Endometriosis
Deep-Dive Articles
Endometriosis is under-diagnosed for an average of 7–10 years, under-treated with hormonal band-aids, and misunderstood even by gynecologists. The eight guides below each tackle one piece — why diagnosis takes so long, the excision-vs-ablation surgery debate, the full menu of hormonal options, why pelvic floor PT is a game changer, the adenomyosis overlap, the endo-belly gut connection, fertility planning, and the diet/lifestyle evidence. Start wherever you are.
Diagnosis Delay & Imaging
Why the average diagnosis takes 7–10 years, the limits of transvaginal ultrasound, when MRI with deep-infiltrating protocols helps, and scripts for pushing a skeptical gyn toward diagnostic laparoscopy.
Excision vs. Ablation
The surgery that actually removes endo (excision / LAPEX) vs. the one that burns the surface (ablation / fulguration), why recurrence rates differ, how to find a true excision surgeon, and what to expect in recovery.
Hormonal Therapy Options
Continuous combined OCPs, progestin-only (norethindrone, dienogest / Visanne), Mirena IUD, GnRH agonists (leuprolide), GnRH antagonists (elagolix, relugolix combos), aromatase inhibitors — dose, cost, side effects, and who each option fits.
Pelvic Floor & Central Sensitization
Why pain continues after surgery, pelvic floor dysfunction & hypertonicity, central pain sensitization, finding a pelvic PT, internal vs. external work, and the home dilator / wand / breathing protocols that move the needle.
Endometriosis & Adenomyosis
The cousin condition — endometrial tissue inside the uterine muscle. How it overlaps with endometriosis (about 40% of patients have both), how MRI distinguishes them, and why treatment differs.
Endo Belly & Gut Connection
The dramatic bloating that makes you look 5 months pregnant by evening, SIBO and IBS overlap, the gut-endo axis, bowel endometriosis, low-FODMAP trials, and when to work up gut symptoms separately.
Fertility & Endometriosis
How endometriosis affects conception, when to see REI, excision-before-IVF debates, IVF protocols tuned for endo (ultra-long GnRH suppression), endometriomas and ovarian reserve, and timelines for family-building.
Diet & Lifestyle
Anti-inflammatory eating, dairy and gluten elimination trials, omega-3s, curcumin / resveratrol / NAC evidence, reducing xenoestrogen exposure, and the sleep / stress / exercise basics that compound over months.
Bladder & Bowel Endometriosis
Deep infiltrating endo, cyclic hematuria/dyschezia, and expert-center surgical decisions.
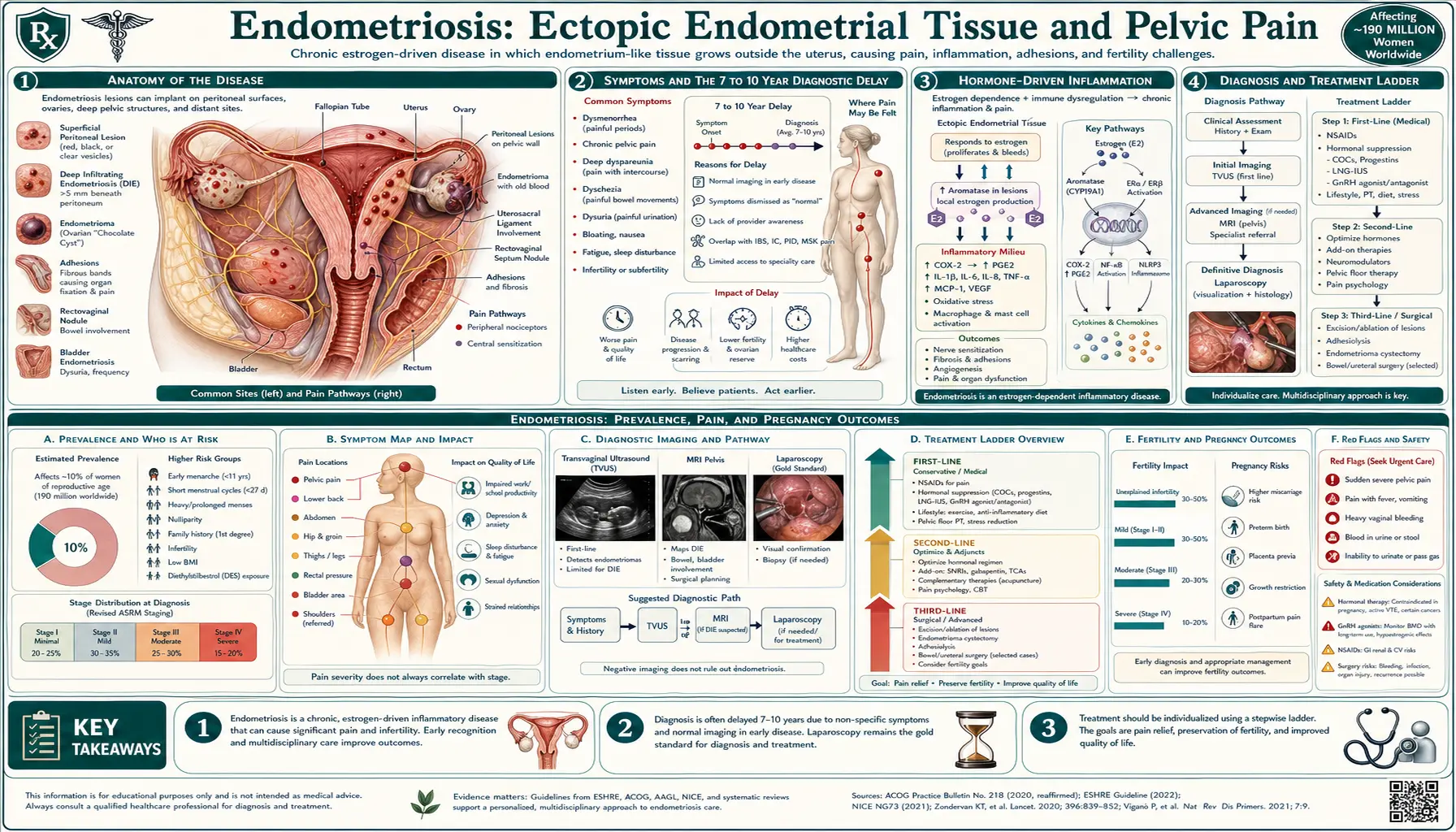
