Starch-Free Diet and the Ebringer Hypothesis
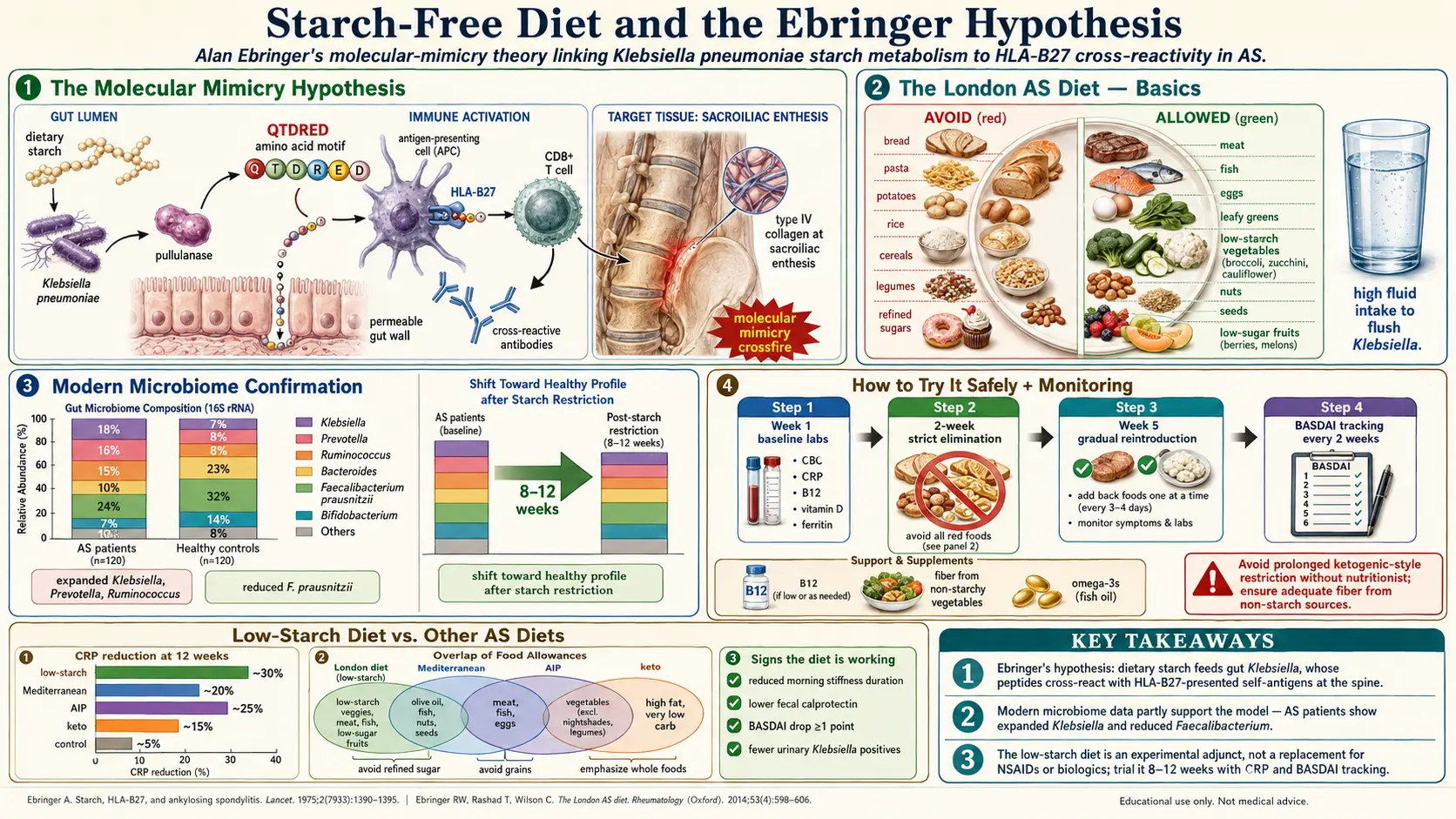
Table of Contents
- Who Was Alan Ebringer?
- The Molecular Mimicry Hypothesis
- Why Starch?
- The London AS Diet — Basics
- What's the Evidence?
