SIBO Breath Test Guide
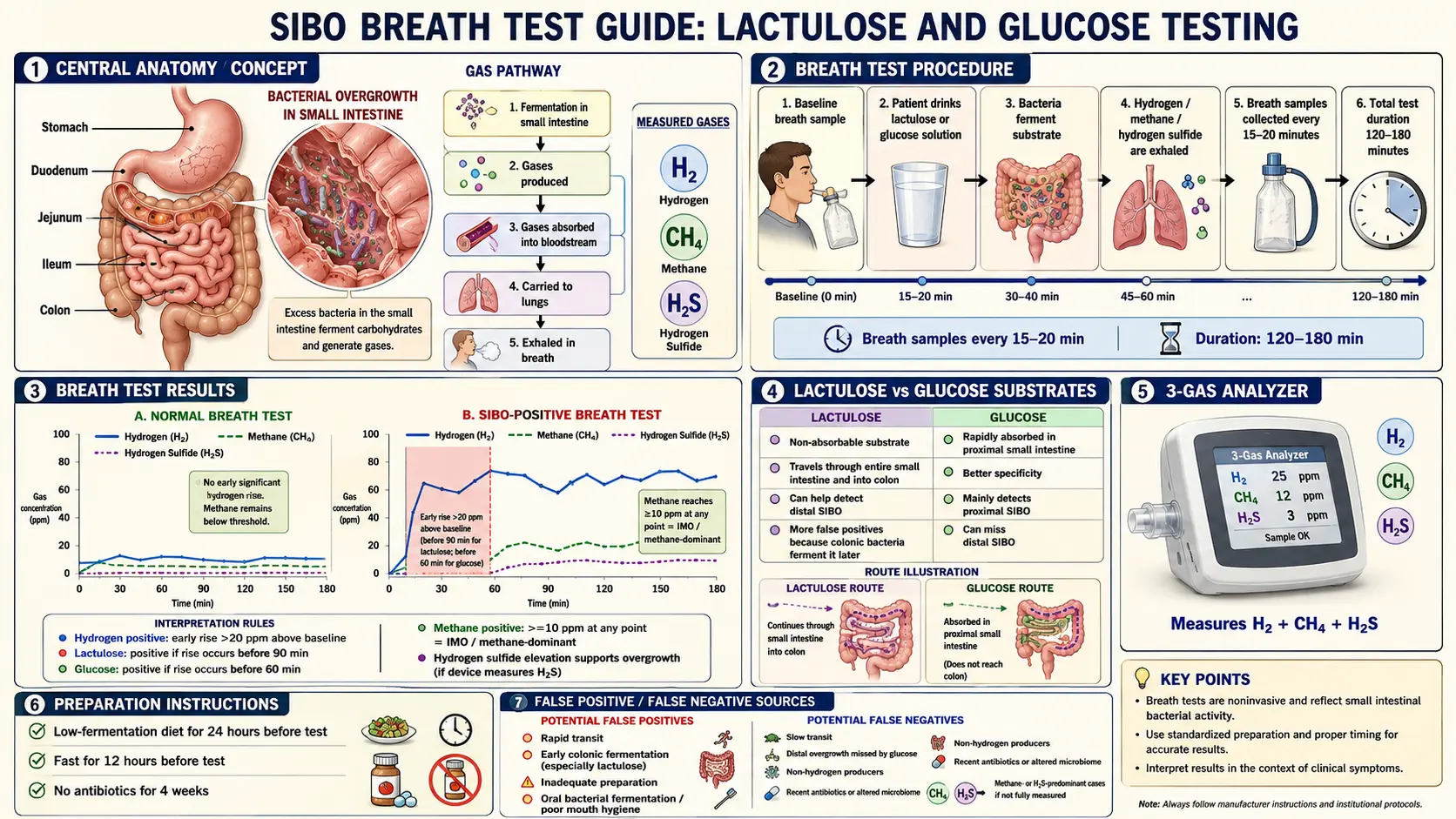
Table of Contents
- What a Breath Test Is Actually Measuring
- The Three Tests: Lactulose, Glucose, Trio-Smart
- The Prep Matters More Than You Think
- Reading Your Results
- Why False Negatives Are So Common
- Where to Get Tested
- What to Do If Your Test Is Positive
- What to Do If Your Test Is Negative But You Still Have Symptoms
- Key Research Papers
- Connections
- Featured Videos
1. What a Breath Test Is Actually Measuring
The strange thing about a SIBO breath test is that it doesn’t actually look at your gut. It looks at your breath. Here’s the full loop, in plain language:
- You drink a sugary solution (lactulose, glucose, or sometimes fructose).
