Bloating
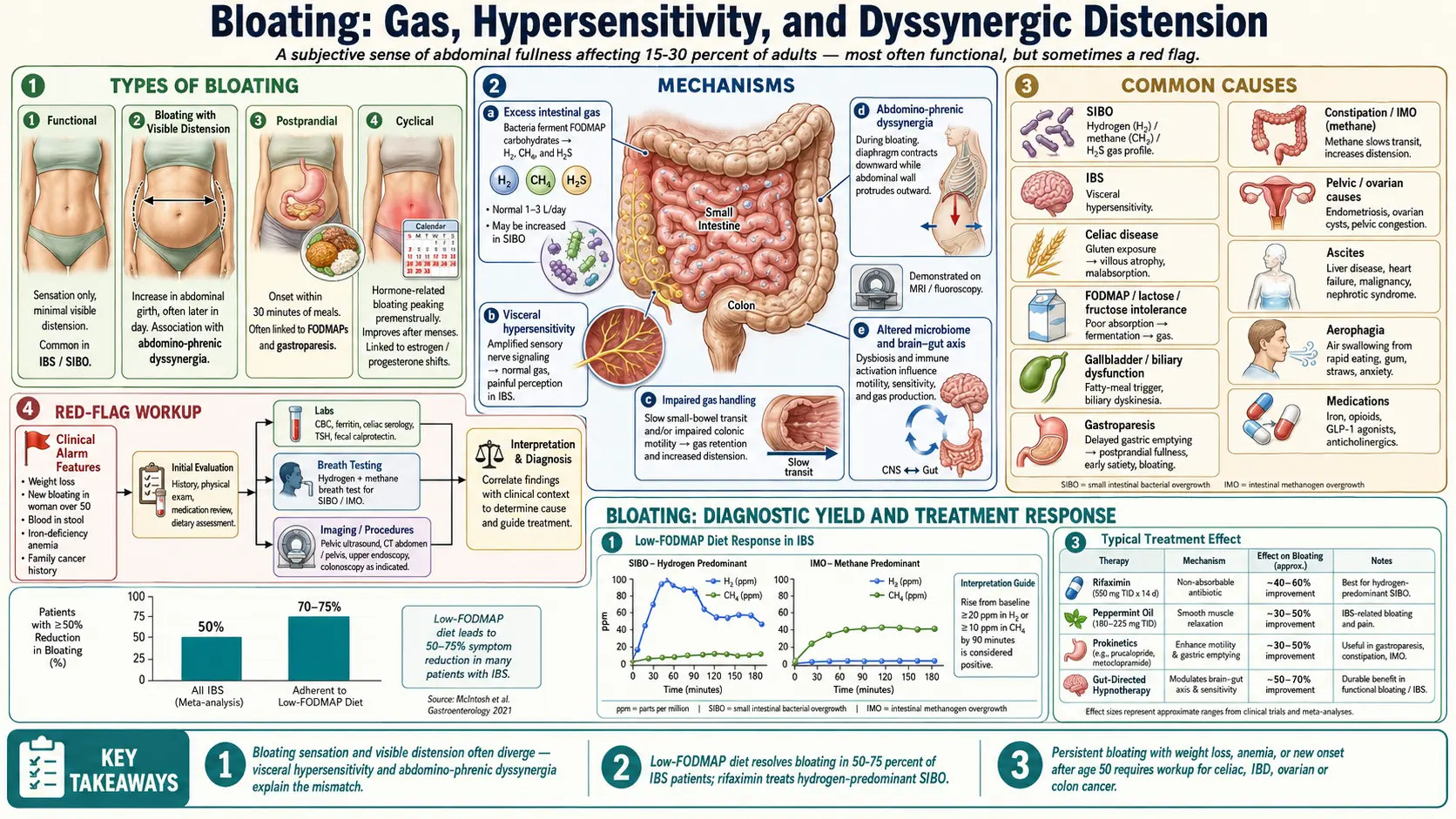
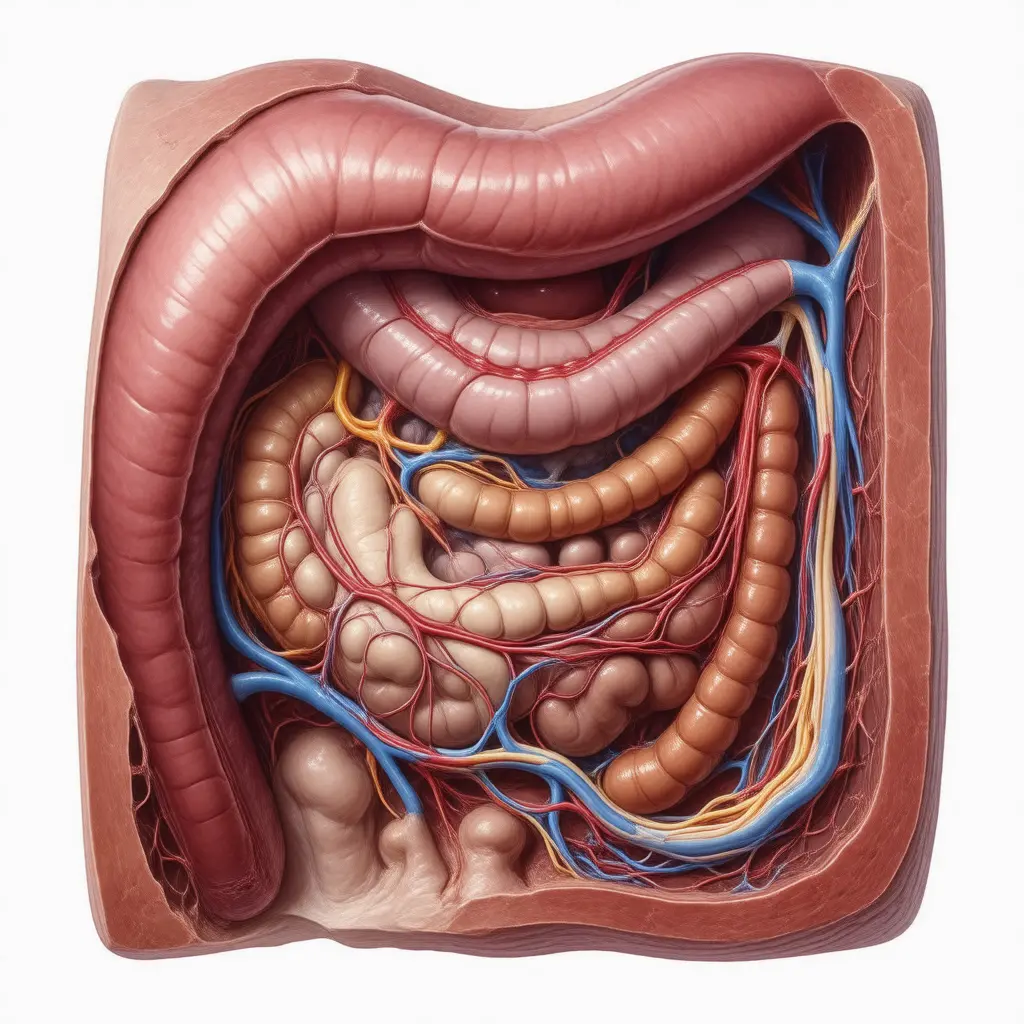
Table of Contents
- Overview
- Types of Bloating
- Common Causes
- Mechanisms
- Evaluation
- Management
- When to Seek Medical Care
- Connections
- References & Research
- Featured Videos
Overview
Bloating is the subjective sensation of abdominal fullness, pressure, or trapped gas. It is one of the most common gastrointestinal complaints, affecting an estimated 15–30 percent of adults at any given time, and is the leading reason patients seek care for digestive symptoms. Bloating may or may not be accompanied by visible abdominal distension — an actual measurable increase in abdominal girth. Most bloating is benign and tied to diet, motility, or visceral hypersensitivity, but persistent bloating with weight loss, anemia, or change in bowel habits warrants evaluation for malignancy, celiac disease, or chronic obstruction.
Types of Bloating
- Functional bloating — sensation of pressure or fullness without an identifiable structural cause. Common in IBS, functional dyspepsia, and SIBO.
- Bloating with distension — both the sensation and a visible increase in girth. Often involves abdomino-phrenic dyssynergia, where the diaphragm pushes down and the abdominal wall protrudes outward in response to even normal gas volumes.
- Postprandial bloating — develops within 30 minutes to a few hours of eating and resolves overnight. Typical of food intolerances (lactose, fructose, FODMAPs), gastroparesis, and gallbladder disease.
- Persistent or progressive bloating — present most days, gradually worsening, or accompanied by enlarging abdominal girth. Requires workup for ascites, ovarian pathology, malignancy, or chronic bowel obstruction.
- Cyclical bloating — tied to the menstrual cycle, peaking premenstrually. Driven by hormonal effects on bowel motility and fluid retention.
Common Causes
- Small intestinal bacterial overgrowth (SIBO) — bacteria normally confined to the colon ferment carbohydrates in the small intestine, producing hydrogen, methane, or hydrogen sulfide gas. The hallmark is bloating that worsens through the day and after meals.
