IMO: Intestinal Methanogen Overgrowth & Constipation
If your breath test came back with high methane, or if you've been told you have "methane SIBO" and the antibiotics and low-FODMAP diet that worked for everyone else barely touched your bloating and constipation — you probably have IMO: Intestinal Methanogen Overgrowth. IMO is a different animal from the classic small intestinal bacterial overgrowth (SIBO) story most people learn first. The bugs are different (they aren't even bacteria), the symptoms lean heavily toward constipation rather than diarrhea, the treatment is harder, and the relapse rate is higher. This page is the plain-language patient guide to what IMO actually is, why it got renamed in 2020, how it's diagnosed, and what really works to knock it down and keep it down.
Interactive Visualization The Gut Barrier & Your Microbiome Watch fibre become butyrate and butyrate tighten the gut wall — then starve the microbes and see them eat your mucus layer instead. Launch →Table of Contents
- What IMO Is (and Why It Was Renamed)
- How Methane Causes Constipation
- Symptoms: The Methane Pattern
- Diagnosis: Breath Testing and the 10 ppm Rule
- Antibiotic Treatment: Why Rifaximin Alone Isn't Enough
- Herbal Antimicrobials for Methane
- Diet: Low-FODMAP Plus Low-Fermentation
- Prokinetics and Preventing Relapse
- Lovastatin and the Future of Methane-Specific Therapy
- Key Research Papers
- Connections
- Featured Videos
What IMO Is (and Why It Was Renamed)
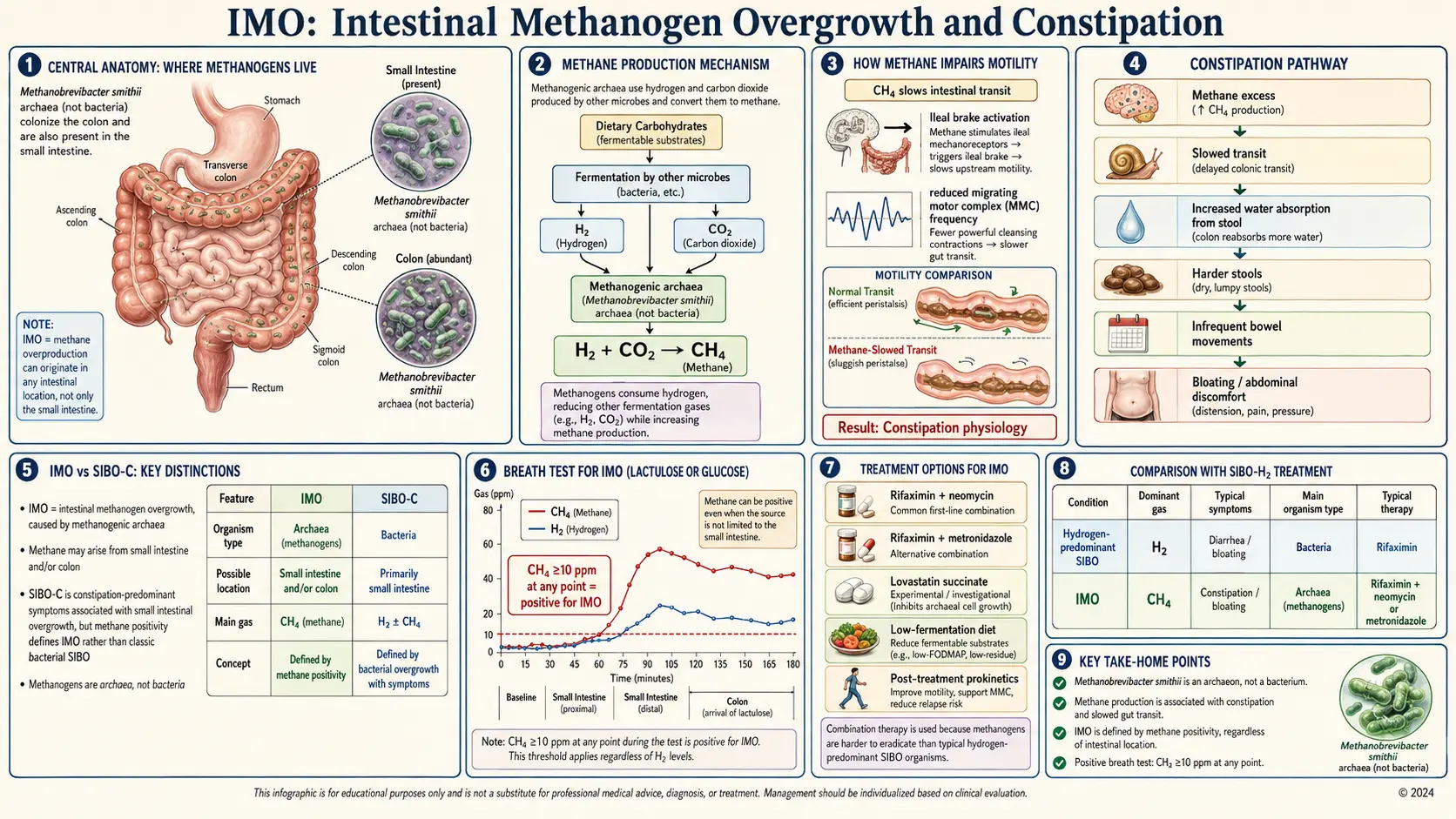
For years, clinicians and patients used the term "methane SIBO" to describe people with high breath methane and constipation. In 2020, a consensus of SIBO researchers formally proposed renaming the syndrome Intestinal Methanogen Overgrowth (IMO). Three facts drove the change:
- Methanogens aren't bacteria. They belong to the domain Archaea — a completely separate branch of life, more ancient than bacteria and biochemically distinct. Calling it "bacterial overgrowth" was technically wrong.
- One species dominates. The overwhelming majority of human methane is produced by Methanobrevibacter smithii. A minority of patients also carry Methanosphaera stadtmanae.