- Modern Gut-Microbiome Research
- How to Try It Safely
- Low-Starch vs Keto vs AIP vs Mediterranean
- Foods to Avoid
- Foods Allowed Generously
- A Practical Sample Day
- Supplements Often Paired
- Signs It's Working
- Limits and Risks
- What Researchers Are Watching
- Key Research Papers
- Connections
- Featured Videos
If you have AS, you have probably run into the "low-starch diet" on a forum, a podcast, or in a 1990s paperback called The New Arthritis Breakthrough by Henry Scammell and Thomas Brown. Somewhere in that thread there is usually a reference to an Alan Ebringer and Klebsiella pneumoniae. This page is an honest look at that hypothesis — what it claims, what the evidence actually says, and how to give it a fair trial without wrecking your nutrition or replacing real medical care.
Who Was Alan Ebringer?
Alan Ebringer (1936–2018) was an Australian-born rheumatologist and immunologist who spent most of his career at King's College London, where he ran a rheumatology clinic and immunology research group for roughly four decades. He was a clinician first and a theorist second: his patients were real AS sufferers being seen at the Middlesex Hospital and later King's, and the "London AS Diet" grew out of what he watched work in that clinic.
Ebringer published steadily from the late 1970s through the 2010s on a single big idea: that many chronic autoimmune diseases are triggered and sustained by specific gut or urinary bacteria whose surface proteins look enough like human self-tissue to fool the immune system. For AS, the suspect bacterium was Klebsiella pneumoniae. For rheumatoid arthritis, it was Proteus mirabilis. For multiple sclerosis, Acinetobacter. He argued, with steady consistency, that reducing the bacterial load by dietary means could reduce disease activity.
Mainstream rheumatology never fully embraced him, but it also never cleanly refuted him. He was taken seriously enough to publish in peer-reviewed journals for forty years, and many of his clinic patients — some of whom are still posting on AS forums today — credit his diet with keeping them functional for decades.
The Molecular Mimicry Hypothesis
The core idea is simple, and the biology behind it is real. Molecular mimicry is the phenomenon in which a short amino-acid sequence on a microbe happens to resemble a short sequence on a human protein closely enough that antibodies (or T-cell receptors) raised against the microbe also bind the human protein. When that happens in the wrong tissue, you get autoimmune damage.
Ebringer's group identified two key resemblances:
- A six-amino-acid sequence (Gln-Thr-Asp-Arg-Glu-Asp, or QTDRED) in the Klebsiella nitrogenase reductase enzyme closely matches a sequence in the HLA-B27 molecule itself.
- Sequences in the Klebsiella pullulanase enzyme resemble sequences in human type I, III, and IV collagen — the structural proteins of cartilage, entheses, and the joint capsule.
The proposed chain of events: HLA-B27-positive person has chronic low-grade Klebsiella overgrowth in the gut, their immune system makes antibodies against Klebsiella, those antibodies (and cross-reactive T cells) then bind HLA-B27-bearing cells and collagen-rich tissue in the spine and sacroiliac joints, and the resulting friendly fire is what shows up on MRI as sacroiliitis. Ebringer's cohort studies repeatedly measured elevated serum IgA anti-Klebsiella antibodies in active AS patients compared with healthy HLA-B27 controls, and he argued this was the fingerprint of the process.
Is mimicry alone sufficient to cause disease? Probably not — plenty of people carry cross-reactive antibodies without getting sick. But mimicry combined with HLA-B27's unusual biology (see HLA-B27 Explained), increased gut permeability, and a genetically primed IL-23/IL-17 axis is a plausible multi-hit explanation for why AS happens.
Why Starch?
Klebsiella pneumoniae is a facultative anaerobe that ferments a wide range of sugars, but it is particularly efficient at fermenting complex starches in the colon. In laboratory culture, Klebsiella grows faster on starch-rich media than many competing gut organisms. Ebringer's working hypothesis was that a high dietary starch intake feeds Klebsiella preferentially, inflating its population relative to other gut bacteria, which in turn keeps the immune system chronically primed against it.
The logic of the diet, then: if you starve Klebsiella of its preferred substrate, the population drops, the anti-Klebsiella antibody titre drops, the cross-reactive attack on your spine eases off, and symptoms improve. Ebringer measured all three endpoints (dietary starch intake, IgA anti-Klebsiella, BASDAI scores) in uncontrolled cohorts and reported that they moved together.
Critics rightly point out that "starch feeds Klebsiella" is an oversimplification. Most dietary starch is digested in the small intestine and never reaches the colon intact; only resistant starch (found in cooled potato, unripe banana, legumes, whole grains) actually reaches Klebsiella's habitat. Ebringer's diet is still built around cutting total starch, not just resistant starch, so the mechanism may be partly wrong even if the clinical effect is real.
