Low-FODMAP Diet for IBS
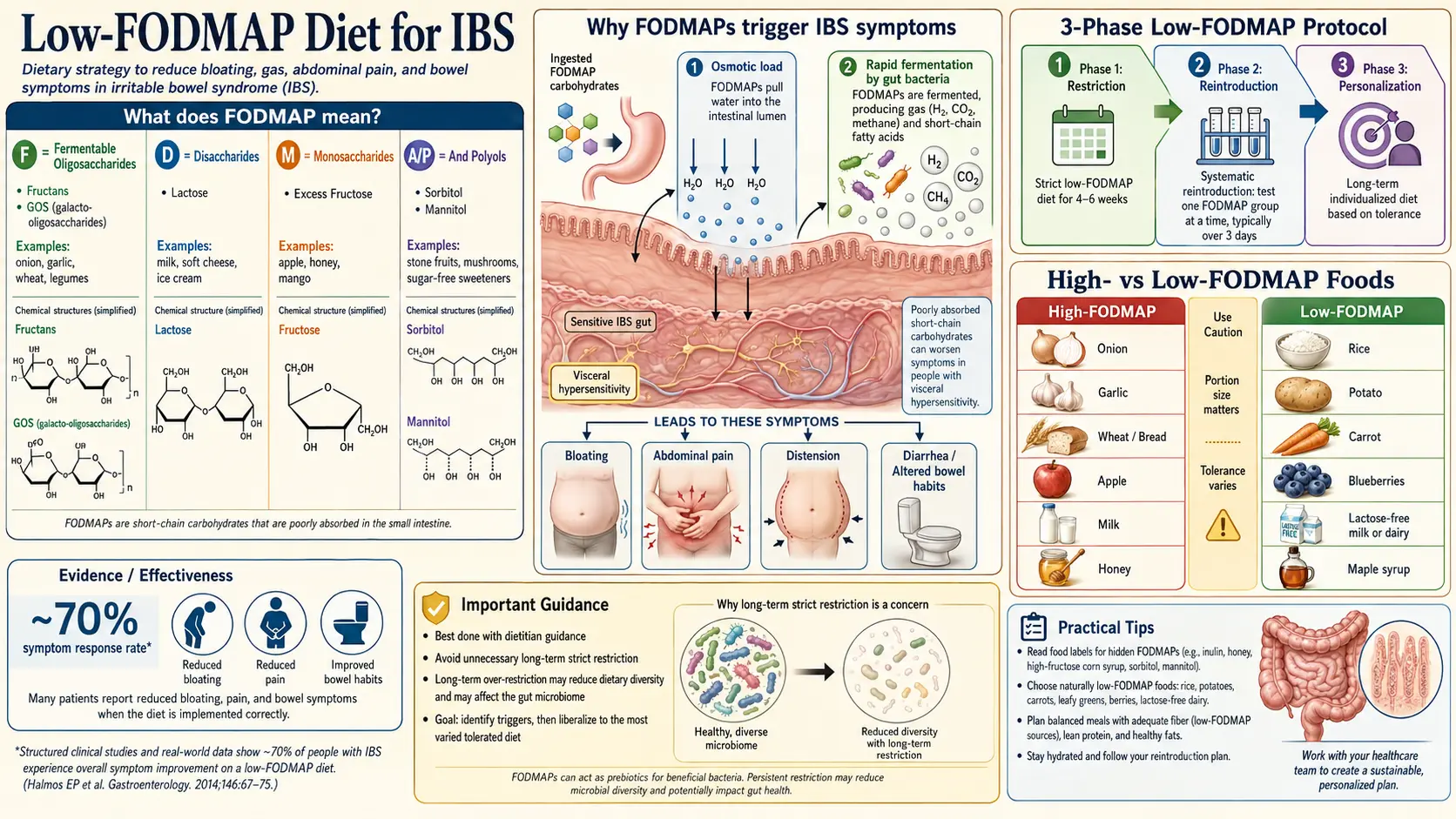
Table of Contents
- What FODMAPs Actually Are
- Why FODMAPs Trigger Symptoms
- Evidence and Response Rates
- The Monash Three-Phase Protocol
- Phase 1 — Strict Elimination (2–6 Weeks)
- Detailed Food Lists for the Elimination Phase
- Phase 2 — Systematic Reintroduction (About 8 Weeks)
- Phase 3 — Personalization
- FODMAP Stacking — The Principle Most People Miss
- The Monash App and Other Tools
- Practical Tactics: Oils, Brands, Eating Out
- Risks of a Prolonged Elimination Phase
- Why a Registered Dietitian Matters
- When Low-FODMAP Doesn't Work
- The Gluten-Free Overlap
- Key Research Papers
- Connections
- Featured Videos
What FODMAPs Actually Are
FODMAP is an acronym coined by the research team at Monash University in Melbourne, Australia, in the mid-2000s. It stands for Fermentable Oligosaccharides, Disaccharides, Monosaccharides, And Polyols. Those are four families of short-chain carbohydrates and sugar alcohols that share two inconvenient properties: your small intestine absorbs them poorly, and your colon bacteria love to ferment them.
