Chronic Diarrhea
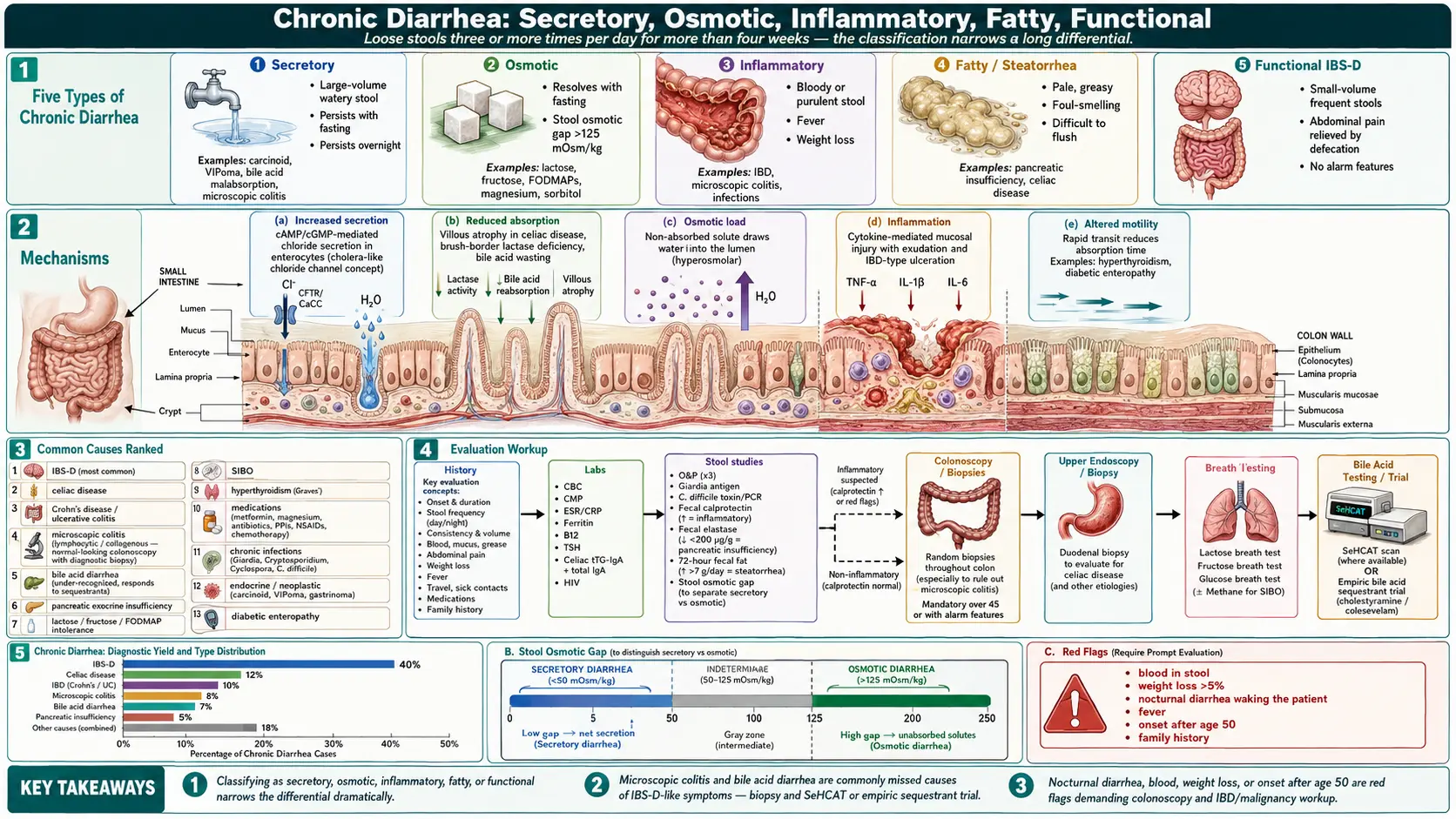
Table of Contents
- Overview
- Types of Chronic Diarrhea
- Common Causes
- Mechanisms
- Evaluation
- Management
- When to Seek Medical Care
- Connections
- References & Research
- Featured Videos
Overview
Chronic diarrhea is loose or watery stools occurring three or more times per day, persisting for more than four weeks. It is one of the most common reasons for gastroenterology referral, and unlike acute diarrhea (which is almost always infectious and self-limited), chronic diarrhea has a long differential that includes irritable bowel syndrome, celiac disease, inflammatory bowel disease, microscopic colitis, bile acid malabsorption, lactose and fructose intolerance, hyperthyroidism, and pancreatic insufficiency. The classic categorization — secretory, osmotic, inflammatory, and motility-related — helps narrow the workup.