- It isn't limited to the small bowel. Methanogens colonize the entire GI tract — small intestine, cecum, and colon. That's why a breath sample taken at any time point can be informative, and why "small intestinal" in the old name was misleading.
The new name is more than a pedantic relabel. It forces clinicians to think about the colon too, to use different antimicrobials, and to understand why the classic SIBO rifaximin protocol so often disappoints methane patients.
How Methane Causes Constipation
Methane isn't just a marker — it's mechanistically constipating. Animal and human studies show that when methane is infused into the gut, transit slows measurably. Two effects stand out:
- Reduced small-bowel contractility. Methane appears to blunt the rhythmic contractions (the migrating motor complex and post-meal peristalsis) that sweep food and microbes downstream. Food lingers. Bloating builds.
- Slower colonic transit. Methane also slows movement through the colon, hardening stools and stretching out the time between bowel movements.
Higher breath methane levels correlate with more severe constipation, more bloating, and — in several studies — higher body weight and BMI. The weight association is still being untangled; one theory is that methanogens help host bacteria extract more calories from food by removing hydrogen, which unblocks further fermentation. Practically, this explains a recurring patient story: "I eat almost nothing and still gain weight, and I haven't had a normal bowel movement in years." That's the methane pattern.
Symptoms: The Methane Pattern
IMO symptoms overlap with hydrogen-predominant SIBO and IBS but skew in predictable directions:
- Constipation — hard stools, fewer than three bowel movements per week, incomplete evacuation, straining. This is the headline feature.
- Bloating — often worse as the day goes on, with a visibly distended abdomen by evening.
- Excessive belching or gas that doesn't smell particularly bad (methane itself is odorless).
- Weight gain or resistance to weight loss despite calorie control.
- Brain fog, fatigue, mild nausea — nonspecific but common.
- Overlap with IBS-C (constipation-predominant IBS) — many people labeled IBS-C test positive for IMO. See the Rome IV subtypes article.
If your primary complaint is diarrhea, you likely have hydrogen or hydrogen-sulfide SIBO instead. See the three-gas comparison.
