POTS Medications Guide
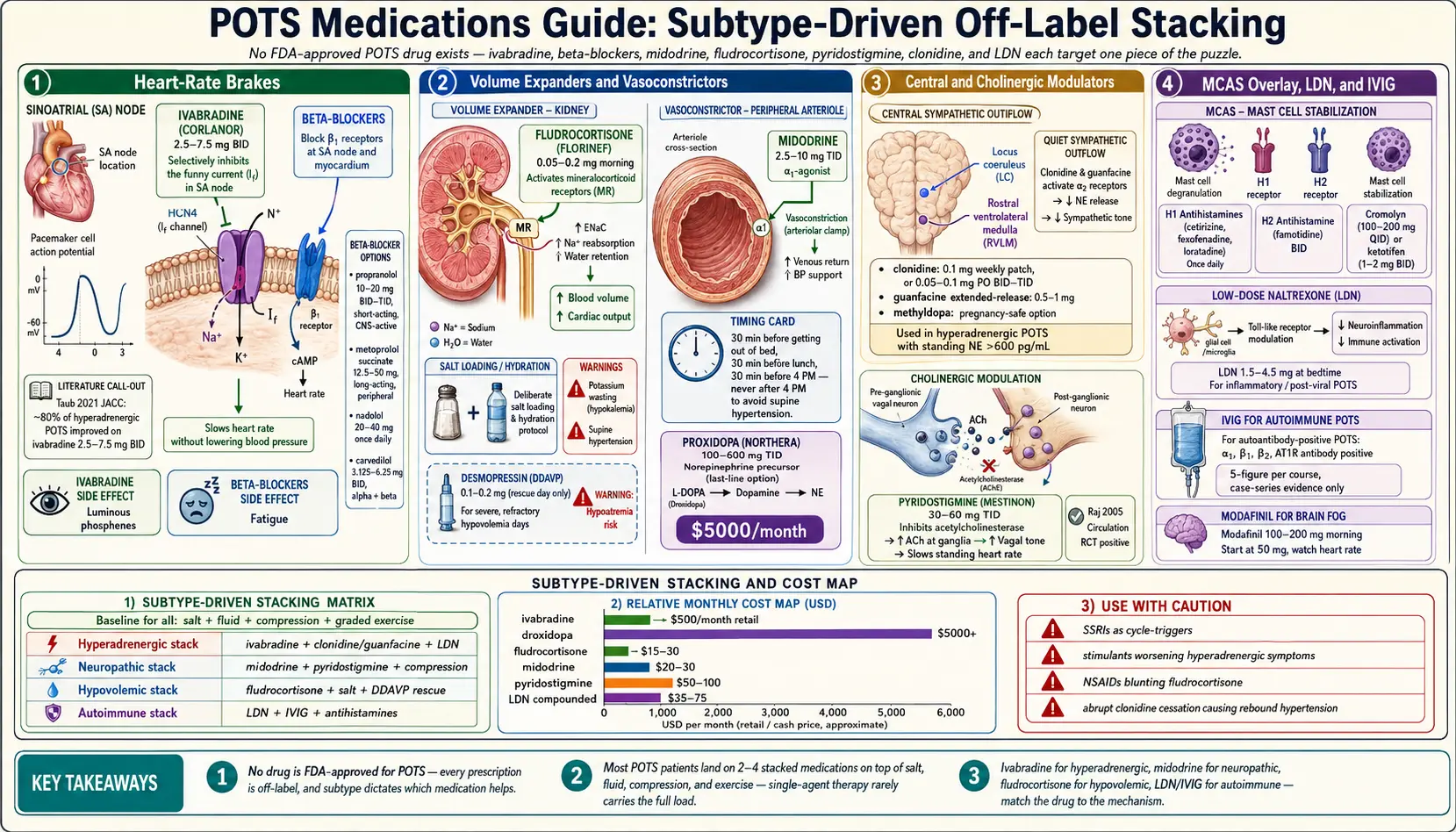
Table of Contents
- There Is No “POTS Drug”
- Heart-Rate-Focused Meds
- Blood-Volume-Focused Meds
- Vasoconstrictor Meds
- Central-Acting Meds
- Cholinergic Meds
- Mast Cell / Allergic Overlay
- Specialty & Emerging
- Stacking Protocols by Subtype
- Avoid or Use With Caution
- Insurance Navigation Tips
- How to Know a Med Is Working
- Key Research Papers
- Research Papers
- Connections
- Featured Videos
1. There Is No “POTS Drug”
Here is the uncomfortable truth every POTS patient eventually learns: there is no FDA-approved medication for postural orthostatic tachycardia syndrome. Not one. Every prescription your cardiologist or neurologist writes for you — ivabradine, midodrine, fludrocortisone, propranolol, pyridostigmine, clonidine — is used off-label. That word matters because it shapes insurance denials, pharmacist questions, and how much hand-holding you get when you fill the script.
