Low-FODMAP Diet for SIBO
If your doctor handed you a one-page FODMAP list and sent you on your way, this article is for you. The low-FODMAP diet works — but not the way most people are taught to use it. It is a diagnostic tool with three distinct phases, not a permanent way of eating, and the middle phase (the one almost everyone skips) is where the real answers live. Here is the whole map, written for tired people who are reading this in the cereal aisle.
Interactive Visualization The Gut Barrier & Your Microbiome Watch fibre become butyrate and butyrate tighten the gut wall — then starve the microbes and see them eat your mucus layer instead. Launch →Table of Contents
- What FODMAP Even Means
- The Three Phases (This Is Important)
- The FODMAP Categories, with Food Lists
- A Sample Low-FODMAP Day
- Why You Should NOT Stay Low-FODMAP Long-Term
- Low-FODMAP vs. SCD vs. Bi-Phasic Diet
- Why Diet Alone Doesn't Cure SIBO
- Apps and Resources
- Working with a Dietitian
- Key Research Papers
- Connections
- Featured Videos
1. What FODMAP Even Means
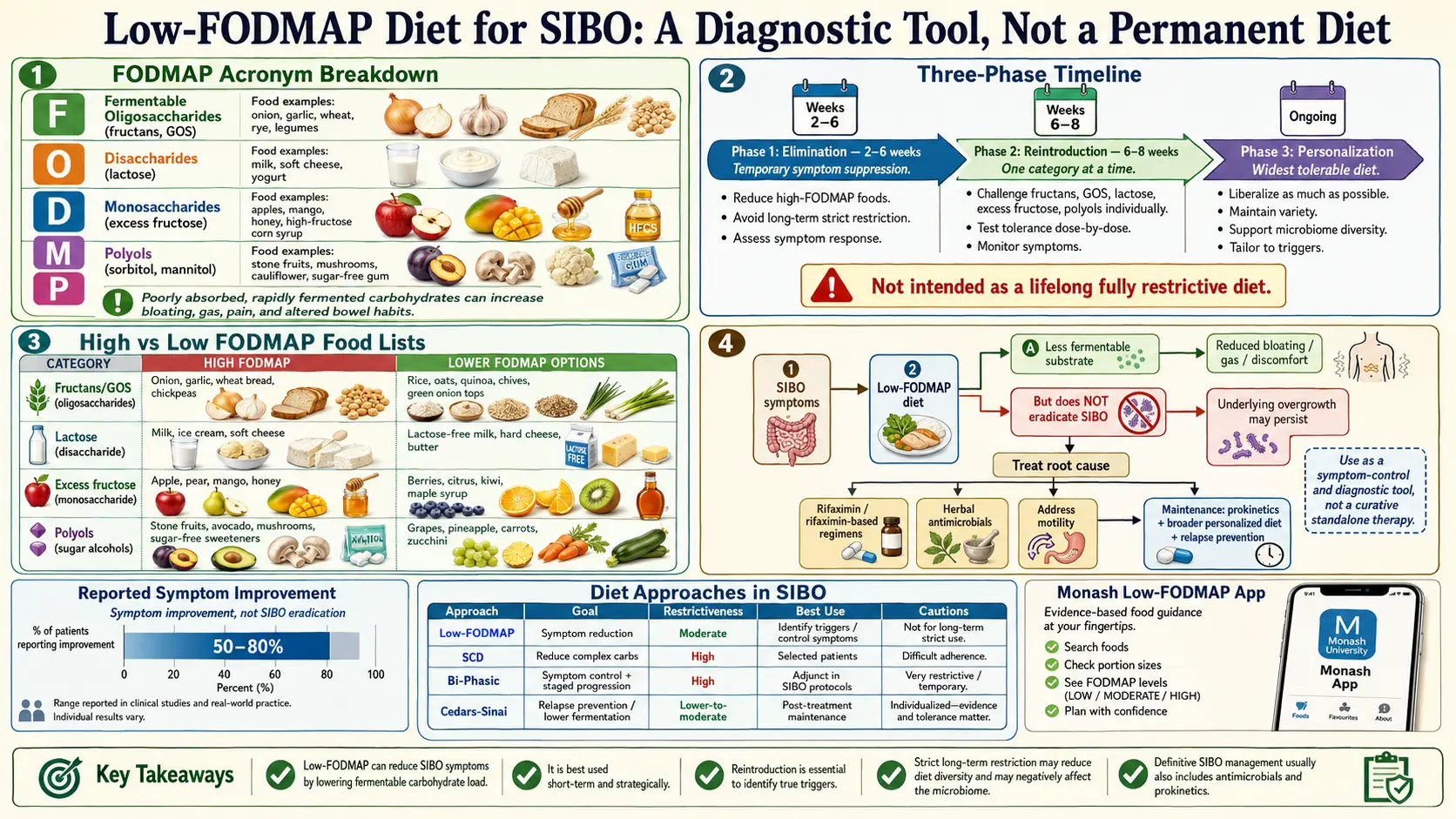
FODMAP is an acronym — not a food group, not a toxin, just a cluster of carbohydrate shapes that share one inconvenient property. It stands for Fermentable Oligosaccharides, Disaccharides, Monosaccharides And Polyols. These are short-chain carbohydrates that the human small intestine absorbs poorly (or not at all) but that bacteria absolutely love.
The concept was developed at Monash University in Melbourne, Australia, by gastroenterologist Peter Gibson and dietitian Sue Shepherd around 2005. Their insight was simple: if your small intestine is harboring more bacteria than it should (SIBO), and those bacteria ferment carbohydrates into hydrogen, methane, and hydrogen sulfide, then logically — remove the substrate and you remove the gas, bloating, and pain.
Low-FODMAP is not about eating "healthier." It is about starving bacteria of their favorite fuel long enough to quiet symptoms and figure out which specific fuels your bacteria overreact to. A banana is a perfectly healthy food. In someone with SIBO, a ripe banana becomes a buffet.
2. The Three Phases (This Is Important)
This is the section most people never hear about. The low-FODMAP diet is a three-phase protocol. Most patients only ever do Phase 1, stay on it for months or years, and wonder why they feel worse. Here is how it is actually supposed to work.