Diagnosis: Breath Testing and the 10 ppm Rule
IMO is diagnosed with a lactulose or glucose breath test. You drink a sugar solution, then exhale into collection tubes every 15–20 minutes for three hours. The lab measures hydrogen, methane, and (on newer trio-smart devices) hydrogen sulfide in parts per million (ppm).
The 2017 North American Consensus set the criterion for IMO:
- Methane ≥ 10 ppm at any time point during the test = positive for IMO.
That's a key difference from hydrogen SIBO, which requires a rise of at least 20 ppm above baseline within 90 minutes. For methane, even a flat elevated baseline counts — because methanogens colonize the whole GI tract, they can pump out methane continuously without needing a fermentation spike.
Practical tips:
- A 3-hour collection is standard; shorter tests miss late-rising methane.
- Follow the 24-hour prep diet (plain protein, white rice, broth) and a 12-hour overnight fast.
- Avoid antibiotics for 4 weeks, probiotics for 2 weeks, and laxatives/prokinetics for a week before the test.
- Lactulose is preferred over glucose for IMO because it reaches the colon, where many methanogens live.
See the full Breath Test Guide for prep details, cost, and how to interpret your graph.
Antibiotic Treatment: Why Rifaximin Alone Isn't Enough
Here's where IMO patients get frustrated. Rifaximin monotherapy — the gold standard for hydrogen SIBO — is often disappointing against methane. Methanogens live partly in the colon, have thick archaeal cell walls, and simply aren't knocked out by rifaximin alone in many people. You need a second drug.
The three evidence-based regimens:
- Rifaximin 550 mg three times daily + Neomycin 500 mg twice daily × 14 days. This is the classic dual regimen. Pimentel's 2014 trial showed that the combination was significantly more effective than rifaximin alone for methane-predominant patients, with better symptom relief and methane reduction. Neomycin is a non-absorbed aminoglycoside that reaches the colon.
- Rifaximin 550 mg three times daily + Metronidazole 250 mg three times daily × 14 days. A common alternative when neomycin isn't available, is poorly tolerated, or insurance refuses to cover it. Metronidazole is cheap and widely available but causes nausea, a metallic taste, and must not be combined with alcohol.
- Rifaximin 550 mg three times daily × 14 days alone. Sometimes tried first in mild cases or when cost is prohibitive, but expect a lower response rate for methane.
Cost reality check. Rifaximin is expensive (often $1,500–$2,000 for a 14-day course without insurance) but Xifaxan has manufacturer copay cards that can drop it to $0–$50 for commercially insured patients. Neomycin and metronidazole are generic and cheap. Ask your pharmacist to check both the Salix/Bausch copay card for Xifaxan and GoodRx pricing.
For the full rifaximin protocol — including timing, food interactions, and what to do during treatment — see the Rifaximin Protocols page.
Herbal Antimicrobials for Methane
Herbal combinations are a legitimate alternative for patients who can't access or tolerate prescription antibiotics, or who prefer a natural-first approach. A 2014 Johns Hopkins trial found herbal antimicrobials roughly equivalent to rifaximin for general SIBO response. For methane specifically, the evidence is weaker but the three agents with the most support are:
- Allicin (stabilized garlic extract) — the single most-cited herbal agent for methane. Allicin appears to inhibit methanogen enzymes directly. Typical dose: Allimax Pro 450 mg, 2 capsules three times daily, for 4 weeks. Take on an empty stomach.
- Oregano oil (emulsified or enteric-coated) — broad-spectrum antimicrobial. Typical dose: 100–200 mg emulsified oregano, three times daily, for 4 weeks.
- Berberine — from goldenseal, Oregon grape, or barberry. Also helps blood sugar and motility in some patients. Typical dose: 400–500 mg three times daily, for 4 weeks.
Most protocols combine two or three of these and run them for 4–8 weeks (longer than antibiotics). Expect a 2–3 week period of Herxheimer-type symptoms (worse bloating, headache, fatigue) as methanogens die off. For the detailed herbal protocols — brand names, dosing schedules, and how to stack agents — see the Herbal Antimicrobials page.
