Prokinetics and SIBO Relapse Prevention
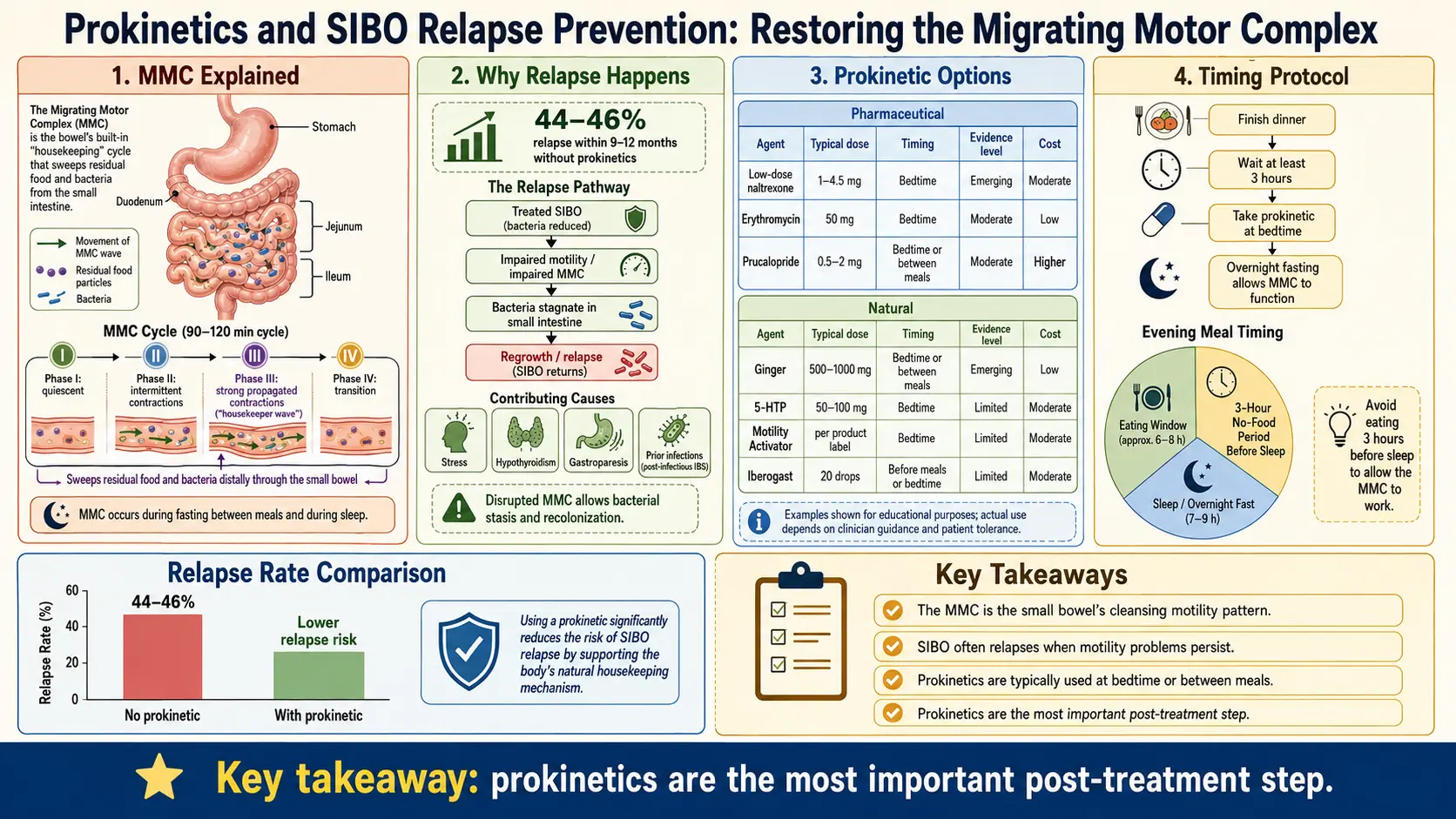
Table of Contents
- The 45% Problem
- Meet the Migrating Motor Complex (MMC)
- What Breaks the MMC
- The 4-5 Hour Meal Spacing Rule
- The Prokinetic Toolkit — Prescription
- Natural / Herbal Prokinetics
- Protocol: Starting Prokinetics After SIBO Treatment
- Lifestyle Levers That Actually Matter
- Addressing the Root Cause Is Still Part of Prevention
- What the Research Actually Shows
- Key Research Papers
- Featured Videos
1. The 45% Problem
You did the hard thing. You took the rifaximin. Or you white-knuckled your way through two weeks of an elemental diet. Or you powered through eight weeks of berberine and oregano oil. Your breath test came back clean. Your bloating went away. For the first time in years, you ate a meal without looking six months pregnant afterward.