What is Endometriosis?
Endometriosis is a chronic condition where tissue similar to the lining of the uterus (endometrium) grows outside the uterus. This abnormal tissue growth can cause pain, inflammation, and the formation of scar tissue. Endometriosis most commonly affects the ovaries, fallopian tubes, and the tissue lining the pelvis but can spread beyond these areas in severe cases.
Common Symptoms of Endometriosis
- Pelvic pain: Often associated with menstrual periods but can occur at other times as well.
- Painful periods (dysmenorrhea): Pain can start before and extend several days into a period.
- Heavy menstrual bleeding or bleeding between periods.
- Pain during intercourse
- Painful bowel movements or urination: Particularly during menstrual periods.
- Infertility: Endometriosis can make it difficult to conceive.
- Fatigue, bloating, nausea, and constipation, especially during periods.
Causes and Risk Factors
- Retrograde menstruation: Menstrual blood containing endometrial cells flows back through the fallopian tubes into the pelvic cavity.
- Genetic predisposition: Having a family member with endometriosis increases risk.
- Hormonal factors: Estrogen is known to promote endometriosis growth.
- Immune system disorders: An impaired immune response may fail to detect and destroy endometrial-like tissue outside the uterus.
- History of pelvic infection
Diagnosis
- Medical history and physical examination: To assess symptoms and pelvic abnormalities.
- Ultrasound: Uses high-frequency sound waves to create images of the pelvic organs.
- Magnetic resonance imaging (MRI): Provides detailed images to identify endometrial tissue.
- Laparoscopy: A minimally invasive surgical procedure that allows direct visualization and biopsy of endometrial tissue.
Treatment Options
- Pain management:
- Over-the-counter pain relievers: Such as ibuprofen or naproxen to relieve pain.
- Hormonal therapy:
- Birth control pills: To regulate or stop menstruation and reduce pain.
- Gonadotropin-releasing hormone (GnRH) agonists: To reduce estrogen levels and slow endometrial tissue growth.
- Progestin therapy: Helps counteract the effects of estrogen on endometrial tissue.
- Conservative surgery:
- Laparoscopic excision: Removes as much endometrial tissue as possible while preserving reproductive organs.
- Hysterectomy:
- Removal of the uterus: Considered a last resort for severe cases when other treatments are ineffective.
- Fertility treatments: For those struggling with infertility due to endometriosis, options include in vitro fertilization (IVF).