The London AS Diet — Basics
In its simplest form the diet is:
- High in meat, fish, eggs, hard cheese, yogurt, and most vegetables.
- High in low-starch fruit (berries, apples, pears, melon, citrus).
- Very low in bread, pasta, rice, potato, corn, oats, and legumes.
- Unrestricted in fats and oils — olive oil, butter, animal fat are all fine.
There is no calorie counting, no macro-tracking, and no fasting requirement. The rule of thumb is: if it tests positive with iodine (the classic starch stain), cut it. Sugar, honey, and most fruit are allowed because simple sugars are absorbed in the small intestine and do not reach the colon to feed Klebsiella.
That last point surprises many patients: Ebringer's diet is not low-carb in the ketogenic sense. You can eat apples, grapes, berries, and even a modest amount of table sugar. What you cut is specifically complex starch.
What's the Evidence?
This is where honesty matters. The evidence for the London AS Diet is suggestive but not conclusive.
What we have:
- Multiple Ebringer-group cohort studies (1980s through 2000s) reporting that AS patients on a low-starch diet showed reduced ESR, CRP, BASDAI scores, and serum IgA anti-Klebsiella antibody titres over months to years.
- Consistent laboratory evidence that Klebsiella antibodies cross-react with HLA-B27 and collagen peptides.
- Patient-reported outcomes on AS forums — hundreds of self-reported cases of reduced morning stiffness and medication use.
What we don't have:
- A single large, blinded, randomized controlled trial. The Ebringer studies were open-label and mostly uncontrolled; patients who stayed on the diet were compared to those who didn't, with no randomization and no placebo.
- Any endorsement in the ASAS (Assessment of SpondyloArthritis International Society) or ACR (American College of Rheumatology) treatment guidelines. Both groups currently say there is insufficient evidence to recommend any specific diet.
- Mechanistic proof that dropping starch actually shrinks Klebsiella populations in living human colons (stool-microbiome studies on the diet are small and inconsistent).
The fair summary: Ebringer's hypothesis is plausible and intriguing, but not proven. It sits in the "worth trying if you're motivated, doesn't replace real treatment" tier — roughly where Mediterranean-diet recommendations sat 25 years ago before the evidence caught up.
Modern Gut-Microbiome Research
A striking twist: twenty-first-century microbiome research, done with 16S ribosomal RNA sequencing rather than Ebringer's old antibody assays, has independently confirmed that AS patients have a distinctive gut microbiome. Findings that line up (at least loosely) with Ebringer's picture:
- Costello et al. 2015 sequenced terminal ileum biopsies and showed AS patients had significantly different bacterial communities than healthy controls, with increased Lachnospiraceae, Ruminococcaceae, Rikenellaceae, and Porphyromonadaceae.
- HLA-B27 transgenic rats develop spondyloarthropathy only when raised in conventional (microbe-containing) housing — germ-free animals stay healthy. The disease is, at some level, microbially driven.
- Several 2018–2023 stool microbiome studies have found Klebsiella genus increased in AS patients vs controls, though not every study reproduces the finding at the species level.
- Breban et al. 2017 and other French groups have reported a distinct "AS dysbiosis signature" that normalizes somewhat on TNF-inhibitor therapy — suggesting gut bacteria and joint inflammation really are yoked together.
None of this proves the Ebringer story. But it does mean the fundamental idea — that AS is a gut-joint axis disease — has aged better than anyone expected in 1980.
How to Try It Safely
If you want to test the diet on yourself, do it like a clinical trial of one:
- Pick a start date and a 6–8-week window. Shorter trials don't give gut flora time to shift; longer-than-8-week blind trials make it hard to tell diet from seasonal change.
- Record a baseline. Write down your current BASDAI score (you can score yourself online), current morning stiffness duration, current NSAID use, and ideally a recent CRP and ESR from bloodwork.
- Keep a simple food diary. One line per day: what you ate, stiffness on waking (0–10), fatigue (0–10), flares.
- Don't change your medications. Stay on NSAIDs, biologics, DMARDs exactly as prescribed. The diet is additive, not a replacement.
- If you're starting with severe restriction or are already underweight, see a registered dietitian or nutritionist once before starting. Losing too much weight on an AS diet is counterproductive.
- At week 6–8, re-score your BASDAI and re-check CRP/ESR. Compare. If nothing's moved — stop. The diet is cheap but it isn't free, and an 8-week fair test is plenty.
Low-Starch vs Keto vs AIP vs Mediterranean
Patients often conflate these, but they are very different protocols:
- Low-starch (London AS Diet). Cuts complex starch specifically. Allows sugar, fruit, and all animal foods. Rationale: starve Klebsiella. Protein and fat are unrestricted.