And then, somewhere between month three and month twelve, it came back.
You are not doing anything wrong. You are not "broken." You are one of the 44-46% of SIBO patients who relapse within 9-12 months of successful eradication. This number is so consistent across studies — Pimentel, Lauritano, Ghoshal — that it is now considered the expected outcome, not the exception. Most doctors do not explain why this happens. Many will just hand you another course of rifaximin and send you home.
Here is the truth: the bacteria are not the problem. The fact that they keep coming back is the problem. Killing them again and again without fixing why they keep coming back is like mopping the floor while the faucet is still running. You will mop forever. This article is about turning off the faucet — and the single most important lever for that is restoring your migrating motor complex.
2. Meet the Migrating Motor Complex (MMC)
Your small intestine has a cleaning cycle. Between meals — when you are fasting — a wave of coordinated muscular contractions sweeps from your stomach all the way down to your ileocecal valve. This is the migrating motor complex (MMC), and it runs on a 90-120 minute loop as long as you are not eating.
The MMC has four phases, but only one really matters here. Phase III is the star of the show: a burst of strong, coordinated, high-amplitude contractions that pushes residual food particles, shed epithelial cells, mucus, and — most importantly — bacteria downstream into the colon where they belong.
Think of the MMC as the intestinal equivalent of a dishwasher rinse cycle. If the dishwasher never runs, the dishes pile up. If the MMC never runs, bacteria pile up. That is SIBO.
Gastroenterologists at Cedars-Sinai and elsewhere now consider the MMC the single most important defense mechanism against small intestinal bacterial overgrowth — more important than gastric acid, more important than the ileocecal valve, more important than immunoglobulin A. If your MMC is broken, you will keep getting SIBO no matter how many antibiotics you take.
3. What Breaks the MMC
The MMC is a delicate system. It depends on intact vagal signaling, healthy interstitial cells of Cajal (the intestinal "pacemaker" cells), and properly functioning motilin and serotonin receptors. A lot of things can damage it:
- Post-infectious IBS — a bout of food poisoning (especially Campylobacter jejuni, but also Salmonella, Shigella, E. coli, and norovirus) triggers autoantibodies against vinculin, a protein expressed on the interstitial cells of Cajal. The immune system attacks its own motility pacemakers. This is the most common identifiable cause of adult-onset SIBO.
- Diabetic autonomic neuropathy — chronically elevated blood glucose damages the vagus nerve, which controls MMC cycling.
- Hypothyroidism — low thyroid hormone slows every smooth muscle in the body, including the small intestine. SIBO prevalence in untreated hypothyroidism is around 54%.
- Opioid medications — even short courses of oxycodone, hydrocodone, tramadol, or kratom powerfully suppress the MMC through mu-receptor activation.
- Chronic stress / sympathetic overdrive — the MMC runs on the parasympathetic (rest-and-digest) branch of the nervous system. Chronic fight-or-flight shuts it down.
- Scleroderma / systemic sclerosis — smooth muscle fibrosis destroys intestinal contractility.
- Ehlers-Danlos syndrome and joint hypermobility — connective tissue laxity disrupts intestinal wall mechanics.
- Parkinson's disease — alpha-synuclein deposition in the enteric nervous system disrupts the MMC years before motor symptoms appear.
- Aging — MMC amplitude and frequency decline with age, which is part of why SIBO prevalence rises to 15-33% in adults over 60.
And the biggest everyday saboteur of all: food. The MMC is suppressed by eating. Every time you put calories in your mouth, the MMC stops. Every snack, every coffee-with-cream, every handful of nuts resets the digestive clock and aborts the cleaning cycle that was about to start.
4. The 4-5 Hour Meal Spacing Rule
This is the single cheapest, most powerful, most underutilized intervention in SIBO prevention, and it costs you nothing except a cultural habit.
Eat three meals a day. Space them 4-5 hours apart. Do not snack between them.
That is it. That is the rule. The MMC needs roughly 90-120 minutes of uninterrupted fasting after a meal to initiate a Phase III sweep. If you eat breakfast at 7, snack at 10, lunch at 12, another snack at 3, dinner at 6, and a handful of crackers at 9, your MMC never runs. You just spent the entire day telling your small intestine that food is coming, so don't clean up. Bacteria love this.
Between meals you can have: water, plain black coffee, plain black or green tea, plain herbal tea. Anything with calories — even cream in coffee, a splash of juice, a single almond — restarts the digestive phase and aborts the MMC. Gum and mints are also problematic because they trigger cephalic-phase digestion.