- Irritable bowel syndrome (IBS) — the most common functional cause. Bloating in IBS reflects visceral hypersensitivity to normal gas volumes plus altered motility.
- Celiac disease — gluten-driven small-bowel inflammation impairs digestion of carbohydrates, causing fermentation and bloating along with diarrhea, weight loss, and nutrient deficiencies.
- Lactose, fructose, and FODMAP intolerance — undigested fermentable carbohydrates reach the colon and are fermented by bacteria, producing gas.
- Gallbladder disease and biliary dysfunction — impaired bile flow leaves fat poorly emulsified, leading to maldigestion, postprandial fullness, and bloating, particularly after fatty meals.
- Gastroparesis — delayed gastric emptying, often from diabetes or post-viral nerve injury, produces fullness, early satiety, and bloating after meals.
- Constipation — slow colonic transit allows more time for fermentation and gas accumulation. Common in methane-predominant SIBO (IMO) and hypothyroidism.
- Pelvic and gynecologic causes — ovarian cysts, fibroids, endometriosis, and ovarian cancer can present with bloating and an enlarging abdominal girth.
- Ascites — fluid accumulation in the peritoneal cavity from cirrhosis, heart failure, malignancy, or nephrotic syndrome.
- Aerophagia — air swallowing from chewing gum, carbonated drinks, smoking, or anxiety.
- Medications — iron supplements, opioids, calcium-channel blockers, GLP-1 agonists, and some antidepressants commonly cause bloating.
Mechanisms
Bloating arises from several overlapping mechanisms, and most patients have more than one operating at once:
- Excess intestinal gas — normal flora produce 1–3 liters of gas per day from fermentable carbohydrates. SIBO, FODMAP intolerance, and rapid transit can multiply this many times over.
- Visceral hypersensitivity — the gut perceives normal gas volumes as painful or distending. This is the dominant mechanism in IBS and explains why total measured gas volumes often look normal in patients who feel severely bloated.
- Abnormal gas handling — impaired ability to propel and expel gas. Patients may have normal amounts of gas but slow transit through the small bowel.
- Abdomino-phrenic dyssynergia — an abnormal motor reflex in which the diaphragm contracts downward and the anterior abdominal wall relaxes in response to gas, producing visible distension out of proportion to gas volume. Identified by MRI or fluoroscopy.
- Altered microbiome — both composition (which species dominate) and location (small bowel vs. colon) influence which substrates are fermented and which gases are produced.
- Brain-gut axis — stress and emotional arousal modulate motility, secretion, and pain perception, often amplifying bloating.
Evaluation
Initial workup is guided by the pattern (functional vs. progressive, postprandial vs. persistent) and any alarm features. A reasonable starting set includes:
- History and dietary review — timing, triggers, FODMAP exposure, alcohol, fiber load, recent antibiotics, weight change, bowel-habit change.
- Complete blood count, ferritin, comprehensive metabolic panel — screen for anemia, malnutrition, liver dysfunction.
- Celiac serology — tissue transglutaminase IgA with total IgA. Should be done while still eating gluten.
- TSH — rule out hypothyroidism as a constipation/bloating driver.
- Fecal calprotectin — differentiates inflammatory from functional causes.
- Hydrogen and methane breath testing — for SIBO, IMO, and lactose/fructose malabsorption. See the Breath Test Guide for prep, interpretation, and pitfalls.
- Stool studies — ova and parasites, Giardia antigen, fecal elastase (pancreatic insufficiency).
- Abdominal imaging — ultrasound or CT for ascites, mass, or biliary disease. Pelvic ultrasound for ovarian pathology in women.
- Upper endoscopy with biopsy — if celiac is suspected and serology is positive, or if symptoms include reflux, dysphagia, or anemia.
- Colonoscopy — in patients over 45, with iron deficiency, blood in stool, or unexplained weight loss.
Management
- Treat the underlying cause — rifaximin for hydrogen-predominant SIBO, gluten-free diet for celiac, levothyroxine for hypothyroidism, prokinetics for gastroparesis. See Rifaximin Protocols for SIBO dosing.
- Low-FODMAP diet — an elimination-and-reintroduction protocol that resolves bloating in 50–75 percent of IBS patients. Should be done with a registered dietitian to avoid unnecessary long-term restriction. See the Low-FODMAP Diet overview.
- Targeted food avoidance — lactose, fructose, sugar alcohols (sorbitol, mannitol), and excessive fiber are the most common triggers.
- Prokinetics — low-dose erythromycin, prucalopride, or metoclopramide can improve transit and reduce postprandial bloating; particularly important for SIBO relapse prevention. See Prokinetics & Relapse Prevention.
- Peppermint oil — enteric-coated peppermint oil reduces bloating and pain in IBS through smooth-muscle relaxation, supported by multiple meta-analyses.