Phase 1: Elimination (2 to 6 weeks — not longer)
Remove all high-FODMAP foods. Every category, strictly, for 2 to 6 weeks. The goal is to reach a clear symptom baseline — a quieter gut, less bloating, more predictable bowel movements. If symptoms do not improve at all after 4 weeks of strict elimination, FODMAPs are probably not your main driver and you should stop and reassess with a clinician.
Do not stay in this phase indefinitely. Phase 1 is diagnostic. It is the equivalent of turning off every appliance in the house to see which one was tripping the breaker — useful for a day, not a way to live.
Phase 2: Reintroduction / Challenge (6 to 8 weeks)
This is the most-skipped and the most important phase. Once symptoms have stabilized, you reintroduce one FODMAP category at a time, over three days, while watching your body's response. A typical challenge looks like this:
- Day 1: small serving of the test food (for example, 1/4 avocado for polyols).
- Day 2: medium serving (1/2 avocado).
- Day 3: normal serving (whole avocado).
- Then 2 to 3 washout days of strict low-FODMAP before challenging the next category.
You are not testing whether a food is "good" or "bad." You are measuring your personal dose threshold for each category. Most people tolerate some FODMAPs fine and react strongly to only one or two.
Phase 3: Personalization
You now have a map. You know, for example, that you tolerate lactose and polyols but fructans wreck you. Phase 3 is the long-term diet built from that map: eat normally, keep your trigger FODMAPs restricted, and re-test tolerance every few months because tolerance changes as SIBO is treated.
The goal is the widest possible diet you can eat comfortably — not the narrowest.
3. The FODMAP Categories, with Food Lists
Each FODMAP subgroup has its own biology and its own food list. The lists below are representative, not exhaustive — always cross-check a specific food against the Monash app before a challenge.
Fructans (Oligosaccharides)
Chains of fructose. Humans do not produce the enzyme to break them down, so everyone ferments fructans to some degree — the question is how much. Fructans are the single biggest symptom driver in most SIBO patients.