Prevention and Management Strategies
- Maintain a balanced diet: Anti-inflammatory foods may help reduce symptoms.
- Exercise regularly: Helps manage pain and reduce stress.
- Limit alcohol and caffeine: May help decrease estrogen levels.
- Manage stress: Techniques like yoga and meditation can aid in managing chronic pain.
Complications of Endometriosis
- Infertility: Up to 30-40% of women with endometriosis may experience difficulties conceiving.
- Chronic pain: Persistent pain can impact quality of life and mental health.
- Adhesions and scar tissue: Can cause organs to stick together, leading to pain and potential complications.
- Ovarian cysts (endometriomas): May form on the ovaries and can cause discomfort.
8. References & Research
Historical Background
Endometriosis was first described by Czech pathologist Karl von Rokitansky in 1860, who identified ectopic endometrial tissue outside the uterus. John Sampson popularized the retrograde menstruation theory in 1927, which remains one of the leading hypotheses for the disease's pathogenesis.
Key Research Papers
- Taylor HS, Kotlyar AM, Flores VA. Endometriosis is a chronic systemic disease: clinical challenges and novel innovations. The Lancet. 2021;397(10276):839-852.
- Giudice LC, Kao LC. Endometriosis. The Lancet. 2004;364(9447):1789-1799.
- Bulun SE. Endometriosis. New England Journal of Medicine. 2009;360(3):268-279.
- Vercellini P, Vigano P, Somigliana E, Fedele L. Endometriosis: pathogenesis and treatment. Nature Reviews Endocrinology. 2014;10(5):261-275.
- Johnson NP, Hummelshoj L; World Endometriosis Society Montpellier Consortium. Consensus on current management of endometriosis. Human Reproduction. 2013;28(6):1552-1568.
- Sampson JA. Peritoneal endometriosis due to menstrual dissemination of endometrial tissue into the peritoneal cavity. American Journal of Obstetrics and Gynecology. 1927;14(4):422-469.
- Nnoaham KE, Hummelshoj L, Webster P, et al. Impact of endometriosis on quality of life and work productivity: a multicenter study across ten countries. Fertility and Sterility. 2011;96(2):366-373.
- Zondervan KT, Becker CM, Missmer SA. Endometriosis. New England Journal of Medicine. 2020;382(13):1244-1256.
- Dunselman GA, Vermeulen N, Becker C, et al. ESHRE guideline: management of women with endometriosis. Human Reproduction. 2014;29(3):400-412.
- Zondervan KT, Becker CM, Koga K, Missmer SA, Taylor RN, Vigano P. Endometriosis. Nature Reviews Disease Primers. 2018;4:9.
- Chapron C, Marcellin L, Borghese B, Santulli P. Rethinking mechanisms, diagnosis and management of endometriosis. Nature Reviews Endocrinology. 2019;15(11):666-682.
- Kennedy S, Bergqvist A, Chapron C, et al. ESHRE guideline for the diagnosis and treatment of endometriosis. Human Reproduction. 2005;20(10):2698-2704.
Table of Contents
Research Papers
The following PubMed topic searches aggregate the current peer-reviewed literature. Each link opens a live PubMed query — results update as new studies are indexed.
- PubMed — endometriosis
- PubMed — endometriosis pathogenesis
- PubMed — deep infiltrating endometriosis
- PubMed — endometriosis infertility
- PubMed — endometriosis laparoscopy
- PubMed — GnRH agonist endometriosis
- PubMed — dienogest endometriosis
- PubMed — endometriosis pain management
- PubMed — adenomyosis
- PubMed — endometrioma ovarian
- PubMed — endometriosis diet
- PubMed — endometriosis recurrence
Connections
- Reproductive Medicine
- Dysmenorrhea (Menstrual Cramps)
- Laparoscopy: Excision vs Ablation
- Hormonal Therapy Options
- Adenomyosis Overlap
- Bladder and Bowel Endometriosis
- Diagnosis Delay and Imaging
- Pelvic Floor Therapy and Central Sensitization
- Fertility and Endometriosis
- Endo Belly and Gut Connection
- Diet and Lifestyle
- Infertility
- Ovarian Cysts
- Perimenopause
- Uterine Fibroids
- Menopause and HRT
- Vitamin D3
- Magnesium
- Polycystic Ovary Syndrome
- Chronic Pain
- Ovarian Cancer
- PMS and PMDD
- Valerian for Menstrual Cramps — herbal adjunct for the cramp and sleep burden of pelvic pain.