- That sugar travels down to your small intestine.
- If there are too many bacteria living up there, they grab the sugar and ferment it — the same chemistry that makes beer or sourdough.
- Fermentation produces hydrogen (H2), methane (CH4), and/or hydrogen sulfide (H2S) as waste gases.
- Those gases dissolve into your bloodstream through the thin gut wall, ride to your lungs, and cross into the air sacs.
- You exhale them. A small machine or collection bag measures the concentration in parts per million (ppm) every 15–20 minutes for two to three hours.
Human cells cannot make hydrogen, methane, or hydrogen sulfide on their own. So any of these gases in your breath must have come from microbes. The question the test answers is not “are there microbes?” — there always are — but where and how many. Gas that appears early (within the first 90–120 minutes) points to fermentation in the small intestine, which is abnormal. Gas that appears later is normal colonic fermentation.
This is important to understand before you walk in the door, because the test’s whole logic — the timing, the prep, the thresholds — is built around catching that early rise. Anything you do that disrupts the timing can produce a false negative or a false positive.
2. The Three Tests: Lactulose, Glucose, Trio-Smart
There are three breath tests in clinical use today. They measure different things, reach different parts of the gut, and have very different sensitivity and specificity profiles. Ask your doctor which one is being ordered — most will default to whatever their lab offers, which may not be the best fit for your case.
| Feature | Lactulose (LBT) | Glucose (GBT) | Trio-Smart |
|---|---|---|---|
| Substrate dose | 10 g lactulose | 50–75 g glucose | 10 g lactulose (usually) |
| Gases measured | H2, CH4 | H2, CH4 | H2, CH4, H2S |
| Positive H2 threshold | ≥20 ppm rise from baseline within 90 min | ≥12–20 ppm rise within 120 min | Same as lactulose |
| Positive CH4 threshold | ≥10 ppm at any single timepoint | ≥10 ppm at any single timepoint | ≥10 ppm at any single timepoint |
| Positive H2S threshold | Not measured | Not measured | ≥3 ppm |
| Sensitivity | 52–68% | 20–93% | Highest of the three |
| Specificity | 44–86% | 30–86% | Comparable to lactulose |
| Reach | Entire small bowel (distal reach) | Proximal only | Entire small bowel |
Lactulose Breath Test (LBT)
Lactulose is a synthetic sugar that humans cannot absorb at all. Every bit of it travels the full length of the small intestine and into the colon. That makes it excellent for catching distal overgrowth — bacteria living in the last part of the small bowel near the ileocecal valve. The catch is that lactulose will always ferment eventually (in the colon, around 90–120 minutes), so the 90-minute rule matters: a hydrogen rise before 90 minutes indicates small-bowel fermentation; after that, you’re probably just watching normal colonic activity.
Glucose Breath Test (GBT)
Glucose is absorbed completely in the first two to three feet of small intestine. If bacteria ferment it before your body can absorb it, there’s clearly overgrowth — but only in the proximal small bowel. A glucose test is more specific (fewer false positives) but less sensitive (more false negatives) because it simply cannot reach bacteria living further down. If your overgrowth is in the distal ileum, a glucose test will miss it entirely.
Trio-Smart
Trio-smart is the newest option and, for most patients, the one worth asking for. It measures all three fermentation gases simultaneously on the same breath sample. Before trio-smart existed, roughly 15–20% of symptomatic SIBO patients got a “flat-line” result — neither hydrogen nor methane elevated — and were told they didn’t have SIBO. Many of those people actually had hydrogen sulfide overgrowth (driven by Desulfovibrio and Fusobacterium species), which was invisible to the old machines. Trio-smart catches that missing slice.
3. The Prep Matters More Than You Think
This is where most people unknowingly wreck their test. The breath test is looking for gas produced by bacteria in real time, so anything that leaves residual fermentable food in your gut, or kills off the bacteria before the test, or adds confounding gas from your mouth, will distort the result. Here are the rules, and why each one exists:
- 4-week antibiotic washout. Any antibiotic within the last month — even a dental course or a Z-Pak — will knock down the overgrowth temporarily and produce a falsely low gas output. Rifaximin, doxycycline, and amoxicillin are the usual culprits. Bismuth subsalicylate (Pepto-Bismol) counts too and should be stopped for 2 weeks.
