Inflammatory Bowel Disease (IBD)
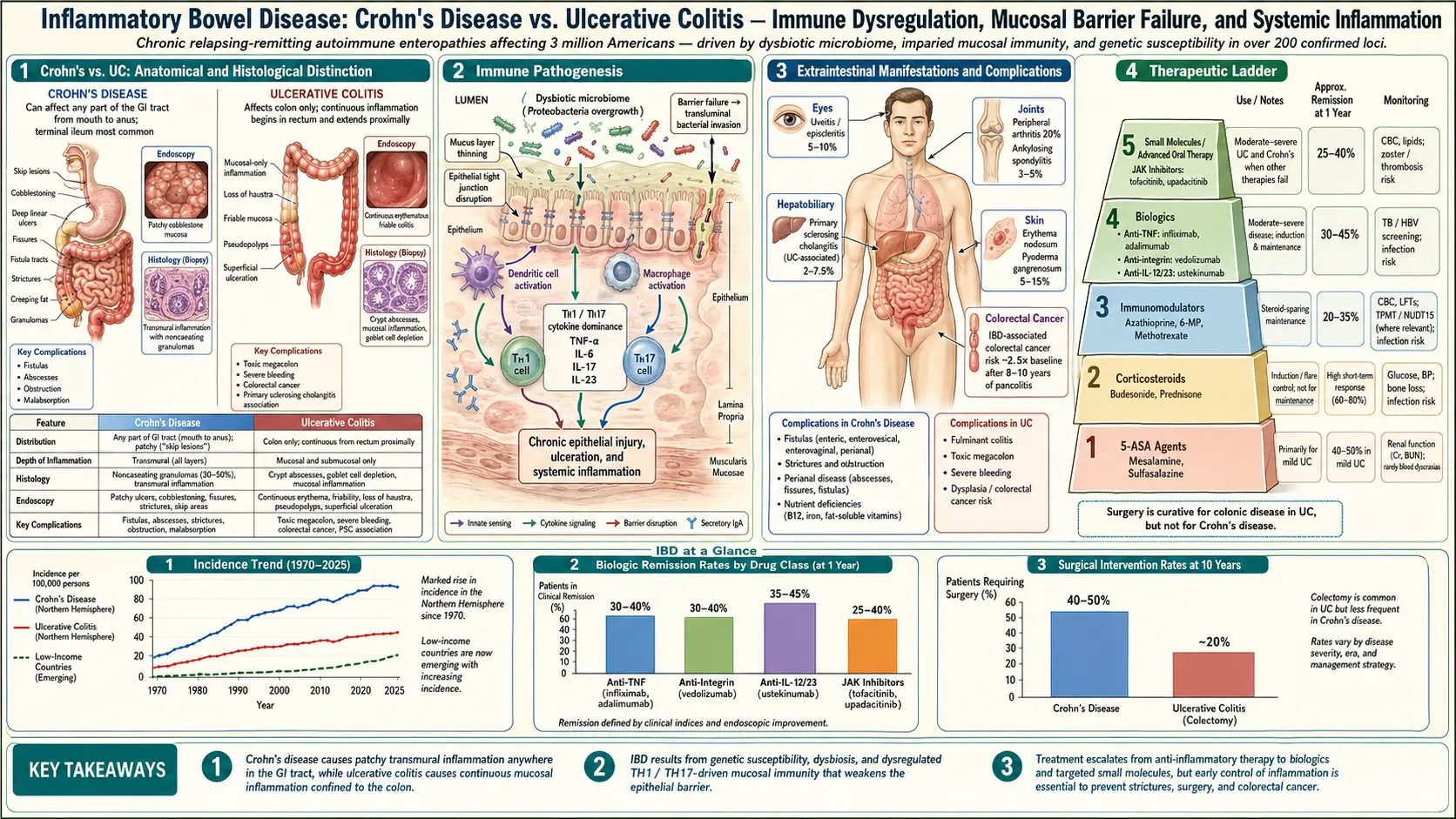
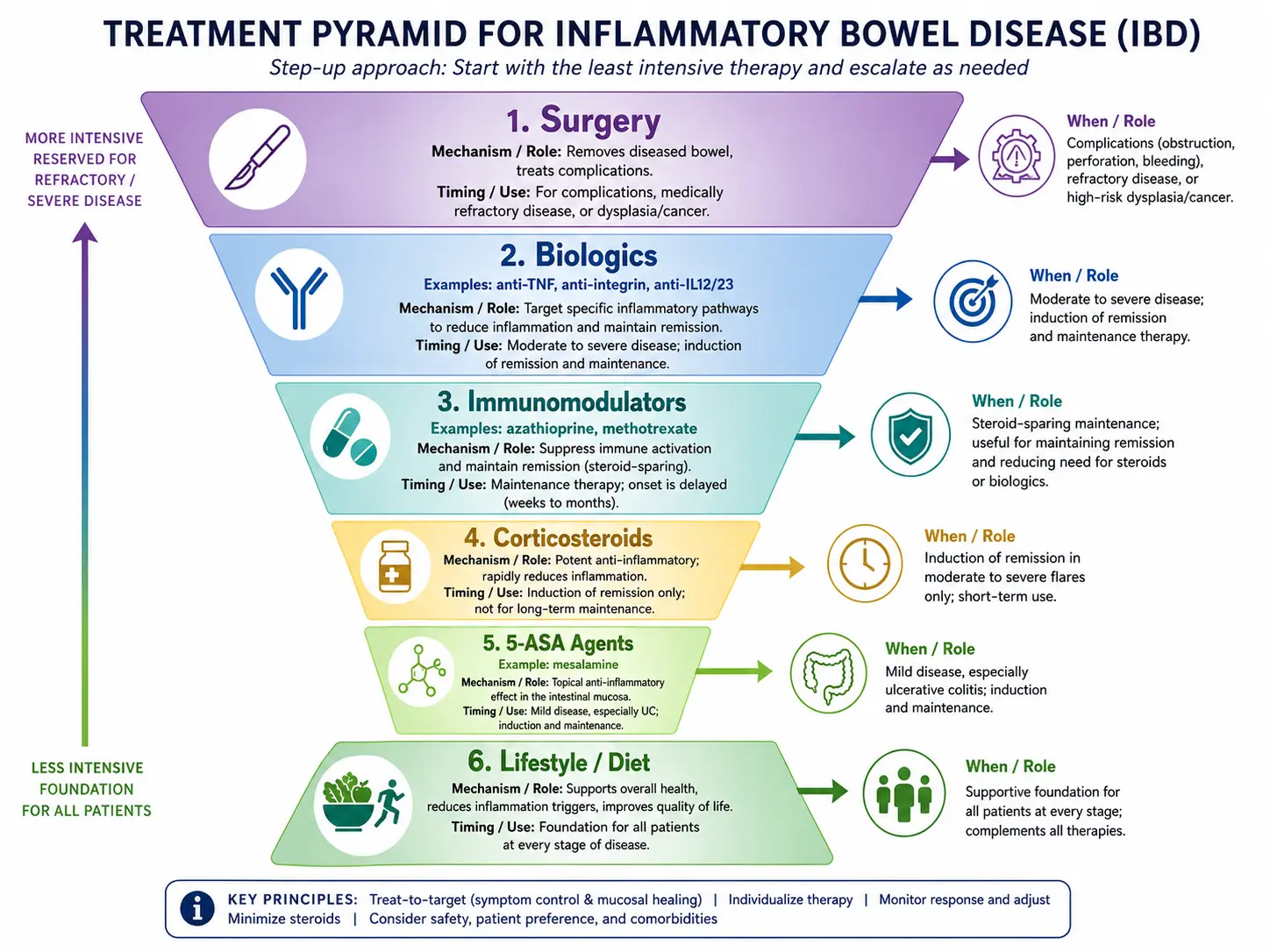

Table of Contents
- Deep-Dive Articles
- What is Inflammatory Bowel Disease (IBD)?
- Types of IBD
- Common Symptoms of IBD
- Causes and Risk Factors
- Diagnosis
- Treatment Options
- Prevention and Management Strategies
- Complications of IBD
- Research Papers
- Connections
- Featured Videos
Deep-Dive Articles
The articles below go beyond this overview into diagnosis, biologics, diet, surgery, and the extraintestinal side of IBD. Written for patients and caregivers, with real research citations.
Crohn's vs Ulcerative Colitis
Location, depth of inflammation, skip lesions vs continuous disease, and why the distinction drives treatment choice.
Diagnostic Workup
Fecal calprotectin, colonoscopy with biopsy, MR enterography, and how to tell IBD from IBS or infection.