Types of Chronic Diarrhea
- Secretory — large-volume, watery stools that persist with fasting; persistent overnight; due to abnormal ion transport. Causes include carcinoid, VIPoma, bile acid malabsorption, microscopic colitis.
- Osmotic — resolves with fasting; stool osmotic gap >125 mOsm/kg. Causes include lactose / fructose / FODMAP intolerance, magnesium-containing laxatives, sorbitol.
- Inflammatory — bloody or pus-containing stool, fever, weight loss, abdominal pain. IBD, microscopic colitis, infections.
- Fatty (steatorrhea) — pale, greasy, foul-smelling, hard to flush. Pancreatic insufficiency, celiac, small-bowel disease.
- Functional (IBS-D) — small-volume frequent stools associated with abdominal pain; relieved by defecation; no alarm features.
Common Causes
- Irritable bowel syndrome (IBS-D) — the most common cause; functional, with normal labs and imaging.
- Celiac disease — gluten-driven small-bowel inflammation.
- Crohn's disease and ulcerative colitis — chronic inflammatory bowel disease.
- Microscopic colitis (lymphocytic, collagenous) — large-volume watery diarrhea with normal-looking colonoscopy; biopsy is diagnostic.
- Bile acid diarrhea — under-recognized cause of IBS-D-like symptoms; responds to bile acid sequestrants.
- Pancreatic exocrine insufficiency — chronic pancreatitis, cystic fibrosis, pancreatic resection; presents with steatorrhea and weight loss.
- Lactose, fructose, FODMAP intolerance — osmotic diarrhea after specific foods.
- Small intestinal bacterial overgrowth — particularly in patients with motility disorders or surgical history.
- Hyperthyroidism (Graves' disease) — rapid GI transit causes diarrhea.
- Medications — metformin, magnesium, antibiotics, PPIs, NSAIDs, chemotherapy.
- Infections (chronic) — Giardia, Cryptosporidium, Cyclospora, Clostridioides difficile, post-infectious IBS.
- Endocrine and neoplastic — carcinoid syndrome, VIPoma, gastrinoma (Zollinger-Ellison), medullary thyroid cancer.
- Diabetic enteropathy — autonomic neuropathy with rapid transit.
Mechanisms
- Increased secretion — abnormal cAMP- or cGMP-mediated chloride secretion from enterocytes (cholera-like).
- Reduced absorption — mucosal injury (celiac, IBD), brush-border enzyme deficiency (lactase), bile acid wasting.
- Osmotic load — non-absorbed solutes (lactose, fructose, FODMAPs, magnesium, mannitol) draw water into the lumen.
- Inflammation — cytokine-mediated mucosal injury and exudation.
- Altered motility — rapid transit reduces absorption time; relevant in hyperthyroidism, IBS-D, diabetic enteropathy.
Evaluation
- History — duration, stool description, weight loss, blood, nocturnal symptoms, travel, food triggers, medications, family history of IBD or celiac.
- Bloodwork — CBC, CMP, ESR/CRP, ferritin, B12, TSH, celiac serology (tTG-IgA + total IgA), HIV.
- Stool studies — ova and parasites, Giardia antigen, C. difficile, fecal calprotectin (separates inflammatory from functional), fecal elastase (pancreatic insufficiency).
- 72-hour fecal fat — for steatorrhea workup.
- Stool osmotic gap — secretory vs osmotic.
- Colonoscopy with random biopsies — rules out microscopic colitis and IBD; mandatory for over 45 or with alarm features.
- Upper endoscopy with duodenal biopsy — if celiac or small-bowel disease suspected.
- Hydrogen / methane breath testing — lactose, fructose, SIBO; see the Breath Test Guide.
- SeHCAT or 75Se-homocholic acid scan — for bile acid diarrhea (limited availability in U.S.)
- Empiric trial of bile acid sequestrant — in suspected bile acid diarrhea when SeHCAT is not available.
Management
- Treat the underlying cause — gluten-free diet for celiac, biologics for IBD, levothyroxine taper or treatment for hyperthyroidism, pancreatic enzymes for insufficiency, rifaximin for SIBO, bismuth or budesonide for microscopic colitis.
- IBS-D — low-FODMAP diet, soluble fiber, peppermint oil, antispasmodics, eluxadoline, alosetron, rifaximin, low-dose tricyclics, gut-directed hypnotherapy.