- 1-week pause on prokinetics and laxatives. Anything that speeds transit — prucalopride, low-dose erythromycin, magnesium citrate, senna, MiraLAX, linaclotide — flushes the substrate through the small bowel before the bacteria can ferment it. You get a flat curve that looks normal but isn’t.
- 24-hour prep diet. The day before the test, eat only: plain white rice, plain baked or boiled chicken or turkey (no marinade, no spices beyond salt), eggs, clear beef or chicken broth, and water, black coffee, or weak black tea. No vegetables, no fruit, no dairy, no whole grains, no fiber, no sweeteners, no gum. Anything fermentable left in your gut overnight will still be feeding bacteria when you arrive, raising your baseline hydrogen and masking the real rise.
- 12-hour fast before the test. Nothing but plain water after dinner the night before. No coffee the morning of.
- No mouthwash or fluoride toothpaste the morning of. Your mouth contains billions of bacteria that can ferment the lactulose the moment you swallow it, producing an early hydrogen spike that never came from your gut. Brush with plain water or a baking-soda paste, and skip mouthwash entirely.
- No smoking and no vigorous exercise during the test. Smoking contains hydrogen directly and inflates every sample. Exercise changes your breathing rate and alters the ppm reading. Read, sit, scroll — don’t walk laps.
- No sleeping during the test. Hypoventilation lowers gas concentrations and flattens the curve.
If any one of these rules gets broken, the honest move is to reschedule. A botched $250 test that tells you the wrong answer is far more expensive than a second trip to the lab.
4. Reading Your Results
When the lab sends your report, you’ll see a grid of numbers — ppm readings at 0, 20, 40, 60, 80, 100, 120, 140, 160, 180 minutes — and usually a graph of two or three curves. Here is what to look for.
Hydrogen (H2) — requires a RISE
Hydrogen is diagnostic only in terms of change from baseline. Your baseline might be 5 ppm or 15 ppm; what matters is whether it climbs ≥20 ppm above that baseline within the first 90 minutes of a lactulose test (or within 120 minutes of a glucose test). A steady high reading that never rises isn’t SIBO — it probably means you didn’t fast properly.
Methane (CH4) — diagnostic at ANY single value
Methane plays by different rules. A methane level of ≥10 ppm at any single timepoint — including baseline — is diagnostic of intestinal methanogen overgrowth (IMO). It doesn’t need to rise. This is because methanogens (Methanobrevibacter smithii) produce methane steadily rather than in a post-substrate burst, and high methane correlates strongly with constipation.
Hydrogen Sulfide (H2S) — trio-smart only
H2S ≥3 ppm at any timepoint is positive. H2S-dominant patients often show a pattern of suppressed hydrogen (the sulfate-reducing bacteria consume H2 to make H2S), so a very flat hydrogen curve combined with elevated H2S is classic.
The “Double Peak” Curve
A classic SIBO lactulose curve has two peaks: an early rise around 30–80 minutes (the small-bowel bacteria fermenting), followed by a dip, then a second much larger rise after 100–120 minutes (the lactulose finally hitting the colon). A single late peak is normal. A single early peak is SIBO. A double peak is SIBO plus a healthy colonic microbiome doing its job afterward.
5. Why False Negatives Are So Common
If you have textbook SIBO symptoms — the bloating that builds through the day, the sulfur burps, the alternating constipation and diarrhea — but your breath test came back negative, you are in enormous company. False-negative rates for lactulose and glucose breath tests commonly run 30–50%. Here is why:
- Bad prep. By far the most common cause. A prep-diet cheat, a recent antibiotic, an unflagged prokinetic, or mouthwash the morning of the test.
- Hydrogen sulfide overgrowth. If the lab used a two-gas machine (H2 and CH4 only), H2S producers are invisible. These patients often have suppressed hydrogen because the sulfate-reducing bacteria eat it. A trio-smart retest fixes this. See the Hydrogen vs. Methane vs. Hydrogen Sulfide article for the full breakdown.