The four groups, translated into food:
- Oligosaccharides — short chains of sugars. The two that matter are fructans (in wheat, rye, onion, garlic, leeks, shallots, artichokes) and galacto-oligosaccharides (GOS) (in most beans, lentils, chickpeas, cashews, and pistachios). Humans have no enzyme to split these bonds — everyone, IBS or not, passes them undigested into the colon.
- Disaccharides — specifically lactose, the milk sugar. Whether lactose is a problem depends on whether you still produce the enzyme lactase. Roughly 65% of adults worldwide lose most of their lactase activity after childhood.
- Monosaccharides — specifically fructose in excess of glucose. Fructose is absorbed efficiently when paired 1:1 with glucose (as in table sugar) but poorly when it floats free in high amounts (as in apples, pears, mangoes, honey, agave, and high-fructose corn syrup).
- Polyols — sugar alcohols such as sorbitol and mannitol, naturally abundant in stone fruits (plums, peaches, apricots, cherries), mushrooms, cauliflower, and sugar-free gum and candy sweetened with xylitol, maltitol, or erythritol.
Note what FODMAPs are not. They are not gluten, not dairy protein, not histamine, not lectins, not nightshades, not oxalates. They are one specific family of fermentable carbohydrates, and a low-FODMAP diet is designed to target that chemistry and nothing else.
Why FODMAPs Trigger Symptoms
Two mechanisms, both normal physiology pushed past a threshold.
Osmotic pull. FODMAPs are small, dissolved, and osmotically active. When they sit in the small intestine unabsorbed, they drag water in with them. In a healthy gut with normal motility, the extra fluid moves along without trouble. In an IBS gut — where the bowel wall is more reactive and motility is dysregulated — the added fluid stretches the small bowel and produces the characteristic cramping, urgency, and loose stools of IBS-D.
Rapid fermentation. Whatever reaches the colon still undigested becomes bacterial food. Colonic microbes ferment FODMAPs into short-chain fatty acids plus large volumes of gas — hydrogen, methane, and sometimes hydrogen sulfide. In healthy people this fermentation is slow and mostly comfortable. In IBS, the gas is produced faster than the colon can move or absorb it, the bowel distends, and nerve endings that are already too sensitive (see visceral hypersensitivity) fire as if something is badly wrong. That signal reaches the brain as pain and bloating.
Low-FODMAP is not a food-allergy diet. FODMAPs are not doing anything toxic, and your immune system is not producing antibodies against them. The diet simply reduces the substrate that feeds the mechanical and fermentative triggers, giving the gut less raw material to react to.
Evidence and Response Rates
The low-FODMAP diet is the most-studied dietary intervention for IBS and the one with the strongest evidence base of any single approach. Multiple randomized controlled trials and meta-analyses consistently report that 50 to 80 percent of IBS patients see a clinically meaningful reduction in symptoms — bloating, pain, gas, and stool urgency — during the elimination phase.