- High (avoid in Phase 1): wheat, rye, barley, garlic, onion, leek, shallots, scallions (white part), artichokes, chicory root, inulin-fortified foods.
- Low (allowed): firm/green banana, carrot, bell pepper, cucumber, potato, rice, oats, quinoa, scallion greens, garlic-infused oil (the fructans are water-soluble, not oil-soluble).
GOS (Galacto-oligosaccharides)
Short chains of galactose found mainly in legumes. Like fructans, humans cannot digest them — which is why beans produce gas in basically everyone.
- High: lentils, chickpeas, kidney beans, black beans, soybeans, cashews, pistachios.
- Low: canned and well-drained lentils or chickpeas (draining removes much of the GOS), firm tofu, tempeh, peanuts, macadamia nuts, walnuts.
Lactose (Disaccharide)
Milk sugar. Roughly 65% of adults worldwide are lactase-deficient to some degree, so this one is often already familiar.
- High: cow's milk, goat's milk, soft cheese (ricotta, cottage, cream cheese), yogurt, ice cream, custard.
- Low: lactose-free milk, hard aged cheeses (cheddar, parmesan, Swiss — the aging process digests the lactose), butter, lactose-free yogurt, almond/coconut milk.
Fructose in Excess (Monosaccharide)
Fructose is only a FODMAP when it exists in excess of glucose in the same food. Glucose helps fructose absorb; an imbalance leaves fructose stranded in the gut to be fermented.
- High: honey, apples, pears, mango, watermelon, high-fructose corn syrup, agave, dried fruit, fruit juice concentrates.
- Low: strawberries, blueberries, raspberries, oranges, grapes, kiwi, pineapple, cantaloupe, table sugar (sucrose is balanced 1:1).
Polyols (Sorbitol and Mannitol)
Sugar alcohols. Poorly absorbed by design — which is why sugar-free gum gives most people diarrhea.
- High (sorbitol): apples, pears, stone fruits (peaches, plums, cherries, apricots, nectarines), blackberries, avocado (more than 1/8), sugar-free gum and mints (sorbitol, xylitol, maltitol, isomalt).
- High (mannitol): mushrooms, cauliflower, snow peas, celery, sweet potato (large servings).
- Low: grapes, kiwi, strawberries, zucchini, carrots, cucumber, spinach, lettuce, green beans.
4. A Sample Low-FODMAP Day
Phase 1 does not have to be grim. Here is what a normal day can look like:
- Breakfast: oatmeal cooked in lactose-free milk, topped with blueberries, a handful of walnuts, and a drizzle of maple syrup. Black coffee or green tea.
- Mid-morning snack: a firm banana and a small handful of peanuts, or a rice cake with peanut butter.
- Lunch: grilled chicken over rice with roasted carrots, zucchini, and bell peppers, dressed with olive oil, lemon, salt, and a splash of garlic-infused oil for flavor.
- Afternoon snack: carrot sticks with lactose-free Greek yogurt dip, or a square of dark chocolate (check ingredients — no inulin).
- Dinner: pan-seared salmon, mashed potato with butter and chives (green part only), sauteed spinach with garlic-infused oil.
- Dessert: strawberries with a scoop of lactose-free vanilla ice cream.
- Drinks all day: water, black/green tea, peppermint tea, coffee (watch dairy), still or sparkling water with lemon.
That is three meals, three snacks, and every major food group — no garlic, no onion, no wheat, no apples, no milk, and not a shred of deprivation.
5. Why You Should NOT Stay Low-FODMAP Long-Term
Here is what almost no one tells patients: the foods you are removing are the same foods that feed your beneficial gut bacteria. FODMAPs are prebiotics. Strip them out and you starve the overgrowth — but you also starve Bifidobacterium, Faecalibacterium prausnitzii, and other commensals that keep the colon healthy.
Staudacher et al. (2015, Gut) showed that after just 4 weeks of strict low-FODMAP eating, stool Bifidobacterium populations dropped measurably and significantly compared to controls on a normal diet. Bennet et al. (2018, Gut) and others have since confirmed that long-term low-FODMAP correlates with reduced overall microbiome diversity — the opposite of what you want for long-term gut health.