Diet: Low-FODMAP Plus Low-Fermentation
A standard low-FODMAP diet helps IMO but often isn't enough on its own. Methanogens feed on the hydrogen produced when other microbes ferment carbohydrates — so reducing all fermentable substrate, not just high-FODMAP ones, tends to work better. The practical combination most SIBO dietitians use:
- Low-FODMAP as the backbone — eliminates the high-fermentation fruits, lactose, wheat, garlic, onion, legumes, and sugar alcohols.
- Low-fermentation layer — also limits resistant starch, cold potatoes, underripe bananas, and excess fiber during the treatment phase.
- Adequate fat and protein — these don't feed methanogens, so fish, eggs, olive oil, and lean meat become your nutritional anchor.
- Mind the gap between meals. Eat three distinct meals with 4–5 hours between them. Constant grazing prevents the migrating motor complex from firing, which is the #1 reason SIBO/IMO relapses.
An elemental diet (2–3 weeks of a predigested amino-acid formula) is the nuclear option when antibiotics and herbals fail — trials show 80%+ normalization of breath tests. It's tough to do and expensive, but it works.
Diet is a treatment-phase tool, not a forever sentence. Long term, starving your microbiome of all fiber makes things worse. The goal is to reintroduce foods methodically once the overgrowth is cleared.
Prokinetics and Preventing Relapse
This is where IMO patients win or lose. Without a prokinetic to keep the migrating motor complex firing at night, relapse rates run 40–60% within a year. The evidence-based options:
- Prucalopride (Motegrity) 1–2 mg at bedtime. A 5-HT4 agonist, specifically approved for chronic idiopathic constipation and the best-tolerated prokinetic for IMO. Insurance is the main obstacle — usually requires prior authorization documenting a trial of laxatives first.
- Low-dose erythromycin 50 mg at bedtime. An old antibiotic used at sub-antimicrobial doses as a motilin receptor agonist. Cheap, generic, but can cause tachyphylaxis (loss of effect) after a few months.
- Tegaserod — back on the US market in some formulations; effective but has cardiovascular warnings.
- Natural prokinetics — ginger (Iberogast, or 1000 mg ginger extract + 20 mg artichoke leaf at bedtime, as in MotilPro/Motility Activator). Gentler but often enough for mild cases.
Plan on staying on a prokinetic for at least 3–6 months after clearing the overgrowth, longer if you have an underlying motility disorder. See the Prokinetics and Relapse Prevention page for full dosing, side effects, and how to wean off. And address the root cause — adhesions, hypothyroidism, post-infectious IBS, Ehlers-Danlos, diabetic gastroparesis — or you'll just keep recurring.
Lovastatin and the Future of Methane-Specific Therapy
One of the most interesting stories in the IMO field is lovastatin. Beyond lowering cholesterol, lovastatin's lactone form inhibits an enzyme (HMG-CoA reductase) that methanogens also use to build their cell membranes. A specially formulated delayed-release lovastatin lactone called SYN-010 was developed by Synthetic Biologics to deliver the drug intact to the intestine, targeting methanogens without significantly lowering blood cholesterol.
Early phase II trials (Gottlieb 2016 and subsequent studies) showed promising methane reduction and symptom improvement in IBS-C patients with elevated methane. SYN-010 is still investigational as of 2026 and is not FDA-approved.
Important caveat. Regular commercial lovastatin is not a substitute for SYN-010. It's absorbed in the upper GI tract and reaches the blood before it can act on colonic methanogens, bringing the usual statin side-effect profile (muscle pain, liver enzyme changes, rare rhabdomyolysis) without targeted action. Some naturopaths experiment with red yeast rice (which contains natural monacolin K, biochemically identical to lovastatin) but the same caveat applies, plus red yeast rice is unregulated and variable in potency. Don't self-prescribe statins for IMO — wait for SYN-010 or a confirmed clinical protocol.
Key Research Papers
Foundational and recent peer-reviewed publications on methanogen biology, intestinal methanogen overgrowth, and methane-associated constipation. Each citation links to the full text via DOI.
- Pimentel M, Saad RJ, Long MD, Rao SSC. ACG Clinical Guideline: Small Intestinal Bacterial Overgrowth. American Journal of Gastroenterology. 2020;115(2):165–178.