Halmos and colleagues (2014) ran the landmark feeding trial in which every meal was provided to participants, ruling out adherence problems. Overall gastrointestinal symptom scores fell significantly on the low-FODMAP arm compared with a typical Australian diet. Staudacher and colleagues (2017) extended this with a placebo-controlled trial comparing low-FODMAP plus placebo, low-FODMAP plus probiotic, and a sham diet plus placebo; the low-FODMAP arms beat sham. Bohn and colleagues (2015) in Sweden compared low-FODMAP against traditional IBS dietary advice (regular meals, reduced fat, less caffeine, less insoluble fiber) and found the two roughly equivalent — a useful finding because it suggests that for some patients the simpler traditional advice is enough.
The number needed to treat is in the range of 4 to 5, which is excellent for any IBS therapy. Response is usually apparent within one to two weeks and solid by week three or four.
The Monash Three-Phase Protocol
The Monash protocol — the only evidence-based version of this diet — is three distinct phases, and skipping any of them defeats the purpose.
- Phase 1 (Elimination): 2 to 6 weeks of strict low-FODMAP eating to see whether symptoms improve at all.
- Phase 2 (Reintroduction): roughly 8 weeks of systematic challenges, adding back one FODMAP subgroup at a time to learn which specific sugars trigger you and at what dose.
- Phase 3 (Personalization): a lifelong, modified diet that excludes only the subgroups and portions you personally tolerate poorly, while reintroducing everything else.
The diet was never designed to be followed strictly for the rest of your life. The elimination phase is a diagnostic tool, not a destination. The reintroduction phase is where the real information is gathered. The personalized phase is the goal.
Phase 1 — Strict Elimination (2–6 Weeks)
During Phase 1 you remove — or sharply reduce — every food known to contain significant FODMAPs. This means reading labels, cooking most meals at home, and accepting that restaurant eating will be awkward for a few weeks. Do not drift into a "mostly low-FODMAP" compromise; the whole point is to drop your FODMAP load below the reaction threshold, and partial compliance often gives ambiguous results.
Give it at least two weeks before judging, and up to six if your symptoms are severe or slow-responding. If you see clear improvement by week three or four, you know FODMAPs are a real trigger and you move on to Phase 2. If four to six weeks of genuine compliance produces no change at all, FODMAPs are probably not your primary driver, and you stop the diet and look elsewhere (see When It Doesn't Work).
Detailed Food Lists for the Elimination Phase
These lists are a practical starting point. The authoritative reference — updated as Monash re-tests foods in the lab — is the Monash University FODMAP Diet app. When the app and a generic web list disagree, trust the app.
What You Can Eat Freely
- Grains: basmati rice, jasmine rice, brown rice, quinoa, oats (plain rolled oats in modest portions), corn tortillas, sourdough spelt bread, gluten-free bread that is also onion- and garlic-free, rice noodles, buckwheat.
- Proteins: virtually all plain meats, poultry, fish, and seafood; eggs; firm tofu and tempeh (not silken tofu); small portions of canned lentils or chickpeas that have been drained and rinsed.
- Dairy and alternatives: hard cheeses (cheddar, parmesan, Swiss, brie, feta); lactose-free milk, yogurt, and ice cream; almond milk (unsweetened); small amounts of butter.
- Vegetables: carrots, cucumbers, zucchini, spinach, lettuce, kale, bell peppers (red/yellow/green in moderate portions), eggplant, green beans, bok choy, tomatoes, potatoes, sweet potato (about half a cup), parsnip, the green tops of scallions and leeks (not the white bulb), chives.
- Fruits: blueberries, strawberries, raspberries, oranges, grapes, kiwi, pineapple, cantaloupe, firm bananas (not overripe), lemons, limes. Portion matters — most fruits are low-FODMAP at one serving and high at two.
- Fats and extras: olive oil, all cooking oils, vinegars, most herbs and spices (not onion or garlic powder), maple syrup in small amounts, plain dark chocolate in small portions.
What to Avoid
- Wheat, rye, and barley in any substantial portion — bread, pasta, couscous, pastries, flour tortillas, cereal, crackers. The issue is the fructans, not the gluten.
- Onion and garlic in any form — raw, cooked, powdered, dehydrated, in stock cubes, in sauces, in seasonings. This single exclusion is harder than it looks; garlic and onion are hidden in nearly every packaged savory product.
- Most beans and legumes — black beans, kidney beans, pinto beans, soybeans, and large portions of lentils or chickpeas.