- Oral bacteria contamination. Poor dental hygiene can make the mouth ferment lactulose faster than the gut, producing an irrelevant early spike that obscures the real pattern.
- Fast transit flushing the substrate. If the substrate sweeps through the small bowel too quickly (common in hyperthyroidism or after laxative use), bacteria don’t have time to ferment it.
- Distal-only overgrowth missed by glucose. Glucose is absorbed in the first few feet. Overgrowth in the distal ileum produces no glucose response but is caught by lactulose.
- Recent antibiotics in the last 4 weeks. Including dental prophylaxis, UTI courses, and courses taken for an unrelated infection.
- Intermittent overgrowth. Bacterial populations fluctuate. A test caught on a “low day” can miss the condition.
- Hydrogen non-producers. A small percentage of people have gut flora that produce almost no hydrogen under any circumstance. Without the CH4 or H2S data, they look normal.
6. Where to Get Tested
There are two paths: in-office testing at a GI clinic, or an at-home kit. Both require a physician’s order in most cases.
- In-office testing. You sit in a chair at the GI clinic for 2–3 hours blowing into a tube every 15–20 minutes. The upside is that staff handle the timing and the samples are analyzed immediately. The downside is cost and the logistical hassle.
- At-home kits. The two major providers in the US are Commonwealth Diagnostics International (which makes trio-smart) and Aerodiagnostics. A kit arrives with pre-labeled collection bags, the lactulose substrate, detailed prep instructions, and a prepaid return shipping envelope. You do the test at your kitchen table. Results typically arrive in 5–10 business days via your ordering physician’s portal.
Cost. Cash-pay ranges from roughly $150 for a basic two-gas lactulose test to $350 for trio-smart. Insurance coverage is inconsistent — Medicare covers breath testing with appropriate ICD-10 codes (K90.9, K59.9), many commercial plans cover it with prior authorization, and some exclude it as “investigational.” Call your insurer before ordering.
7. What to Do If Your Test Is Positive
A positive breath test is a starting line, not a finish line. It tells you bacteria are fermenting where they shouldn’t be; it does not tell you why. Treatment typically follows a three-track approach:
- Eradicate the overgrowth. This is where rifaximin (for hydrogen-dominant), rifaximin + neomycin (for methane-dominant), or herbal antimicrobials come in. The Chedid 2014 study showed herbs are statistically equivalent to rifaximin, so neither choice is obviously better — it often comes down to cost, access, and tolerance.
- Manage symptoms during treatment. A low-FODMAP diet or the elemental diet for more aggressive cases.
- Prevent relapse. This is the step most doctors skip and the reason SIBO comes back in 44–46% of people. See Prokinetics & Relapse Prevention and the work on root causes.
Retest 3–4 weeks after finishing antimicrobials to confirm eradication. If gases have normalized but symptoms persist, you’re likely dealing with residual visceral hypersensitivity or a root cause that hasn’t been addressed.
8. What to Do If Your Test Is Negative But You Still Have Symptoms
Don’t walk away yet. A negative two-gas test in a patient with classic SIBO symptoms is, more often than not, a false negative. Here is the practical order of next steps:
- Trio-smart retest. If your first test measured only H2 and CH4, insist on a trio-smart retest that includes H2S. This alone catches a large chunk of previously “negative” patients.
- Audit your prep. If you broke any of the rules — recent antibiotic, prokinetic still on board, a salad the night before, mouthwash that morning — retest after a clean run.
- Anti-vinculin and anti-CdtB antibody testing. The ibs-smart blood test identifies post-infectious IBS with autoimmune damage to the interstitial cells of Cajal. Many SIBO patients develop the condition after a stomach flu (Campylobacter, Salmonella, Shigella, or E. coli), and these antibodies are the fingerprint. See Root Causes.
- Empirical treatment trial. Some physicians will prescribe a two-week rifaximin or herbal antimicrobial course based on symptoms alone. If you respond, that’s diagnostically informative. If you don’t, you’ve ruled out SIBO as the primary driver.
- Jejunal aspirate. The traditional gold standard, done via upper endoscopy. Invasive and expensive, but definitive — a bacterial count of ≥103 CFU/mL of colonic-type organisms confirms the diagnosis. Usually reserved for refractory cases or complicated patients (immunosuppressed, post-surgical).