The reason this field is so fragmented is that POTS isn’t one disease. It’s a shared final pathway — standing heart rate rises ≥30 bpm — reached by at least four different underlying mechanisms. That’s why your friend got midodrine and you got ivabradine, and why both of you might be correctly treated. Subtype drives drug choice. See Subtypes for the full breakdown.
The other reality: most POTS patients end up on 2–4 medications stacked, plus salt, fluid, compression, and exercise. A single pill rarely carries the full load. Think of this guide as a map of tools, not a decision tree where you pick the one right answer.
2. Heart-Rate-Focused Meds
These drugs target the tachycardia itself — the fast standing heart rate that defines POTS. They don’t fix blood volume or vasoconstriction; they just put the brakes on the pulse.
Ivabradine (Corlanor)
Ivabradine is the holy grail for hyperadrenergic POTS and increasingly the first-line choice across subtypes when insurance allows. It inhibits the funny (If) current in the sinoatrial node, which slows heart rate without lowering blood pressure and without the fatigue hit of beta-blockers. For patients whose standing BP is already borderline low, that specificity is the difference between tolerating the drug and being crushed by it.
Typical dose: 2.5–7.5 mg twice daily. Start at 2.5 mg BID and titrate every 2 weeks by pulse response. The Taub 2021 randomized trial (JACC) showed roughly 80% of hyperadrenergic POTS patients improved meaningfully on ivabradine — the best head-to-head number in the field.
Cost: Retail runs around $500/month, but Amgen’s copay program and most commercial insurers cover it when a POTS or inappropriate sinus tachycardia diagnosis is documented. Expect a prior authorization battle the first time.
Side effects: The signature one is luminous phosphenes — brief visual flashes or halos, especially when looking at bright lights. They usually fade in a few weeks. Bradycardia happens if overdosed; if your resting pulse drops below 50, cut the dose. Ivabradine is contraindicated in atrial fibrillation and severe hepatic impairment.
Beta-Blockers
Before ivabradine arrived, beta-blockers were the default for POTS, and they’re still the cheapest, most widely available option. The trade-off is that they lower blood pressure along with heart rate, and they sap energy in some patients — a real problem when fatigue is already the dominant symptom.
Propranolol 10–20 mg BID-TID is the most commonly prescribed. Short-acting, crosses the blood-brain barrier, which helps if anxiety overlaps the POTS picture and hurts if fatigue already dominates. Low doses (10 mg) are often enough; don’t let a cardiologist reflex to 40 mg TID.
Metoprolol succinate 12.5–50 mg daily is long-acting and mostly stays out of the brain — a gentler option for patients who get foggy on propranolol. The succinate (extended-release) form gives smoother coverage than tartrate.
Nadolol 20–40 mg daily is very long-acting and non-selective, which makes it useful for patients who wake up at 3 AM in a tachycardia surge. One dose covers the full 24-hour cycle.
Carvedilol 3.125–6.25 mg BID combines alpha and beta blockade. Good for the hyperadrenergic patient with wildly swinging blood pressures — the alpha effect damps the pressor spikes that pure beta-blockers can’t touch.
Side effects across the class: fatigue (huge issue in POTS — this is the main reason patients migrate to ivabradine), bronchospasm in asthmatics, worsening of depression, reduced exercise tolerance, cold hands and feet. Never stop a beta-blocker abruptly; taper over a week.
3. Blood-Volume-Focused Meds
Many POTS patients are chronically hypovolemic — measurably low circulating plasma volume, often 10–30% below normal. Raising volume raises preload and drops the compensatory tachycardia. Salt and fluid are the foundation; these drugs are the pharmacologic amplifier.
Fludrocortisone (Florinef)
Fludrocortisone is a synthetic mineralocorticoid. It tells the kidneys to retain sodium, which pulls water with it and expands plasma volume. Works best when paired with deliberate salt loading (see Salt & Hydration Protocol) — no sodium in, nothing for the drug to act on.