- High-FODMAP fruits: apples, pears, mangoes, watermelon, cherries, peaches, plums, apricots, nectarines, blackberries, dried fruit, fruit juice concentrates.
- High-FODMAP vegetables: cauliflower, mushrooms, asparagus, sugar snap peas, artichoke, beetroot in large portions, the white part of leeks, Jerusalem artichoke.
- Regular dairy: cow's milk, regular yogurt, ice cream, soft cheeses such as ricotta and cottage cheese, condensed milk.
- Sweeteners: honey, agave, high-fructose corn syrup, and any sugar alcohol ending in -ol (sorbitol, mannitol, xylitol, maltitol, isomalt, erythritol is better tolerated but still a polyol). Sugar-free gum and mints are a classic hidden source.
- Cashews and pistachios — the two high-GOS nuts. Almonds, walnuts, peanuts, macadamia, and pecans are fine in modest portions.
Phase 2 — Systematic Reintroduction (About 8 Weeks)
Phase 2 is the phase people skip, and skipping it is the single biggest mistake in low-FODMAP dieting. Without reintroduction, you never learn which specific FODMAPs actually bother you — and most people only react to two or three of the six subgroups, not all of them.
The method: continue the low-FODMAP baseline, then pick one FODMAP subgroup and test it on day 1, day 3, and day 5 of a week, at increasing doses, while logging symptoms. Between tests and between subgroups, return to a strict low-FODMAP diet for a few days so any reaction clearly belongs to the most recent challenge.
A standard test schedule, one subgroup per week:
- Week 1 — Mannitol: half a cup of button mushrooms, then one cup, then one and a half cups.
- Week 2 — Sorbitol: five blackberries, then ten, then half a cup.
- Week 3 — Lactose: half a cup of milk, then one cup, then one and a half cups.
- Week 4 — Fructose: half a teaspoon of honey, then one teaspoon, then one tablespoon.
- Week 5 — Fructans (wheat): one slice of wheat bread, then two, then three.
- Week 6 — Fructans (onion/garlic): a quarter of a small onion, then half, then a whole one.
- Week 7 — GOS: a quarter cup of chickpeas, then half, then three-quarters.
- Week 8 — Recheck and combine: re-test anything ambiguous, or start combining tolerated subgroups.
The result is a personal map. You will probably discover that one or two subgroups give you trouble at any dose, one or two give you trouble only at larger portions, and the rest you tolerate fine. That map is the whole point of the diet.
Phase 3 — Personalization
Phase 3 is the rest of your life. You keep whatever you learned in Phase 2 and build a diet that excludes, or limits, only your personal triggers. For most people this means one or two permanent restrictions (often onion, garlic, or apples/pears) and otherwise a broadly varied diet.
Every three to six months it is worth re-challenging a previously poorly-tolerated FODMAP. Gut physiology changes with time, stress, infections, and hormone cycles, and tolerances drift. Something that triggered symptoms last year may be fine now.
FODMAP Stacking — The Principle Most People Miss
FODMAPs add up. A single food may be rated "low-FODMAP" at one portion because it contains only a small amount of, say, fructans. Eat three different low-FODMAP fructan-containing foods at the same meal — a slice of sourdough, a bowl of lentil soup, and a cup of sugar snap peas — and the combined fructan load can cross your threshold and trigger symptoms even though no single item was "high" on the list.
This is FODMAP stacking, and it explains most "but I ate only low-FODMAP foods and still felt awful" complaints. Keep variety within a meal, don't pile multiple moderate sources of the same subgroup, and watch total daily load. The Monash app flags stacking risk when you log a meal.
The Monash App and Other Tools
The Monash University FODMAP Diet app (iOS and Android, one-time purchase around $10 USD) is the single indispensable tool. The Monash team physically tests foods in their laboratory and assigns a traffic-light rating (green, amber, red) at specific serving sizes. No other source is as accurate. Use it for grocery shopping, restaurant decisions, and Phase 2 challenges.
Secondary tools worth owning:
- A food and symptom diary — paper or an app like Bowelle, Cara Care, or mySymptoms. Phase 2 is impossible to interpret without written records.
- The Monash-certified product list — packaged foods Monash has tested and approved for low-FODMAP.