Biologics: TNF, IL-23, Integrins
Infliximab, adalimumab, ustekinumab, risankizumab, vedolizumab — how each class works, side-effect profile, and sequencing.
JAK Inhibitors & S1P Modulators
Tofacitinib, upadacitinib, ozanimod, etrasimod — oral small molecules for UC, when they fit, and the black-box warnings.
Diet for IBD
Specific Carbohydrate Diet, Mediterranean, CDED, and enteral nutrition — what the trials actually show.
Surgery Decisions
Ileocecal resection, colectomy with J-pouch, ostomy — when surgery is the right call and what life looks like after.
Extraintestinal Manifestations
Arthritis, uveitis, erythema nodosum, PSC — the IBD symptoms that show up outside the gut.
Fatigue, Anemia & Nutrients
Iron deficiency, B12, vitamin D, and why fatigue persists even when inflammation is controlled.
Pregnancy & IBD
Fertility, which biologics and small molecules are safe in pregnancy and lactation, flare risk, and PIANO-registry data.
What is Inflammatory Bowel Disease (IBD)?
Inflammatory Bowel Disease (IBD) is an umbrella term used to describe chronic inflammatory conditions of the gastrointestinal (GI) tract. The two main types of IBD are Crohn's disease and ulcerative colitis. Both conditions involve long-term inflammation that can cause damage to the digestive tract.
Types of IBD
1. Crohn's Disease
- Can affect any part of the GI tract, from the mouth to the anus, but most commonly affects the end of the small intestine (ileum) and the beginning of the colon.
- Inflammation can occur in patches, with healthy tissue in between.
- May involve all layers of the bowel wall.
2. Ulcerative Colitis
- Affects only the colon and rectum.
- Inflammation is continuous, starting from the rectum and extending proximally.
- Typically affects only the innermost lining of the colon.
Common Symptoms of IBD
Symptoms can range from mild to severe and may include:
- Persistent diarrhea
- Abdominal pain and cramping
- Blood in the stool
- Unintended weight loss
- Fatigue
- Reduced appetite
- Urgency to have a bowel movement
Causes and Risk Factors
- Genetics: Family history of IBD increases the risk.
- Immune system response: An abnormal immune response may trigger inflammation in the GI tract.
- Environmental factors: Higher incidence in developed countries; diet and lifestyle may play a role.
- Age: Most commonly diagnosed before age 30 but can develop at any age.
- Smoking: Particularly linked to Crohn's disease.
Diagnosis
- Medical history and physical examination: To assess symptoms and possible risk factors.
- Endoscopic procedures: Such as colonoscopy or sigmoidoscopy to visualize the inside of the colon and take tissue samples.
- Imaging tests: MRI or CT scans to identify areas of inflammation or complications in the GI tract.
- Blood tests: To check for anemia or signs of infection.
- Stool tests: To rule out infections and detect inflammation markers.
Treatment Options
- Medications:
- Aminosalicylates (5-ASAs): Help reduce inflammation in mild to moderate cases.
- Corticosteroids: Used for short-term flare-up management to reduce inflammation.
- Immunosuppressants: Such as azathioprine and methotrexate to control immune system activity.
- Biologic therapies: Target specific parts of the immune system (e.g., infliximab, adalimumab).
- Antibiotics: To treat or prevent infections related to IBD.
- Dietary changes: Modifying diet to identify and avoid trigger foods.
- Stress management: Stress-reduction techniques such as mindfulness and relaxation exercises.
- Surgery:
- For Crohn's disease: May involve removal of diseased portions of the intestine.
- For ulcerative colitis: Colectomy (removal of the colon) may be curative.
Prevention and Management Strategies
- Maintain a balanced diet: Emphasize nutrient-dense foods and avoid known triggers.
- Stay hydrated
- Avoid smoking: Can exacerbate symptoms, especially in Crohn's disease.
- Regular exercise: Helps manage stress and overall well-being.
- Medication adherence: Consistently take prescribed medications to control inflammation.
Complications of IBD
- Bowel obstruction: Chronic inflammation can lead to scarring and narrowing of the intestines.
- Fistulas: Abnormal connections between different parts of the intestine or between the intestine and other organs.
- Abscesses: Pockets of infection in the abdomen or rectal area.
- Colon cancer: Increased risk, especially with long-term ulcerative colitis.
- Malnutrition: Due to decreased nutrient absorption.
- Primary sclerosing cholangitis: A rare condition causing liver damage, more common in people with ulcerative colitis.
