Mast Cell Activation Syndrome (MCAS): The Underdiagnosed Allergic-Autonomic Condition
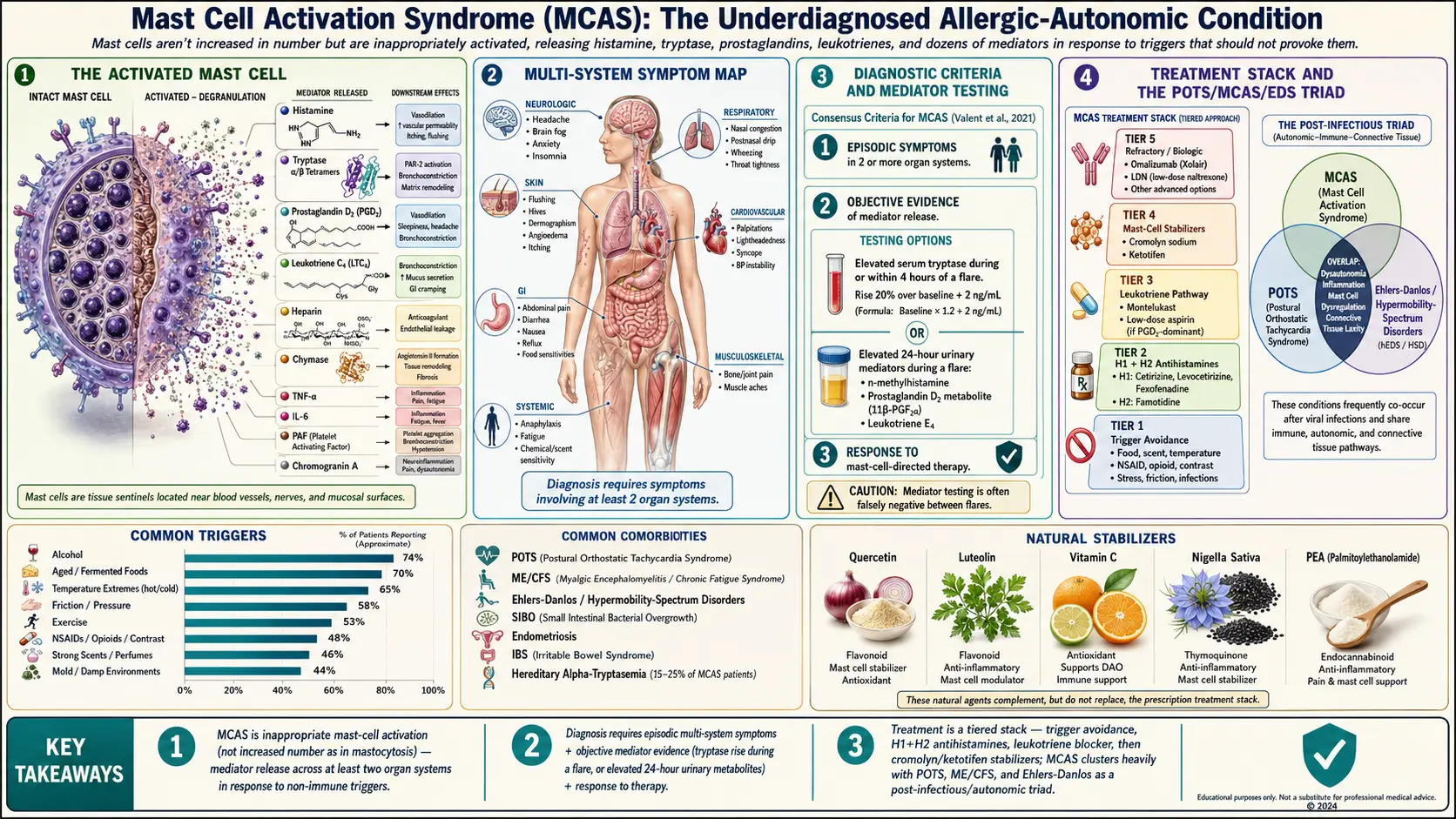

Mast cell activation syndrome (MCAS) is a condition in which mast cells — immune cells that mediate allergic responses — are not numerically increased (as they are in mastocytosis) but are inappropriately activated, releasing histamine, tryptase, leukotrienes, prostaglandins, and dozens of other mediators in response to triggers that should not provoke them. The result is a multi-system illness that affects skin, gastrointestinal tract, cardiovascular and respiratory systems, and nervous system. MCAS is often triggered or unmasked by infections (including EBV and COVID-19), physical trauma, pregnancy, or hormonal transitions, and it clusters heavily with POTS and ME/CFS.