A narrower microbiome is a more fragile microbiome. It recovers more slowly from antibiotics, is more prone to Clostridioides difficile, and may even worsen food sensitivities over time as the gut's tolerance for variety shrinks.
The rule of thumb: Phase 1 for 2 to 6 weeks. Phase 2 systematically. Phase 3 forever. Not the other way around.
6. Low-FODMAP vs. SCD vs. Bi-Phasic Diet
Three different dietary frameworks get recommended for SIBO. They overlap but are not the same.
- Low-FODMAP (Monash): restricts fermentable carbohydrates by category. Best-studied. Designed originally for IBS, later applied to SIBO. Structured three-phase protocol.
- Specific Carbohydrate Diet (SCD): developed by Sidney Haas and popularized by Elaine Gottschall's Breaking the Vicious Cycle. Eliminates all grains, most disaccharides, and starches — only monosaccharides are allowed. Stricter than low-FODMAP and not phase-structured. Often used for IBD.
- SIBO Bi-Phasic Diet (Dr. Nirala Jacobi): specifically designed for SIBO. Combines the low-FODMAP framework with the carbohydrate restrictions of SCD, structured into two phases over roughly 8 weeks with clear food lists for each phase. It is the most SIBO-specific of the three and is often easier to follow than trying to merge low-FODMAP and SCD rules on your own.
For most SIBO patients starting out, low-FODMAP is the reasonable first attempt. If it helps but not enough, the Bi-Phasic Diet is the natural next step.
7. Why Diet Alone Doesn't Cure SIBO
This is the hard truth. Low-FODMAP relieves symptoms by reducing the fuel bacteria use to produce gas. It does not reduce the number of bacteria in your small intestine. The overgrowth is still there; you have just put it on a diet.
Stop low-FODMAP without treating the underlying SIBO, and symptoms return within days. This is why patients often conclude "I have to eat this way forever" — because the diet is the only thing holding symptoms down. It is a valid coping strategy, but it is not a cure, and it has a real microbiome cost.
Real eradication requires attacking the overgrowth directly — see the pages on rifaximin protocols and herbal antimicrobials — and then preventing relapse by identifying why the overgrowth happened in the first place. See root causes. Diet is a supporting player, not the protagonist.
8. Apps and Resources
- Monash University FODMAP Diet app (iOS and Android, paid): the gold standard. Monash researchers developed the FODMAP framework and continue to test specific foods in their lab. Their traffic-light system (green/yellow/red per serving size) is the only source that reflects current lab data. If you use one tool, use this one.
- FODMAP Friendly (Australian certification program): a second certification body that tests packaged foods and labels qualifying products. Useful in supermarkets for scanning boxes.
- Fig (free): lets you scan a grocery barcode and filter against low-FODMAP (and other) dietary needs. Not as rigorous as Monash but helpful for quick shopping checks.
- Monash blog and recipes: the Monash University department of gastroenterology publishes recipes and updates as foods are retested.
9. Working with a Dietitian
Phase 2 reintroduction is genuinely hard to do alone. The protocol requires careful food journaling, dose laddering, and washout periods. Most people — especially exhausted, overwhelmed SIBO patients — abandon it halfway and either spring-release back to their old diet or stay stuck in Phase 1 forever.
A registered dietitian (RD) with GI and SIBO training can make the difference between success and a lost six months. Monash maintains a Monash-certified dietitian directory of RDs who have completed their FODMAP training; this is the most reliable place to find one. A good SIBO RD will structure the reintroduction schedule, interpret ambiguous reactions, and adapt the plan as you go.
If cost is a barrier, even one or two sessions — one to plan Phase 2, one to interpret results — is usually enough. Ask whether your insurance covers medical nutrition therapy (MNT) for IBS, SIBO, or functional GI disorders; many plans do.
10. Key Research Papers
Peer-reviewed studies on the low-FODMAP diet for IBS and SIBO — mechanisms, clinical efficacy, microbiome impact, and reintroduction strategy. Each citation links to the full text via DOI.