Typical dose: 0.05–0.2 mg every morning. Start at 0.05 mg and titrate by symptoms and labs. Doses above 0.2 mg rarely help more and rapidly increase side effects.
Cost: Cheap generic, about $15–30/month.
Best for: Hypovolemic subtype and low-renin patients (some POTS specialists draw a renin/aldosterone ratio before starting to confirm).
Side effects: Potassium wasting is the big one — supplement with potassium-rich foods or a low-dose K+ tablet, and check a basic metabolic panel at 2 weeks, then every 3 months. Edema, weight gain, supine hypertension, and headache are common. Long-term use can suppress the HPA axis; don’t stop abruptly.
Desmopressin (DDAVP)
Desmopressin is a synthetic vasopressin analog. It tells the kidneys to hold water, rapidly expanding volume. This is a rescue medication, not a daily med — pulse dosing only, for days you know will be brutal (long flights, weddings, heat waves).
Typical dose: 0.1–0.2 mg orally as needed, once daily maximum.
Do not use daily. Chronic use can produce dangerous hyponatremia — sodium levels low enough to seize on. If a patient is using DDAVP more than 2–3 times a week, the regimen needs a rethink.
4. Vasoconstrictor Meds
In the neuropathic POTS phenotype, standing causes too much blood to pool in the lower body because small peripheral vessels don’t constrict properly. Vasoconstrictor drugs put the squeeze back on those vessels, pushing blood back toward the heart.
Midodrine (ProAmatine)
Midodrine is an alpha-1 adrenergic agonist. It binds directly to the peripheral vasculature and makes small arteries clamp down. It’s the workhorse for neuropathic POTS — cheap, effective, and fast-acting (onset in 30 minutes, duration 3–4 hours).
Typical dose: 2.5–10 mg three times daily. Start at 2.5 mg TID and titrate.
Timing is non-negotiable. Midodrine works for a short window, so schedule it around the day:
- 30 minutes before getting out of bed (set an alarm, take it, lie back down)
- 30 minutes before lunch
- 30 minutes before 4 PM
- Last dose by 4 PM — take it any later and you risk supine hypertension when you lie down at night
Cost: Generic, roughly $20–30/month.
Side effects: The famous one is scalp tingling or goosebumps — harmless, just the alpha receptors on scalp and skin doing their job. Supine hypertension is the real risk; never take a dose and then go lie down. Urinary retention can occur in older men with prostatic hypertrophy.
Droxidopa (Northera)
Droxidopa is a synthetic norepinephrine precursor that the body converts into NE. It’s FDA-approved for neurogenic orthostatic hypotension (Parkinson’s, multiple system atrophy, pure autonomic failure) — not POTS. In pure POTS it’s reserved for refractory cases where midodrine has failed and volume expansion isn’t enough.
Typical dose: 100–600 mg three times daily.
Cost: Brutal. Retail runs $5,000+/month. Insurance approval for POTS (versus nOH) is a fight. Lundbeck’s patient assistance program is worth applying to.
5. Central-Acting Meds
Hyperadrenergic POTS is driven by too much sympathetic output from the brain — standing norepinephrine levels often exceed 600 pg/mL. Central alpha-2 agonists quiet the sympathetic outflow upstream, before it reaches the heart and vessels.
Clonidine
Clonidine is an alpha-2 agonist that acts in the brainstem to reduce norepinephrine release. It’s the go-to for hyperadrenergic POTS when ivabradine alone isn’t enough.
Typical dose: 0.1 mg weekly patch (preferred — smooth 7-day levels with no peak-trough swings), or 0.05–0.1 mg orally BID-TID.
The oral form’s sedation makes bedtime dosing ideal — it knocks out the middle-of-the-night adrenergic surges that wake hyperadrenergic patients drenched in sweat.
Side effects: Dry mouth (very common), drowsiness, orthostatic dizziness if dosed too aggressively, and — critically — rebound hypertension if stopped abruptly. Always taper clonidine over a week or more.
Guanfacine
Guanfacine is clonidine’s better-behaved cousin — same mechanism, less sedation, longer half-life. Patients who can’t tolerate clonidine’s drowsiness often do well on guanfacine.
Typical dose: 0.5–1 mg daily, extended-release preferred.