- Investigate alternative diagnoses. Bile acid malabsorption, sucrase-isomaltase deficiency, pancreatic insufficiency, visceral hypersensitivity, and pelvic floor dysfunction can all mimic SIBO.
9. Key Research Papers
Foundational peer-reviewed literature on the diagnostic accuracy, methodology, and interpretation of breath testing for SIBO and intestinal methanogen overgrowth. Each citation links to the full text via DOI.
- Pimentel M, Saad RJ, Long MD, Rao SSC. ACG Clinical Guideline: Small Intestinal Bacterial Overgrowth. American Journal of Gastroenterology. 2020;115(2):165–178.
- Rezaie A, Buresi M, Lembo A, et al. Hydrogen and Methane-Based Breath Testing in Gastrointestinal Disorders: The North American Consensus. American Journal of Gastroenterology. 2017;112(5):775–784.
- Saad RJ, Chey WD. Breath Testing for Small Intestinal Bacterial Overgrowth: Maximizing Test Accuracy. Clinical Gastroenterology and Hepatology. 2014;12(12):1964–1972.
- Khoshini R, Dai SC, Lezcano S, Pimentel M. A Systematic Review of Diagnostic Tests for Small Intestinal Bacterial Overgrowth. Digestive Diseases and Sciences. 2008;53(6):1443–1454.
- Pimentel M, Chow EJ, Lin HC. Eradication of Small Intestinal Bacterial Overgrowth Reduces Symptoms of Irritable Bowel Syndrome. American Journal of Gastroenterology. 2000;95(12):3503–3506.
- Ghoshal UC. How to Interpret Hydrogen Breath Tests. Journal of Neurogastroenterology and Motility. 2011;17(3):312–317.
- Pimentel M, Mayer AG, Park S, Chow EJ, Hasan A, Kong Y. Methane Production During Lactulose Breath Test Is Associated with Gastrointestinal Disease Presentation. Digestive Diseases and Sciences. 2003;48(1):86–92.
- Singer-Englar T, Rezaie A, Gupta K, et al. Competitive Hydrogen Gas Utilization by Methane- and Hydrogen Sulfide-Producing Microorganisms and Associated Symptoms: Results of a Novel 4-Gas Breath Test Machine. American Journal of Gastroenterology. 2018;113:S402.
- Pimentel M, Constantino T, Kong Y, Bajwa M, Rezaei A, Park S. A 14-Day Elemental Diet Is Highly Effective in Normalizing the Lactulose Breath Test. Digestive Diseases and Sciences. 2004;49(1):73–77.
- Gasbarrini A, Corazza GR, Gasbarrini G, et al. Methodology and Indications of H2-Breath Testing in Gastrointestinal Diseases: The Rome Consensus Conference. Alimentary Pharmacology & Therapeutics. 2009;29(Suppl 1):1–49.
- Lin EC, Massey BT. Scintigraphy Demonstrates High Rate of False-Positive Results from Glucose Breath Tests for Small Bowel Bacterial Overgrowth. Clinical Gastroenterology and Hepatology. 2016;14(2):203–208.
- Bures J, Cyrany J, Kohoutova D, et al. Small Intestinal Bacterial Overgrowth Syndrome. World Journal of Gastroenterology. 2010;16(24):2978–2990.
Live PubMed Searches
Live PubMed queries that update as new papers are indexed.
- PubMed: lactulose breath test
- PubMed: glucose breath test
- PubMed: hydrogen sulfide breath test
- PubMed: SIBO diagnosis gold standard
- PubMed: SIBO false negative
- PubMed: breath test preparation diet
- PubMed: intestinal methanogen overgrowth
- PubMed: jejunal aspirate culture
Connections
- The Gut Barrier & Your Microbiome — interactive animation
- SIBO Overview
- Elemental Diet
- Root Causes
- Herbal Antimicrobials
- Prokinetics and Relapse Prevention
- Rifaximin Protocols
- Low-FODMAP Diet
- Hydrogen vs Methane vs Hydrogen Sulfide
- IMO and Constipation
- Irritable Bowel Syndrome
- Celiac Disease
- Post-Infectious IBS
- Bloating
- Constipation
- Gut Healing
- Magnesium
- Gut Microbiome
- IBS and SIBO Overlap
- Lactulose — the non-absorbable sugar used as the substrate in the standard SIBO breath test.