Overnight is your biggest MMC window. A 12-14 hour overnight fast (finish dinner by 7 pm, breakfast at 7-9 am) gives you 6-8 uninterrupted MMC cycles while you sleep. That is more cleaning than you will get all day.
5. The Prokinetic Toolkit — Prescription
When meal spacing alone is not enough — and for most people with a damaged MMC, it isn't — pharmacological prokinetics directly stimulate Phase III contractions. These are not laxatives. A laxative empties the colon. A prokinetic restores the cleaning wave of the small intestine.
Low-Dose Erythromycin (50-100 mg at bedtime)
Erythromycin is an old macrolide antibiotic, but at sub-antimicrobial doses it has a completely different action: it is a motilin receptor agonist. Motilin is the hormone that triggers Phase III of the MMC, and erythromycin mimics it directly. At 50-100 mg taken at bedtime, erythromycin is far below the dose needed to kill bacteria, but high enough to kick off a powerful cleaning wave while you sleep.
This is the most-studied prokinetic for SIBO prevention, and it has the strongest outcome data (see Research section below). Tachyphylaxis — loss of effect over time — can develop after 3-4 weeks of continuous use, because motilin receptors downregulate. Many SIBO-literate practitioners cycle it 4 weeks on / 2 weeks off to keep the receptors responsive.
Prucalopride (Motegrity / Resolor) 1-2 mg daily
Prucalopride is a highly selective 5-HT4 receptor agonist that stimulates high-amplitude propagating contractions throughout the gut. It is FDA-approved for chronic idiopathic constipation, and it is particularly useful for patients with methane-dominant SIBO (IMO) where methane gas has directly paralyzed intestinal transit. Unlike older 5-HT4 drugs (cisapride, tegaserod), prucalopride is selective enough to avoid the cardiac side effects that got its predecessors pulled from the market.
Dose is 1 mg or 2 mg once daily, usually taken in the morning. Cost without insurance runs $350-450 per month, which is the biggest practical barrier.
Low-Dose Naltrexone (LDN) 2.5-4.5 mg at bedtime
Naltrexone at full dose (50 mg) is an opioid receptor blocker used in addiction medicine. At low doses (1.5-4.5 mg) it produces a brief, partial opioid-receptor blockade that triggers a rebound release of endorphins and reduces the inhibitory tone that endogenous opioids exert on MMC cycling. It is also mildly immunomodulatory, which is helpful for the post-infectious-IBS and autoimmune subsets.
LDN must be obtained from a compounding pharmacy because the commercial 50 mg tablet is too concentrated. Typical cost: $40-70 per month. Start at 1.5 mg and titrate up over 2-4 weeks; some patients get vivid dreams during the first week.
Tegaserod (Zelnorm)
Tegaserod is a 5-HT4 partial agonist that was pulled from the US market in 2007 over cardiovascular concerns and returned in 2019 for a narrow label: women under 65 with IBS-C and no cardiovascular risk factors. It works but the restricted eligibility and prescriber hesitation mean it is rarely used for SIBO maintenance. If you qualify and tolerate it, it can be an option.
Metoclopramide / Domperidone
Older prokinetics. Metoclopramide (Reglan) crosses the blood-brain barrier and can cause tardive dyskinesia — irreversible movement disorders — with long-term use. Domperidone does not cross the blood-brain barrier but carries a QT-prolongation cardiac risk and is not FDA-approved in the United States (available through special compounding or from Canada). Neither is considered first-line for long-term SIBO prevention, though domperidone is sometimes used in severe gastroparesis overlap.
6. Natural / Herbal Prokinetics
For patients who can't access prescription prokinetics, don't tolerate them, or prefer a gentler approach, several herbal options have meaningful evidence.
Iberogast (STW 5)
Iberogast is a German liquid formula combining nine botanicals: Iberis amara (bitter candytuft), peppermint, chamomile, caraway, lemon balm, angelica, greater celandine, milk thistle, and licorice. Dose is 20 drops in water three times daily before meals. The evidence is strongest for functional dyspepsia, but it has modest data for supporting MMC function and is widely used by integrative GI practitioners for SIBO relapse prevention.
Ginger (1000 mg daily)
Ginger (Zingiber officinale) modulates 5-HT3 and 5-HT4 receptors and directly accelerates gastric emptying and small bowel transit. It takes 30-60 minutes to start working, so take it before meals, not after. Standardized extracts deliver gingerols more reliably than raw root, but either works. Cheapest option on this list and generally well tolerated.