- A registered dietitian who has been trained in the Monash protocol (see the dietitian section).
Practical Tactics: Oils, Brands, Eating Out
The garlic and onion oil trick. Fructans are water-soluble, not oil-soluble. That means you can cook garlic cloves or onion chunks in olive oil, then remove and discard the solids, and keep the infused oil. The oil carries the flavor; the FODMAPs stayed behind in the solids you threw out. Garlic-infused olive oil is a kitchen staple on low-FODMAP and the single most important flavor rescue. Commercial garlic-infused oils are widely available; check that garlic pieces are not still suspended in the bottle.
Pre-made products. Fody Foods is the largest U.S. brand dedicated to low-FODMAP pantry items — pasta sauces, salsas, ketchups, broths, taco seasonings, all made without onion or garlic. Other Monash-certified brands include Rachel Pauls Food, Casa de Sante, and FreeFrom. These save enormous time in the elimination phase, particularly for sauces and soup bases, where hidden onion and garlic otherwise dominate.
Eating out. Three tactics:
- Choose cuisines that can accommodate you. Plain grilled meats plus rice and vegetables (steakhouse, Japanese, Korean barbecue, some Thai) are easier than heavily sauced cuisines. Indian and Italian are hardest because of onion-garlic bases.
- Ask targeted questions. Say "I have a medical restriction on onion and garlic — does the sauce contain either?" rather than "I'm on a low-FODMAP diet," which servers rarely understand.
- Eat before you go, or bring a small snack. If the restaurant has only two safe items, it is kinder to yourself to pre-eat something solid and treat the restaurant as a social venue.
Risks of a Prolonged Elimination Phase
Staying in Phase 1 indefinitely — as many patients do when nobody walks them through Phase 2 — causes real harm.
- Nutrient gaps. Long-term low-FODMAP eating can reduce calcium (from restricted dairy), fiber (from restricted wheat, fruit, and legumes), folate, thiamine, and some B vitamins. Studies show measurable drops in several micronutrients after six months of strict elimination.
- Microbiome reduction. FODMAPs are prebiotics. They feed beneficial bacteria, particularly Bifidobacteria. Several studies, including Halmos and Staudacher, have documented significant reductions in Bifidobacterium abundance after three to four weeks of strict low-FODMAP. We do not fully know the long-term consequences, but feeding your gut flora less of their preferred fuel for years is biologically unlikely to be neutral.
- Disordered eating risk. Any restrictive diet carries a risk of triggering or worsening orthorexia, particularly in patients with prior eating-disorder history. If food fear is escalating, stop the diet and talk to a clinician.
- Social cost. Strict elimination constrains meals out, travel, and family eating. That cost is acceptable for a few weeks of diagnostic clarity; it becomes corrosive over years.
Reintroduction is not optional. The entire point of Phase 1 is to earn the right to do Phase 2.
Why a Registered Dietitian Matters
If you can possibly afford one visit — even a single session covered by insurance or paid out of pocket — work with a registered dietitian trained specifically in the low-FODMAP protocol. Monash runs a training course, and their website lists certified dietitians by country.
A good dietitian does three things a book or app cannot. First, they catch nutrient shortfalls early — adjusting your calcium and fiber intake before deficits build. Second, they design a Phase 2 reintroduction schedule that fits your life rather than a textbook. Third, they keep you honest about exiting Phase 1 on time, which is the single most common failure mode of self-guided low-FODMAP attempts.
In the U.S., many gastroenterology practices now employ or refer to GI-specialized dietitians. Telehealth options make this accessible even in rural areas. Insurance coverage varies; if your plan does not cover nutrition counseling, one to two self-paid visits across the whole three-phase journey is usually enough.
When Low-FODMAP Doesn't Work
Roughly one in four IBS patients gets little or no benefit from a properly executed low-FODMAP trial. If you are one of them, it is a useful data point, not a failure. It means FODMAPs are not your main driver, and the answer lies elsewhere.
Common alternative drivers to investigate next:
- Small intestinal bacterial overgrowth (SIBO) — bacteria have migrated into the small bowel and ferment almost anything you eat, not just FODMAPs. Low-FODMAP may give partial short-term relief but never full relief because the underlying overgrowth is still there. A breath test and antibiotic or herbal treatment comes first. See the IBS and SIBO overlap article and the fuller SIBO overview plus its own low-FODMAP notes.