Deep-Dive Articles
MCAS is a diagnosis where most patients end up managing themselves — the workup is slow, the specialists are few, and the day-to-day tradeoffs (what to eat, which antihistamines to stack, when to escalate) fall on you. The eight articles below cover the pieces in plain language: how to test for it, how to eat, how to medicate, how to prevent flares, and where the natural-medicine layer actually helps.
Mediators & Symptom Map
Histamine, tryptase, prostaglandin D2, leukotrienes, heparin, chromogranin A — what each chemical mast cells release actually does in your body, and which symptoms point to which mediator. The key to targeted treatment.
MCAS Testing Guide
Serum tryptase, 24-hour urine N-methylhistamine, prostaglandin D2, leukotriene E4, chromogranin A. When to draw during a flare, why most tests come back “normal” even when you’re clearly reacting, and what the Consensus-1 and Consensus-2 criteria require.
Low-Histamine Diet
The complete food lists, DAO enzyme supplementation, histamine liberators (foods that don’t contain histamine but make your body release its own), fresh-is-best rules, leftovers as poison, and why this is a short-term tool, not a life sentence.
H1/H2 Blocker Stacks
Cetirizine, fexofenadine, loratadine, hydroxyzine, famotidine, ranitidine (gone), Xyzal, Benadryl — which antihistamines do what, morning vs. night dosing, the H1+H2 combo, and when to double up safely.
Cromolyn & Ketotifen Protocols
Second-line stabilizers for when antihistamines aren’t enough. Oral cromolyn sodium (Gastrocrom) dosing, compounded ketotifen, titration schedules, side-effect management, and how to find a compounding pharmacy.
Triggers & Flare Management
How to build a trigger diary that actually reveals your pattern, the most common culprits (heat, friction, stress, hormonal cycles, specific foods, exercise), and a step-by-step flare rescue plan before and during an episode.
Hereditary α-Tryptasemia
A genetic duplication of the TPSAB1 gene that drives elevated baseline tryptase and mimics MCAS. Testing, what the diagnosis changes, and how it overlaps with EDS and POTS.
Natural Mast Cell Stabilizers
Quercetin, luteolin, vitamin C, nigella sativa, holy basil, PEA. Dosing, product-quality notes, and how they stack with prescription antihistamines. The evidence-based natural layer.
Hormone Sensitivity & Menstrual Flares
Why estrogen triggers mast cells — cyclic flares, pregnancy, perimenopause.
What MCAS Is
Mast cells normally release their granule contents only in response to specific allergen-IgE binding or genuine pathogen signals. In MCAS, they degranulate repeatedly in response to non-immunologic triggers — heat, cold, stress, friction, certain foods, certain medications, exercise, and even emotional stimuli. The downstream effects cascade across systems because mast cells sit at tissue interfaces throughout the body — skin, gut mucosa, blood-vessel walls, respiratory tract, and perivascular nervous tissue.
Multi-System Symptoms
Symptoms typically span at least two organ systems and fluctuate:
- Skin: flushing, hives, itching, dermographism (skin writing), angioedema
- Gastrointestinal: abdominal pain, diarrhea, nausea, reflux, bloating, food sensitivities
- Cardiovascular: palpitations, lightheadedness, syncope, blood-pressure instability
- Respiratory: nasal congestion, postnasal drip, wheezing, throat tightness
- Neurologic: headache, brain fog, anxiety, insomnia
- Musculoskeletal: bone and joint pain, muscle aches
- Systemic: anaphylaxis, fatigue, chemical/scent sensitivity
Diagnostic Criteria
Consensus criteria require all three:
- Episodic symptoms consistent with mast-cell mediator release affecting at least two organ systems.
- Objective evidence of mast-cell mediator release — elevated serum tryptase measured during or within 4 hours of a symptomatic episode, or elevated 24-hour urinary n-methyl-histamine, prostaglandin D2 metabolite, or leukotriene E4.
- Response to mast-cell-directed therapy.
In practice, mediator measurement is often falsely negative because labs are typically drawn between flares. The clinical picture and therapeutic response are often the most meaningful signals.