Berberine (500 mg TID)
Berberine pulls double duty: it is a broad-spectrum antimicrobial (it is part of most herbal SIBO kill protocols) and it has mild prokinetic effects, probably through AMPK activation and modulation of serotonin signaling. Dose is 500 mg three times daily. It can reduce blood glucose, so be careful if you are on diabetes medication.
Triphala (500-1000 mg at bedtime)
Triphala is an Ayurvedic formula of three fruits: amalaki, bibhitaki, and haritaki. At 500-1000 mg at bedtime it acts as a gentle nighttime prokinetic; at higher doses it becomes a mild laxative. Many patients pair triphala with ginger for a two-front approach.
MotilPro (Pure Encapsulations)
MotilPro is a capsule combining ginger, artichoke leaf extract, and acacia fiber, plus 5-HTP and acetyl-L-carnitine. It is formulated specifically for MMC support and is one of the more popular practitioner-recommended combo products. Typical dose is 2 capsules at bedtime.
7. Protocol: Starting Prokinetics After SIBO Treatment
The timing matters. Here is the standard protocol used by SIBO-focused practitioners:
- Day 1 after finishing your antimicrobial course — whether that was 14 days of rifaximin, 4 weeks of herbals, or the day you finish refeeding from an elemental diet — start your prokinetic that night.
- Continue for at least 3 months, typically 6-12 months. The MMC does not re-train overnight. You are rebuilding a neural and hormonal rhythm.
- Continue indefinitely if the underlying cause is permanent — scleroderma, diabetic autonomic neuropathy, prior bowel resection, Parkinson's, long-standing post-infectious IBS with persistent anti-vinculin antibodies.
- Retest at 3 and 6 months with a breath test. Asymptomatic does not necessarily mean eradicated.
- Combine with meal spacing from day 1. A drug that stimulates Phase III is wasted if you eat every two hours.
8. Lifestyle Levers That Actually Matter
These are not filler. Several of them are as powerful as any medication.
- Meal spacing. 3 meals, 4-5 hours apart. This is the foundation.
- Overnight fast. 12-14 hours, every night. Eight MMC cycles while you sleep.
- No snacking. Even "healthy" snacks — an apple, a few almonds, a protein shake — reset the MMC. If you are legitimately hungry between meals, make the next meal bigger, don't add a snack.
- Post-meal walking. A 15-20 minute walk after dinner has been shown to speed gastric emptying by approximately 30%. Costs nothing, works immediately.
- Left-side sleeping. Intestinal anatomy favors downward movement of chyme when you lie on your left side. Right-side sleeping can slow transit.
- Vagal tone / stress reduction. Slow diaphragmatic breathing (inhale 4 seconds, exhale 8 seconds) for 5-10 minutes before meals. Cold-water face immersion, humming, gargling, and singing all directly stimulate the vagus nerve. Meditation, yoga, 7-8 hours of sleep. The MMC is a parasympathetic event — if you are stuck in sympathetic overdrive, it will not run.
- Don't chronically undereat or overeat. Extreme caloric restriction downregulates motility; habitually oversized meals delay gastric emptying and push back the MMC window. Regular-sized, regular-timed meals are the goal.
9. Addressing the Root Cause Is Still Part of Prevention
Prokinetics are the most powerful single lever for preventing relapse, but they do not fix the original reason your MMC broke. Depending on your situation, real root-cause work may include:
- Testing for anti-vinculin and anti-CdtB antibodies (the ibs-smart panel) to confirm post-infectious IBS.
- Evaluating and treating hypothyroidism, including sub-clinical cases where TSH is "normal" but free T3 is low.
- Reconsidering PPI therapy — the acid barrier matters.
- Investigating ileocecal valve dysfunction, adhesions from prior surgery, or intestinal structural issues.
- Screening for Ehlers-Danlos / hypermobility spectrum if you have joint laxity, POTS, or MCAS overlap.
See the Root Causes article for the full workup.
10. What the Research Actually Shows
The single most important study in this entire conversation comes from Pimentel's group at Cedars-Sinai. In patients who had been successfully eradicated of SIBO with antibiotics, the 12-month recurrence rate was 43.7% in the untreated control group. In the group placed on nightly low-dose erythromycin (50 mg at bedtime), the recurrence rate dropped to approximately 20%.
That is the number to remember. Prokinetic therapy cuts SIBO relapse roughly in half. No other intervention — not diet, not probiotics, not repeat antibiotics — has produced an effect that large in SIBO prevention.