9. References & Research
Historical Background
Inflammatory bowel disease has been recognized since antiquity, with descriptions of chronic bloody diarrhea dating back to Hippocrates. The modern understanding of IBD emerged in the early 20th century when Sir Samuel Wilks described ulcerative colitis as a distinct entity in 1859, and Burrill B. Crohn characterized regional ileitis in 1932. The NOD2/CARD15 gene, identified in 2001, was the first confirmed susceptibility gene for Crohn's disease.
Key Research Papers
- Ng SC, Shi HY, Hamidi N, et al. Worldwide incidence and prevalence of inflammatory bowel disease in the 21st century: a systematic review. The Lancet. 2017;390(10114):2769-2778.
- Jostins L, Ripke S, Weersma RK, et al. Host-microbe interactions have shaped the genetic architecture of inflammatory bowel disease. Nature. 2012;491(7422):119-124.
- Abraham C, Cho JH. Inflammatory bowel disease. N Engl J Med. 2009;361(21):2066-2078.
- Hugot JP, Chamaillard M, Zouali H, et al. Association of NOD2 leucine-rich repeat variants with susceptibility to Crohn's disease. Nature. 2001;411(6837):599-603.
- de Souza HSP, Fiocchi C, Iliopoulos D. The IBD interactome: an integrated view of aetiology, pathogenesis and therapy. Nat Rev Gastroenterol Hepatol. 2017;14(12):739-749.
- Sandborn WJ, Feagan BG, Rutgeerts P, et al. Vedolizumab as induction and maintenance therapy for Crohn's disease and ulcerative colitis. N Engl J Med. 2013;369(8):711-721.
- Feagan BG, Sandborn WJ, Gasink C, et al. Ustekinumab as induction and maintenance therapy for Crohn's disease. N Engl J Med. 2016;375(20):1946-1960.
- Gomollon F, Dignass A, Annese V, et al. 3rd European evidence-based consensus on the diagnosis and management of Crohn's disease (ECCO). J Crohns Colitis. 2017;11(1):3-25.
- Rubin DT, Ananthakrishnan AN, Siegel CA, et al. ACG clinical guideline: ulcerative colitis in adults. Am J Gastroenterol. 2019;114(3):384-413.
- Kaplan GG. The global burden of IBD: from 2015 to 2025. Nat Rev Gastroenterol Hepatol. 2015;12(12):720-727.
- Ananthakrishnan AN, Bernstein CN, Iliopoulos D, et al. Environmental triggers in IBD: a review of progress and evidence. Nat Rev Gastroenterol Hepatol. 2018;15(1):39-49.
- Ordas I, Eckmann L, Talamini M, Baumgart DC, Sandborn WJ. Ulcerative colitis. The Lancet. 2012;380(9853):1606-1619.
Research Papers
Curated PubMed topic searches of peer-reviewed literature on Inflammatory Bowel Disease (IBD). Each link opens a live PubMed query so you always see the most current studies.
- PubMed: IBD epidemiology
- PubMed: Biologic therapy in IBD
- PubMed: Microbiome dysbiosis in IBD
- PubMed: Vedolizumab in IBD
- PubMed: Ustekinumab in IBD
- PubMed: Surgical outcomes in IBD
- PubMed: CRC surveillance in IBD
- PubMed: Fecal calprotectin
- PubMed: Diet and nutrition in IBD
- PubMed: Pediatric IBD management
- PubMed: Extraintestinal manifestations
- PubMed: JAK inhibitors in IBD
Connections
- Gastroenterology
- Crohn's vs Ulcerative Colitis: Key Differences
- Diagnostic Workup: Calprotectin, Colonoscopy, MRE
- Biologics: TNF, IL-23, and Integrin Inhibitors
- JAK Inhibitors and S1P Modulators
- Diet for IBD: SCD and Mediterranean
- IBD Surgery Decisions
- Extraintestinal Manifestations: Joints, Skin, Eyes
- IBD Fatigue, Anemia, and Nutrient Deficiencies
- Pregnancy and IBD: Fertility, Medications, Outcomes
- Crohn's Disease
- Ulcerative Colitis
- SIBO
- Celiac Disease
- Irritable Bowel Syndrome
- Ankylosing Spondylitis
- Gut-Brain Axis
- Elimination Diet
- Ultra-Processed Foods
- Colorectal Cancer
- Hemorrhoids