Methyldopa
Methyldopa is an older centrally acting agent, now mostly used because it’s pregnancy-safe. If a pregnant POTS patient needs symptom control, methyldopa is one of the few options with a long track record.
6. Cholinergic Meds
Pyridostigmine (Mestinon)
Pyridostigmine is an acetylcholinesterase inhibitor — it blocks the enzyme that breaks down acetylcholine, leaving more ACh available at neuromuscular junctions and (crucially for POTS) at autonomic ganglia. The net effect is enhanced vagal tone, which slows heart rate selectively during standing without lowering it to dangerous levels at rest.
Typical dose: 30–60 mg three times daily. Start at 30 mg once or twice daily to assess GI tolerance, then escalate.
Evidence: The Raj 2005 randomized trial (Circulation) demonstrated significant reduction in standing heart rate on pyridostigmine compared to placebo — one of the few POTS meds with a positive RCT.
Side effects: Cholinergic as expected — abdominal cramping, diarrhea, increased salivation, occasional muscle twitching. Start low and escalate slowly to limit GI effects. Pyridostigmine is a quiet favorite because it often works even when adrenergic-targeted drugs have failed.
7. Mast Cell / Allergic Overlay
An underappreciated reality: many POTS patients also have mast cell activation syndrome (MCAS). If flushing, itching, food reactions, or unexplained anaphylaxis-like episodes sit alongside the orthostatic symptoms, treating the mast cells often improves the POTS — sometimes dramatically.
The typical stack is H1 blocker (cetirizine, fexofenadine, or loratadine daily) + H2 blocker (famotidine BID) + a mast cell stabilizer (cromolyn or ketotifen). Low-dose naltrexone fits here too. For the full workup and treatment map see POTS-MCAS-EDS Triad and MCAS.
8. Specialty & Emerging
Low-Dose Naltrexone (LDN)
LDN is used at 1.5–4.5 mg nightly for inflammatory and autoimmune-leaning POTS phenotypes — especially post-viral cases where cytokine dysregulation appears central. Works on both neuroinflammation and mast cells. Full detail at Low-Dose Naltrexone for POTS.
Intravenous Immunoglobulin (IVIG)
IVIG is reserved for autoantibody-positive POTS — patients with demonstrated adrenergic receptor autoantibodies (alpha-1, beta-1, beta-2) or angiotensin II type 1 receptor (AT1R) antibodies. Dramatic responders exist and they can be life-changing cases, but the evidence base is case-series rather than randomized trials. Infusion-center logistics and cost (five figures per course) mean this is a last-line option, not a first move.
Modafinil (Provigil)
Modafinil 100–200 mg in the morning gets used off-label for POTS brain fog. Evidence is mixed — some patients love it, others find it amplifies tachycardia and jitter. If you try it, start at 50 mg and watch the heart rate.
9. Stacking Protocols by Subtype
Real-world POTS treatment is layered. Here are sample stacks that map cleanly to the four main subtypes — each one assumes baseline salt, fluid, compression, and graded exercise are already in place.
| Subtype | Core Stack | Notes |
|---|---|---|
| Hyperadrenergic | Ivabradine + clonidine patch + LDN | Avoid high-dose salt (can worsen BP spikes). Monitor for supine HTN. |
| Neuropathic | Midodrine + fludrocortisone + pyridostigmine + compression + salt | The classic “pool in the legs” phenotype. Vasoconstriction + volume is the goal. |
| Hypovolemic | Fludrocortisone + high-dose salt/fluid ± midodrine | Check renin/aldosterone; many of these patients have low renin. |
| Mixed / post-viral | Start ivabradine or low-dose propranolol → add midodrine if needed → address MCAS/autoimmune | Work the triggering infection and immune activation, not just the tachycardia. |
These are templates, not prescriptions. The right stack comes from repeated tilt-table or NASA lean tests, a careful symptom diary, and — importantly — a POTS-literate clinician willing to iterate.
10. Avoid or Use With Caution
Some commonly prescribed meds make POTS worse. Know these before you walk into a primary care visit.
- SSRIs. They help some patients (especially with comorbid anxiety) and wreck others — particularly the hyperadrenergic subtype, where pushing serotonin can amplify sympathetic tone. Sertraline 25–50 mg is the most commonly tried; start low, watch the heart rate.