Common Triggers
- Alcohol, aged/fermented foods, histamine-rich foods
- Temperature extremes, hot showers, sun exposure
- Physical pressure, vibration, friction
- NSAIDs, opioids, radiocontrast, certain antibiotics
- Strong scents, chemicals, mold
- Stress, including emotional
- Exercise
- Hormonal fluctuation (menstrual, pregnancy, menopause)
- Infections — viral and bacterial
Workup
- Serum tryptase (baseline and during flare) — >20% rise above baseline + 2 ng/mL during flare is highly suggestive.
- 24-hour urinary n-methyl-histamine, prostaglandin D2 metabolite, leukotriene E4 (chilled transport).
- Total and specific IgE, allergy evaluation.
- KIT D816V mutation analysis to exclude systemic mastocytosis.
- Evaluation for POTS, EDS/hypermobility, and autoimmune overlap.
Treatment — The Stepped Approach
- H1 antihistamines — cetirizine, loratadine, fexofenadine at standard doses, titrating upward as needed (sometimes 2–4x standard).
- H2 antihistamines — famotidine, added to H1.
- Mast-cell stabilizers — cromolyn sodium oral solution before meals, ketotifen.
- Leukotriene inhibitors — montelukast, zafirlukast.
- Quercetin as a natural mast-cell stabilizer (see Quercetin).
- Vitamin C — aids quercetin recycling and has some antihistamine effect.
- Aspirin at low dose for flushing (only with tolerance confirmed).
- Omalizumab for severe refractory cases.
- Emergency epinephrine for patients with history of anaphylaxis.
Low-Histamine Diet
Short-term (2–4 weeks) elimination of high-histamine and histamine-releasing foods often reveals how large a contribution diet is making. Avoid: aged cheeses, cured meats, fermented foods (kimchi, sauerkraut, kombucha), alcohol, vinegar-containing products, tomatoes, spinach, eggplant, citrus, avocado, nuts, shellfish, and leftovers more than 24 hours old. Favor freshly prepared, fresh meats, non-citrus fruits, rice, gluten-free grains. Low-histamine diet is a diagnostic and symptom-management tool, not a lifelong sentence — reintroduction under control is part of the protocol.
Overlap with POTS, ME/CFS, and EDS
MCAS, POTS, and Ehlers-Danlos syndrome / hypermobility spectrum disorder form the classic “triad.” ME/CFS sits adjacent. Screening for the other members of the cluster when one is diagnosed is now standard practice. Proposed shared mechanisms include mast-cell–autonomic interactions in perivascular tissue, connective-tissue fragility affecting autonomic ganglia, and shared post-infectious pathophysiology.
Table of Contents
- Deep-Dive Articles
- What MCAS Is
- Multi-System Symptoms
- Diagnostic Criteria
- Common Triggers
- Workup
- Treatment — The Stepped Approach
- Low-Histamine Diet
- Overlap with POTS, ME/CFS, and EDS
- Research Papers
- Connections
- Featured Videos
Research Papers
Curated PubMed topic searches on MCAS (Mast Cell Activation Syndrome). Each link opens a live PubMed query so the result set stays current as new studies are indexed.
- PubMed topic search: Mast cell activation syndrome review
- PubMed topic search: MCAS diagnostic criteria
- PubMed topic search: Tryptase MCAS
- PubMed topic search: H1 H2 antihistamines MCAS
- PubMed topic search: Cromolyn sodium MCAS
- PubMed topic search: Ketotifen mast cell
- PubMed topic search: Hereditary alpha tryptasemia
- PubMed topic search: MCAS hEDS POTS overlap
- PubMed topic search: Mastocytosis review
- PubMed topic search: Omalizumab mast cell
- PubMed topic search: Low histamine diet
- PubMed topic search: Idiopathic MCAS clinical
Connections
- Natural Mast Cell Stabilizers
- Mediators and Symptom Map
- MCAS Testing Guide
- Low-Histamine Diet
- H1 and H2 Blocker Stacks
- Cromolyn and Ketotifen Protocols
- Triggers and Flare Management
- Hereditary Alpha-Tryptasemia
- Hormone Sensitivity and Menstrual Flares
- POTS
- ME/CFS
- Fibromyalgia
- Ehlers-Danlos Syndrome
- SIBO
- Alpha-Gal Syndrome
- Hashimoto's Thyroiditis
- Quercetin
- Inflammatory Markers