quarter to a third of patients don’t respond to the first course. Before concluding you’re a non-responder, work through this list:
- Confirm compliance and correct dosing. Some pharmacies substitute the wrong strength (200 mg tablets exist for traveler’s diarrhea — that’s not what you want). Verify you got the 550 mg strength and took all 42 doses on schedule.
- Repeat the breath test — including methane and hydrogen sulfide. A trio-smart retest often reveals that what looked like hydrogen SIBO was actually mixed methane or H2S. The original test may have missed it.
- If methane-positive now, add neomycin and retreat. The 28% monotherapy eradication rate for IMO explains a lot of “rifaximin failures.”
- If H2S-positive, try rifaximin + bismuth.
- Consider an elemental diet. See Elemental Diet — 80–85% eradication in the Pimentel trials, no antibiotic required.
- Consider a herbal rotation. See Herbal Antimicrobials — the Chedid 2014 trial showed head-to-head equivalence with rifaximin.
- Investigate the root cause. Migrating motor complex dysfunction, ileocecal valve issues, adhesions, post-infectious anti-vinculin antibodies, untreated hypothyroidism, chronic PPI use. See Root Causes. Without this step, every course of rifaximin is just buying you another 10–12 weeks.
10. When You Can’t Get Rifaximin (Alternatives)
If insurance, cost, or supply issues make rifaximin impossible, the following systemic antibiotics have evidence for SIBO — all with the caveat that they hit commensal flora harder and produce more side effects than rifaximin.
- Metronidazole 250 mg TID × 7–10 days — effective, cheap, alcohol absolutely contraindicated (disulfiram-like reaction), metallic taste, neuropathy risk with prolonged use.
- Ciprofloxacin 500 mg BID × 7 days — effective but carries the fluoroquinolone tendon-rupture and neuropsychiatric warnings. Reserve for patients who have tolerated fluoroquinolones previously.
- Amoxicillin-clavulanate 875/125 mg BID × 14 days — reasonable choice for proximal SIBO, well-tolerated, diarrhea is the main adverse effect.
- Trimethoprim-sulfamethoxazole (Bactrim DS BID × 7 days) — cheap, widely available, contraindicated in sulfa-allergic patients, watch for photosensitivity and rare Stevens-Johnson reactions.
All of these will disrupt the colonic microbiome more than rifaximin, and all increase C. difficile risk. Factor a probiotic reconstruction strategy and, ideally, a stool test at 4–6 weeks post-treatment.
11. Critical: Pair with a Prokinetic
This is the step most gastroenterologists skip, and it’s the reason SIBO relapses. Without addressing migrating motor complex (MMC) dysfunction, the relapse rate after rifaximin is 44–46% within 9–12 months. Adding a nightly prokinetic cuts that rate to roughly 20%.
Common options include low-dose erythromycin (50–100 mg at bedtime), low-dose naltrexone (2.5–4.5 mg), prucalopride (1–2 mg), and ginger extract. Full details, dosing, and pros/cons at Prokinetics & Relapse Prevention.
If you take nothing else away from this page: a successful rifaximin course without a prokinetic afterwards is a round-trip ticket back to the same symptoms by next quarter.
12. Key Research Papers
Pivotal trials and reviews establishing rifaximin's efficacy, dosing, and safety profile for SIBO and IBS, including the TARGET program and combination protocols. Each citation links to the full text via DOI.
- Pimentel M, Lembo A, Chey WD, et al. Rifaximin Therapy for Patients with Irritable Bowel Syndrome without Constipation (TARGET 1 and TARGET 2). New England Journal of Medicine. 2011;364(1):22–32.
- Lembo A, Pimentel M, Rao SS, et al. Repeat Treatment with Rifaximin Is Safe and Effective in Patients with Diarrhea-Predominant Irritable Bowel Syndrome (TARGET 3). Gastroenterology. 2016;151(6):1113–1121.
- Pimentel M, Park S, Mirocha J, Kane SV, Kong Y. The Effect of a Nonabsorbed Oral Antibiotic (Rifaximin) on the Symptoms of the Irritable Bowel Syndrome: A Randomized Trial. Annals of Internal Medicine. 2006;145(8):557–563.
- Pimentel M, Saad RJ, Long MD, Rao SSC. ACG Clinical Guideline: Small Intestinal Bacterial Overgrowth. American Journal of Gastroenterology. 2020;115(2):165–178.
- Rezaie A, Buresi M, Lembo A, et al. Hydrogen and Methane-Based Breath Testing in Gastrointestinal Disorders: The North American Consensus. American Journal of Gastroenterology. 2017;112(5):775–784.
- Low K, Hwang L, Hua J, Zhu A, Morales W, Pimentel M. A Combination of Rifaximin and Neomycin Is Most Effective in Treating Irritable Bowel Syndrome Patients with Methane on Lactulose Breath Test. Journal of Clinical Gastroenterology. 2010;44(8):547–550.
- Lauritano EC, Gabrielli M, Scarpellini E, et al. Small Intestinal Bacterial Overgrowth Recurrence after Antibiotic Therapy. American Journal of Gastroenterology. 2008;103(8):2031–2035.
- Yang J, Lee HR, Low K, Chatterjee S, Pimentel M. Rifaximin versus Other Antibiotics in the Primary Treatment and Retreatment of Bacterial Overgrowth in IBS. Digestive Diseases and Sciences. 2008;53(1):169–174.
- Gatta L, Scarpignato C. Systematic Review with Meta-Analysis: Rifaximin Is Effective and Safe for the Treatment of Small Intestinal Bacterial Overgrowth. Alimentary Pharmacology & Therapeutics. 2017;45(5):604–616.
- Bass NM, Mullen KD, Sanyal A, et al. Rifaximin Treatment in Hepatic Encephalopathy. New England Journal of Medicine. 2010;362(12):1071–1081.
- Pimentel M, Chow EJ, Lin HC. Eradication of Small Intestinal Bacterial Overgrowth Reduces Symptoms of Irritable Bowel Syndrome. American Journal of Gastroenterology. 2000;95(12):3503–3506.
- Chedid V, Dhalla S, Clarke JO, et al. Herbal Therapy Is Equivalent to Rifaximin for the Treatment of Small Intestinal Bacterial Overgrowth. Global Advances in Health and Medicine. 2014;3(3):16–24.
Live PubMed Searches
Live PubMed queries that update as new papers are indexed.
- PubMed: rifaximin for SIBO
- PubMed: rifaximin + neomycin for methane
- PubMed: Xifaxan for IBS-D
- PubMed: rifaximin retreatment
- PubMed: rifaximin safety profile
- PubMed: neomycin for SIBO
- PubMed: rifaximin + bismuth for H2S SIBO
- PubMed: rifaximin in hepatic encephalopathy
Connections
- The Gut Barrier & Your Microbiome — interactive animation
- SIBO Overview
- Elemental Diet
- Root Causes
- Herbal Antimicrobials
- Prokinetics and Relapse Prevention
- Hydrogen vs Methane vs Hydrogen Sulfide
- Low-FODMAP Diet
- Breath Test Guide
- IMO and Constipation
- Irritable Bowel Syndrome
- Gut Healing
- Probiotics
- Berberine
- Bloating
- Constipation
- IBS Medications Guide
- GERD
- Liver Disease