- Stimulants (Adderall, Vyvanse, Ritalin). Frequently prescribed for “brain fog” and frequently disastrous. They raise heart rate and blood pressure directly. Reserve only for treatment-resistant fog after everything else has been tried, and dose at the floor of the therapeutic range.
- Tricyclics (amitriptyline, nortriptyline). Heavy anticholinergic burden, orthostatic hypotension, sedation. Rarely the right choice for a POTS patient.
- Proton-pump inhibitors (PPIs). Chronic acid suppression feeds SIBO, and SIBO commonly worsens autonomic symptoms. If you need one, use the shortest course possible.
- Opioids. Cause constipation, which slows gut transit, which feeds SIBO, which feeds autonomic dysfunction. The cascade is real.
11. Insurance Navigation Tips
Most POTS meds are cheap generics — midodrine, fludrocortisone, pyridostigmine, propranolol, clonidine, metoprolol. The two that will generate friction are ivabradine (~$500/month retail) and droxidopa ($5,000+/month). Here’s how to tilt the odds.
- Use the POTS-specific ICD-10 code: G90.A. “Postural orthostatic tachycardia syndrome” got its own code in 2022. Before that, claims were coded under generic autonomic dysfunction (G90.9) or orthostatic hypotension (I95.1) — both of which insurers flag as vague. G90.A is specific enough that prior auth reviewers can’t pretend they don’t know the diagnosis.
- Attach tilt-table or 10-minute NASA lean test results. Objective hemodynamic documentation is worth more than any narrative. See Tilt Table & NASA Lean Test.
- Cite the 2015 Heart Rhythm Society consensus statement. It explicitly endorses most of the off-label regimens used in POTS.
- Use manufacturer copay cards. Amgen’s Corlanor program and Lundbeck’s Northera assistance both exist; neither is advertised well.
- Find a POTS specialist. Dysautonomia International maintains a vetted list. POTS-literate clinicians handle prior authorizations in their sleep; generalist offices often don’t know where to start.
12. How to Know a Med Is Working
Don’t trust vibes. POTS symptoms fluctuate day to day with weather, hormones, hydration, and sleep, so a “good week” doesn’t mean the drug is working and a “bad day” doesn’t mean it isn’t. Use objective markers:
- Drop in standing heart rate by at least 15 bpm on repeat NASA lean test
- Drop in symptom diary scores across 2–4 weeks (brain fog, presyncope, fatigue, palpitations)
- Ability to complete a 10-minute NASA lean test without crashing
- Functional capacity gain — standing longer in the shower, tolerating errands, returning to part-time work
Give each new med 4–6 weeks at the target dose before deciding. Shorter trials mistake noise for signal. And when you do stop something, change one variable at a time — otherwise you’ll never know which drug was earning its keep.
13. Key Research Papers
- Taub PR, et al. Randomized trial of ivabradine in patients with hyperadrenergic postural orthostatic tachycardia syndrome. JACC. 2021;77(7):861-871.
- Raj SR, et al. Acetylcholinesterase inhibition improves tachycardia in postural tachycardia syndrome. Circulation. 2005;111(21):2734-2740.
- Raj SR, et al. Postural tachycardia syndrome (POTS): review. Circulation. 2013.
- Sheldon RS, et al. 2015 Heart Rhythm Society expert consensus statement on the diagnosis and treatment of POTS. Heart Rhythm. 2015.
14. Research Papers
Curated PubMed topic searches — each link opens a live query so you always see the most recent literature.
- PubMed: Ivabradine for POTS
- PubMed: Midodrine for postural tachycardia
- PubMed: Fludrocortisone for POTS
- PubMed: Pyridostigmine for POTS
- PubMed: Propranolol for postural tachycardia
- PubMed: Clonidine for hyperadrenergic POTS
- PubMed: Droxidopa for orthostatic syndromes
- PubMed: POTS autoantibodies and IVIG
Connections
- POTS Overview
- POTS Subtypes
- LDN for POTS
- Tilt Table Test
- Salt and Hydration Protocol
- POTS/MCAS/EDS Triad
- Compression and Exercise Program
- Vagus Nerve and Autonomic Retraining
- MCAS
- SIBO
- Arrhythmia
- Low-Dose Naltrexone (Remedy)
- Thyroid Disorders
- Fibromyalgia
- ME/CFS
- Fatigue
- Lightheadedness
- Orthostatic Intolerance in ME CFS