- Mast cell activation syndrome (MCAS) and histamine intolerance — symptoms are driven by mast-cell mediator release and by dietary histamine, not by fermentable sugars. Many supposedly "safe" low-FODMAP foods (aged cheese, spinach, tomatoes, fermented foods) are high-histamine. A low-histamine trial often works where low-FODMAP did not. See the MCAS page.
- Bile acid diarrhea — unabsorbed bile salts irritate the colon and cause urgent morning diarrhea. Responds dramatically to a bile-acid sequestrant such as colestipol or colesevelam; does not respond to low-FODMAP at all.
- Celiac disease — never assume IBS without serologic screening. See Celiac Disease.
- Alpha-gal syndrome — a delayed allergy to mammalian meat caused by tick bites, easily mistaken for IBS because symptoms arrive hours after eating. See Alpha-Gal Syndrome.
- Brain-gut hypersensitivity — when visceral nerves are the main amplifier, dietary changes alone rarely help enough. Gut-directed hypnotherapy and CBT carry evidence comparable to low-FODMAP. See hypnotherapy and CBT.
The Gluten-Free Overlap
A large fraction of people who "went gluten-free and felt better" did not actually react to gluten. Wheat is simultaneously the largest source of gluten and one of the largest sources of fructans in the Western diet. When they stopped eating wheat, they lost both at once — and for the majority, the improvement was the fructans, not the gluten.
Nanayakkara and colleagues (2016) and later studies on non-celiac wheat sensitivity have consistently shown that most self-identified "gluten-sensitive" patients without celiac disease respond to fructan restriction at least as well as to gluten restriction, often better. Rule out celiac disease properly first (blood tests plus, if positive or high suspicion, endoscopic biopsy while you are still eating gluten). If celiac is excluded and symptoms persist, a structured low-FODMAP trial is a more informative next step than an open-ended gluten-free diet. See Celiac Disease and the broader Elimination Diet page.
Key Research Papers
- Halmos EP, et al. A diet low in FODMAPs reduces symptoms of irritable bowel syndrome. Gastroenterology. 2014.
- Staudacher HM, et al. A diet low in FODMAPs reduces symptoms in patients with irritable bowel syndrome and a probiotic restores Bifidobacterium species: a randomized controlled trial. Gastroenterology. 2017.
- Böhn L, et al. Diet low in FODMAPs reduces symptoms of irritable bowel syndrome as well as traditional dietary advice: a randomized controlled trial. Gastroenterology. 2015.
- Nanayakkara WS, et al. Efficacy of the low FODMAP diet for treating irritable bowel syndrome: the evidence to date. Clin Exp Gastroenterol. 2016.
Live PubMed Searches
For further reading, the following PubMed topic searches return current peer-reviewed work on FODMAPs, IBS diet, and related mechanisms:
- Low-FODMAP diet and IBS
- FODMAP reintroduction and personalization phase
- FODMAP diet and microbiome / Bifidobacterium
- Fructans and non-celiac wheat sensitivity
- Lactose intolerance and IBS
- Fructose malabsorption and IBS
- Polyols, sorbitol, mannitol and IBS
- Low-FODMAP diet and dietitian-led counseling
Connections
- The Gut Barrier & Your Microbiome — interactive animation
- Irritable Bowel Syndrome
- Low-FODMAP Diet for SIBO
- SIBO
- Celiac Disease
- IBS and SIBO Overlap
- MCAS
- Alpha-Gal Syndrome
- Elimination Diet
- Gut-Directed Hypnotherapy and CBT
- Visceral Hypersensitivity and Brain-Gut Axis
- Peppermint, Probiotics, and Herbals
- Rome IV Subtypes
- Post-Infectious IBS
- IBS Medications Guide
- Low-Histamine Diet
- Gluten-Free Diet Guide
- Bloating
- Yogurt
- High Resistant Starch Foods — food rankings by RS grams per serving, the cook-and-cool RS3 protocol, a daily ~20g meal plan, and butyrate/SCFA mechanism.