- Halmos EP, Power VA, Shepherd SJ, Gibson PR, Muir JG. A Diet Low in FODMAPs Reduces Symptoms of Irritable Bowel Syndrome. Gastroenterology. 2014;146(1):67–75.
- Böhn L, Störsrud S, Liljebo T, et al. Diet Low in FODMAPs Reduces Symptoms of Irritable Bowel Syndrome as Well as Traditional Dietary Advice: A Randomized Controlled Trial. Gastroenterology. 2015;149(6):1399–1407.
- Staudacher HM, Whelan K. The Low FODMAP Diet: Recent Advances in Understanding Its Mechanisms and Efficacy in IBS. Gut. 2017;66(8):1517–1527.
- Staudacher HM, Lomer MCE, Anderson JL, et al. Fermentable Carbohydrate Restriction Reduces Luminal Bifidobacteria and Gastrointestinal Symptoms in Patients with Irritable Bowel Syndrome. Journal of Nutrition. 2012;142(8):1510–1518.
- Marsh A, Eslick EM, Eslick GD. Does a Diet Low in FODMAPs Reduce Symptoms Associated with Functional Gastrointestinal Disorders? A Comprehensive Systematic Review and Meta-Analysis. European Journal of Nutrition. 2016;55(3):897–906.
- Pimentel M, Saad RJ, Long MD, Rao SSC. ACG Clinical Guideline: Small Intestinal Bacterial Overgrowth. American Journal of Gastroenterology. 2020;115(2):165–178.
- Bennet SMP, Böhn L, Störsrud S, et al. Multivariate Modelling of Faecal Bacterial Profiles and FODMAP Response in IBS. Gut. 2018;67(5):872–881.
- Eswaran SL, Chey WD, Han-Markey T, Ball S, Jackson K. A Randomized Controlled Trial Comparing the Low FODMAP Diet vs. Modified NICE Guidelines in US Adults with IBS-D. American Journal of Gastroenterology. 2016;111(12):1824–1832.
- Tuck CJ, Muir JG, Barrett JS, Gibson PR. Fermentable Oligosaccharides, Disaccharides, Monosaccharides and Polyols: Role in Irritable Bowel Syndrome. Expert Review of Gastroenterology & Hepatology. 2014;8(7):819–834.
- Pimentel M, Chow EJ, Lin HC. Eradication of Small Intestinal Bacterial Overgrowth Reduces Symptoms of Irritable Bowel Syndrome. American Journal of Gastroenterology. 2000;95(12):3503–3506.
- Hill P, Muir JG, Gibson PR. Controversies and Recent Developments of the Low-FODMAP Diet. Gastroenterology & Hepatology. 2017;13(1):36–45.
- Chedid V, Dhalla S, Clarke JO, et al. Herbal Therapy Is Equivalent to Rifaximin for the Treatment of Small Intestinal Bacterial Overgrowth. Global Advances in Health and Medicine. 2014;3(3):16–24.
Live PubMed Searches
Live PubMed queries that update as new papers are indexed.
- PubMed: low-FODMAP diet and SIBO
- PubMed: FODMAP reintroduction protocols
- PubMed: FODMAP, microbiome, Bifidobacterium
- PubMed: SIBO elimination diets
- PubMed: low-FODMAP IBS randomized trials
- PubMed: fructans and GI symptoms
- PubMed: bi-phasic SIBO diet
- PubMed: specific carbohydrate diet
Connections
- The Gut Barrier & Your Microbiome — interactive animation
- SIBO Overview
- Root Causes
- Herbal Antimicrobials
- Rifaximin Protocols
- Elemental Diet
- Prokinetics and Relapse Prevention
- Hydrogen vs Methane vs Hydrogen Sulfide
- Breath Test Guide
- IMO and Constipation
- Irritable Bowel Syndrome
- Low-FODMAP Diet for IBS
- Celiac Disease
- Elimination Diet
- Gut Healing
- Probiotics
- Bloating
- Peppermint
- Abdominal Pain