- Bile acid sequestrants — cholestyramine, colesevelam, colestipol for bile acid diarrhea.
- Loperamide — symptomatic, after infection ruled out and root cause being addressed.
- Diet modification — lactose-free, low-FODMAP, fat-restricted (in steatorrhea), gluten-free (in celiac).
- Hydration and electrolyte repletion — oral rehydration solutions in severe diarrhea.
- Probiotics — mixed evidence; Saccharomyces boulardii for antibiotic-associated diarrhea.
When to Seek Medical Care
- Blood in the stool, melena, or persistent rectal bleeding.
- Unintentional weight loss greater than 5 percent of body weight.
- Nocturnal diarrhea waking the patient from sleep.
- Persistent fever with diarrhea.
- Severe abdominal pain or progressive distension.
- Signs of dehydration (dizziness, decreased urine output).
- Diarrhea after recent travel, antibiotics, or hospitalization.
- Family history of colon cancer, IBD, or celiac disease.
- Onset after age 50 (rule out malignancy and microscopic colitis).
Connections
- Irritable Bowel Syndrome
- Celiac Disease
- Inflammatory Bowel Disease
- SIBO
- Crohn's Disease
- Graves' Disease
- Abdominal Pain
- SIBO Breath Test Guide
- Constipation
- Gut Healing
- Bloating
- Gluten-Free Diet Guide
- Ulcerative Colitis
- Magnesium
- Peppermint
- Surgery Decisions Resection J Pouch Ostomy
- Bile Acid Malabsorption in IBS D
References & Research
Historical Background
The 1971 publication of the bile acid diarrhea concept (Hofmann), the 1980 description of microscopic colitis (Read), and the 2010 development of the IBSchek/IBSmart antibody-based diagnostic for post-infectious IBS each transformed pieces of what had been called "functional diarrhea" into specific diagnoses with targeted treatments.
Key Research Papers
- Smalley W, Falck-Ytter C, Carrasco-Labra A, Wani S, Lytvyn L, Falck-Ytter Y. AGA clinical practice guidelines on the laboratory evaluation of functional diarrhea and diarrhea-predominant irritable bowel syndrome in adults. Gastroenterology. 2019;157(3):851-854.
- Vijayvargiya P, Camilleri M, Carlson P, et al. Performance characteristics of serum C4 and FGF19 measurements to exclude the diagnosis of bile acid diarrhoea in IBS-diarrhoea and functional diarrhoea. Alimentary Pharmacology & Therapeutics. 2017;46(6):581-588.
- Schiller LR, Pardi DS, Sellin JH. Chronic diarrhea: diagnosis and management. Clinical Gastroenterology and Hepatology. 2017;15(2):182-193.
- Pardi DS, Kelly CP. Microscopic colitis. Gastroenterology. 2011;140(4):1155-1165.
- Mayer EA, Savidge T, Shulman RJ. Brain-gut microbiome interactions and functional bowel disorders. Gastroenterology. 2014;146(6):1500-1512.
- Halmos EP, Power VA, Shepherd SJ, Gibson PR, Muir JG. A diet low in FODMAPs reduces symptoms of irritable bowel syndrome. Gastroenterology. 2014;146(1):67-75.
- Hill ID, Fasano A, Guandalini S, et al. NASPGHAN clinical report on the diagnosis and treatment of gluten-related disorders. Journal of Pediatric Gastroenterology and Nutrition. 2016;63(1):156-165.
- Lacy BE, Pimentel M, Brenner DM, et al. ACG clinical guideline: management of irritable bowel syndrome. American Journal of Gastroenterology. 2021;116(1):17-44.
- Vijayvargiya P, Camilleri M, Burton D, Busciglio I, Lueke A, Donato LJ. Bile acid deficiency in a subgroup of patients with irritable bowel syndrome with constipation based on biomarkers in serum and fecal samples. Clinical Gastroenterology and Hepatology. 2018;16(4):522-527.
- Pimentel M, Morales W, Rezaie A, et al. Development and validation of a biomarker for diarrhea-predominant irritable bowel syndrome in human subjects. PLoS One. 2015;10(5):e0126438.
PubMed Topic Searches
- Chronic diarrhea evaluation
- Microscopic colitis diagnosis
- Bile acid diarrhea / SeHCAT
- Fecal calprotectin in IBD vs IBS
- Post-infectious IBS
- Pancreatic insufficiency and steatorrhea