Head-to-head comparisons of prokinetics against each other in SIBO specifically do not yet exist in randomized-controlled-trial form. Current choices (erythromycin vs. prucalopride vs. LDN vs. herbal) are made on the basis of cost, access, tolerance, concurrent IBS subtype (constipation vs. diarrhea), and individual response. This is one of the biggest gaps in SIBO research and an area of active investigation.
11. Key Research Papers
Peer-reviewed literature on the migrating motor complex, prokinetic pharmacology, and SIBO relapse prevention. Each citation links to the full text via DOI.
- Pimentel M, Saad RJ, Long MD, Rao SSC. ACG Clinical Guideline: Small Intestinal Bacterial Overgrowth. American Journal of Gastroenterology. 2020;115(2):165–178.
- Pimentel M, Soffer EE, Chow EJ, Kong Y, Lin HC. Lower Frequency of MMC Is Found in IBS Subjects with Abnormal Lactulose Breath Test, Suggesting Bacterial Overgrowth. Digestive Diseases and Sciences. 2002;47(12):2639–2643.
- Pimentel M, Morales W, Pokkunuri V, et al. Autoimmunity Links Vinculin to the Pathophysiology of Chronic Functional Bowel Changes Following Campylobacter jejuni Infection in a Rat Model. Digestive Diseases and Sciences. 2015;60(5):1195–1205.
- Pimentel M, Lin HC, Enayati P, et al. Methane, a Gas Produced by Enteric Bacteria, Slows Intestinal Transit and Augments Small Intestinal Contractile Activity. American Journal of Physiology — Gastrointestinal and Liver Physiology. 2006;290(6):G1089–G1095.
- Pimentel M, Morales W, Lezcano S, Sun-Chuan D, Low K, Yang J. Low-Dose Nocturnal Tegaserod or Erythromycin Delays Symptom Recurrence after Treatment of Irritable Bowel Syndrome Based on Presumed Bacterial Overgrowth. Gastroenterology & Hepatology. 2009;5(6):435–442.
- Tack J, van Outryve M, Beyens G, Kerstens R, Vandeplassche L. Prucalopride (Resolor) in the Treatment of Severe Chronic Constipation in Patients Dissatisfied with Laxatives. Gut. 2009;58(3):357–365.
- Camilleri M, Beyens G, Kerstens R, Robinson P, Vandeplassche L. Safety Assessment of Prucalopride in Elderly Patients with Constipation: A Double-Blind, Placebo-Controlled Study. Neurogastroenterology & Motility. 2009;21(12):1256–e117.
- Lauritano EC, Gabrielli M, Scarpellini E, et al. Small Intestinal Bacterial Overgrowth Recurrence after Antibiotic Therapy. American Journal of Gastroenterology. 2008;103(8):2031–2035.
- Chedid V, Dhalla S, Clarke JO, et al. Herbal Therapy Is Equivalent to Rifaximin for the Treatment of Small Intestinal Bacterial Overgrowth. Global Advances in Health and Medicine. 2014;3(3):16–24.
- Pittman N, Rawn SM, Wang M, Masetto A, Beattie KA, Larché M. Treatment of Small Intestinal Bacterial Overgrowth in Systemic Sclerosis: A Systematic Review. Rheumatology. 2018;57(10):1802–1811.
- Madisch A, Holtmann G, Plein K, Hotz J. Treatment of Irritable Bowel Syndrome with Herbal Preparations: Results of a Double-Blind, Randomized, Placebo-Controlled, Multi-Centre Trial. Alimentary Pharmacology & Therapeutics. 2004;19(3):271–279.
- Hu Y, Bai Y, Hu G, et al. Effects of Linaclotide on Symptoms in IBS-C and Chronic Idiopathic Constipation: A Systematic Review and Meta-Analysis. Aliment Pharmacol Ther. 2022;55(6):635–647.
Live PubMed Searches
Live PubMed queries that update as new papers are indexed.
- PubMed: migrating motor complex and SIBO
- PubMed: low-dose erythromycin prokinetic
- PubMed: prucalopride and SIBO
- PubMed: SIBO recurrence prevention
- PubMed: low-dose naltrexone and gut motility
- PubMed: Iberogast and functional dyspepsia
- PubMed: ginger and gastric motility
Connections
- The Gut Barrier & Your Microbiome — interactive animation
- SIBO Overview
- Root Causes
- Elemental Diet
- Rifaximin Protocols
- Low-FODMAP Diet
- Herbal Antimicrobials
- Hydrogen vs Methane vs Hydrogen Sulfide
- Breath Test Guide
- IMO and Constipation
- Irritable Bowel Syndrome
- Thyroid Disorders
- POTS
- Post-Infectious IBS
- Ginger
- Berberine
- Constipation
- Gut Healing
- Bloating