- Probiotics — mixed evidence; some strains (Bifidobacterium infantis 35624) modestly reduce bloating in IBS, while others worsen it in SIBO. Discontinue if symptoms worsen.
- Digestive enzymes — lactase for lactose intolerance, alpha-galactosidase (Beano) for legume bloating, pancreatic enzymes for documented insufficiency.
- Diaphragmatic breathing and biofeedback — useful for abdomino-phrenic dyssynergia; teaches the diaphragm to relax upward rather than push down.
- Stress management — gut-directed hypnotherapy and cognitive-behavioral therapy reduce visceral hypersensitivity and have effect sizes comparable to pharmacotherapy in IBS.
- Movement — light walking after meals accelerates transit and reduces postprandial bloating.
When to Seek Medical Care
- Bloating accompanied by unintentional weight loss, especially in adults over 40.
- New-onset bloating in a woman over 50 (rule out ovarian cancer).
- Rapidly progressive abdominal distension or visibly enlarging girth.
- Blood in stool, black or tarry stool, or persistent change in bowel habits.
- Severe persistent abdominal pain, especially with fever or vomiting.
- Iron-deficiency anemia, low albumin, or other signs of malabsorption.
- Bloating with shortness of breath, leg swelling, or known liver or heart disease (consider ascites).
- Family history of colon, ovarian, or pancreatic cancer with new persistent bloating.
Connections
- SIBO
- Irritable Bowel Syndrome
- IMO & Methane Constipation
- Celiac Disease
- Gallbladder Disease
- SIBO Breath Test Guide
- Rifaximin Protocols
- Low-FODMAP Diet
- Thyroid Disorders
- Gut Healing
- Abdominal Pain
- Prokinetics & Relapse Prevention
- GERD
- Nausea and Vomiting
- SIBO Root Causes
- Pancreatitis
- Probiotics
- Elimination Diet
- Ovarian Cancer
References & Research
Historical Background
Bloating was long dismissed as a vague functional complaint until the late twentieth century, when manometric studies, breath testing, and abdominal imaging made it possible to distinguish gas accumulation from visceral hypersensitivity from abnormal abdominal-wall mechanics. The rediscovery of small intestinal bacterial overgrowth in the 1990s and the formalization of low-FODMAP dietary therapy by Monash University in the 2000s gave clinicians their first reproducible, evidence-based interventions for chronic bloating.
Key Research Papers
- Lacy BE, Cangemi D, Vazquez-Roque M. Management of chronic abdominal distension and bloating. Clinical Gastroenterology and Hepatology. 2021;19(2):219-231.
- Halmos EP, Power VA, Shepherd SJ, Gibson PR, Muir JG. A diet low in FODMAPs reduces symptoms of irritable bowel syndrome. Gastroenterology. 2014;146(1):67-75.
- Pimentel M, Lembo A, Chey WD, et al. Rifaximin therapy for patients with irritable bowel syndrome without constipation. New England Journal of Medicine. 2011;364(1):22-32.
- Villoria A, Azpiroz F, Burri E, Cisternas D, Soldevilla A, Malagelada JR. Abdomino-phrenic dyssynergia in patients with abdominal bloating and distension. American Journal of Gastroenterology. 2011;106(5):815-819.
- Rezaie A, Buresi M, Lembo A, et al. Hydrogen and methane-based breath testing in gastrointestinal disorders: the North American consensus. American Journal of Gastroenterology. 2017;112(5):775-784.
- Chey WD, Kurlander J, Eswaran S. Irritable bowel syndrome: a clinical review. JAMA. 2015;313(9):949-958.
- Pimentel M, Saad RJ, Long MD, Rao SSC. ACG clinical guideline: small intestinal bacterial overgrowth. American Journal of Gastroenterology. 2020;115(2):165-178.
- Mearin F, Lacy BE, Chang L, et al. Bowel disorders. Gastroenterology. 2016;150(6):1393-1407. (Rome IV criteria)
- Khanna R, MacDonald JK, Levesque BG. Peppermint oil for the treatment of irritable bowel syndrome: a systematic review and meta-analysis. Alimentary Pharmacology & Therapeutics. 2014;40(7):685-694.
- Ford AC, Sperber AD, Corsetti M, Camilleri M. Irritable bowel syndrome. The Lancet. 2020;396(10263):1675-1688.
PubMed Topic Searches
- Abdominal bloating pathophysiology
- SIBO — small intestinal bacterial overgrowth
- Low-FODMAP diet and bloating
- Visceral hypersensitivity in IBS
- Abdomino-phrenic dyssynergia
- Methane (IMO) and constipation