- Rezaie A, Buresi M, Lembo A, et al. Hydrogen and Methane-Based Breath Testing in Gastrointestinal Disorders: The North American Consensus. American Journal of Gastroenterology. 2017;112(5):775–784.
- Pimentel M, Lin HC, Enayati P, et al. Methane, a Gas Produced by Enteric Bacteria, Slows Intestinal Transit and Augments Small Intestinal Contractile Activity. American Journal of Physiology — Gastrointestinal and Liver Physiology. 2006;290(6):G1089–G1095.
- Triantafyllou K, Chang C, Pimentel M. Methanogens, Methane and Gastrointestinal Motility. Journal of Neurogastroenterology and Motility. 2014;20(1):31–40.
- Kunkel D, Basseri RJ, Makhani MD, Chong K, Chang C, Pimentel M. Methane on Breath Testing Is Associated with Constipation: A Systematic Review and Meta-Analysis. Digestive Diseases and Sciences. 2011;56(6):1612–1618.
- Rezaie A, Heitkemper M, Chey WD, Pimentel M. Patients in Whom Methane Is the Predominant Gas on Breath Testing Have Higher Levels of Constipation: Implications for the Diagnosis and Treatment of Constipation Predominant Bowel Disorders. American Journal of Gastroenterology. 2019;114(3):383–385.
- Pimentel M, Chow EJ, Lin HC. Eradication of Small Intestinal Bacterial Overgrowth Reduces Symptoms of Irritable Bowel Syndrome. American Journal of Gastroenterology. 2000;95(12):3503–3506.
- Low K, Hwang L, Hua J, Zhu A, Morales W, Pimentel M. A Combination of Rifaximin and Neomycin Is Most Effective in Treating Irritable Bowel Syndrome Patients with Methane on Lactulose Breath Test. Journal of Clinical Gastroenterology. 2010;44(8):547–550.
- Pimentel M, Chang C, Chua KS, et al. Antibiotic Treatment of Constipation-Predominant Irritable Bowel Syndrome. Digestive Diseases and Sciences. 2014;59(6):1278–1285.
- Gottlieb K, Wacher V, Sliman J, Pimentel M. Review Article: Inhibition of Methanogenic Archaea by Statins as a Targeted Management Strategy for Constipation and Related Disorders. Alimentary Pharmacology & Therapeutics. 2016;43(2):197–212.
- Chedid V, Dhalla S, Clarke JO, et al. Herbal Therapy Is Equivalent to Rifaximin for the Treatment of Small Intestinal Bacterial Overgrowth. Global Advances in Health and Medicine. 2014;3(3):16–24.
- Mathur R, Kim G, Morales W, et al. Intestinal Methanobrevibacter smithii but Not Total Bacteria Is Related to Diet-Induced Weight Gain in Rats. Obesity. 2013;21(4):748–754.
Live PubMed Searches
Live PubMed queries that update as new papers are indexed.
- PubMed: intestinal methanogen overgrowth
- PubMed: Methanobrevibacter smithii and constipation
- PubMed: methane breath test and constipation
- PubMed: rifaximin plus neomycin for methane SIBO
- PubMed: lovastatin, SYN-010, methanogen inhibition
- PubMed: allicin and methanogen archaea
- PubMed: prucalopride for chronic constipation
- PubMed: migrating motor complex and SIBO recurrence
- PubMed: methane, BMI, obesity-microbiome link
- PubMed: North American Consensus on breath testing
Connections
- Gastroenterology
- The Gut Barrier & Your Microbiome — interactive animation
- SIBO Overview
- Herbal Antimicrobials
- Prokinetics and Relapse Prevention
- Rifaximin Protocols
- Breath Test Guide
- Elemental Diet
- Low-FODMAP Diet
- Root Causes
- Hydrogen vs Methane vs Hydrogen Sulfide
- Irritable Bowel Syndrome
- Rome IV Subtypes
- Constipation
- Bloating
- Garlic
- Oregano
- Berberine
- Probiotics
- Thyroid Disorders