- Ketogenic. Cuts all carbohydrate below roughly 30 g/day to force ketone production. Allows fat and protein. Rationale: reduce systemic inflammation via ketones and insulin lowering. Much more restrictive than low-starch — you'd give up most fruit.
- AIP (Autoimmune Protocol). Cuts grains, legumes, dairy, eggs, nightshades, seeds, and alcohol for 30–60 days, then reintroduces. Rationale: identify food triggers. Very restrictive; little direct AS evidence.
- Mediterranean. Emphasizes olive oil, fish, vegetables, legumes, whole grains, moderate wine. Rationale: lower systemic inflammation broadly. Good general rheumatology evidence but allows the starches Ebringer's model wants to cut.
The low-starch diet is by far the least restrictive of the four — if you can give up bread, pasta, potato, and rice, you can keep almost everything else on your plate. That's also why it's easier to sustain for the long run.
Foods to Avoid
- Grains: wheat (bread, pasta, couscous, crackers), rye, barley, oats, rice (white, brown, wild), corn, spelt, millet.
- Starchy tubers: potato, sweet potato, yam, cassava, taro.
- Legumes: beans, lentils, chickpeas, peas (most classical versions of the diet exclude them; some modern versions re-allow lentils in small amounts).
- Unripe bananas and plantains (very high in resistant starch; ripe bananas are far lower).
- Processed foods thickened with cornstarch, tapioca, wheat flour, modified food starch.
- Beer (barley) and most grain-based alcohols.
Foods Allowed Generously
- Protein: beef, lamb, pork, poultry, fish, shellfish, eggs, hard cheeses, cottage cheese, Greek yogurt.
- Non-starchy vegetables: leafy greens, broccoli, cauliflower, cabbage, Brussels sprouts, asparagus, zucchini, bell pepper, tomato, cucumber, mushroom, onion, garlic, carrot (in moderation), beetroot (in moderation).
- Low-starch fruit: berries (strawberry, blueberry, raspberry, blackberry), apples, pears, melon, citrus, grapes, peaches, cherries, ripe bananas (modest portions).
- Fats: olive oil, butter, ghee, avocado, coconut oil, animal fats, nuts and seeds (walnut, almond, pumpkin, sunflower).
- Beverages: water, tea, coffee, wine, spirits (in moderation), milk, kefir.
A Practical Sample Day
- Breakfast. Three-egg omelette with spinach, feta, and tomato. Coffee with milk. A handful of berries.
- Lunch. Grilled salmon over a big mixed-green salad with avocado, cucumber, olives, and olive-oil-lemon dressing. An apple.
- Snack. Greek yogurt with a few walnuts and a drizzle of honey.
- Dinner. Roast chicken thighs with roasted cauliflower, zucchini, and red pepper. A glass of wine if you drink.
- Dessert (optional). Strawberries with a small piece of hard cheese.
Notice there is no bread, rice, pasta, or potato — but the plate looks full, and nobody feels deprived. That's the point. A sustainable AS diet is one you can eat for years, not one you abandon in a month.
Supplements Often Paired
Ebringer did not build a supplement protocol into the diet, but patients and modern integrative rheumatologists commonly add:
- Vitamin D3 — 2000–4000 IU/day to reach a serum 25(OH)D of 40–60 ng/mL. Low vitamin D is associated with higher AS disease activity.
- Omega-3 (EPA+DHA) — 2–3 g/day. Small trials show modest BASDAI improvement.
- Probiotics — specific Lactobacillus strains (L. rhamnosus GG, L. plantarum, L. acidophilus) and Bifidobacterium species have the best track record in spondyloarthritis studies. Broad "shotgun" probiotics are less impressive.
- Curcumin (turmeric extract, 500–1000 mg twice daily with black pepper or phospholipid delivery) — mild anti-inflammatory effect.
- Collagen peptides — anecdotally helpful for enthesitis; evidence is thin but the safety profile is clean.
None of these are substitutes for disease-modifying therapy. They are add-ons.
Signs It's Working
Give the diet 6–8 weeks of strict adherence before deciding. If it is going to help you, you typically see some combination of:
- Morning stiffness dropping from 60–90 minutes toward 15–30 minutes.
- BASDAI falling by at least 20% from baseline (the clinical threshold for a meaningful response).
- Lower CRP and ESR on follow-up bloodwork.
- Fewer "bad days" per week — measured in your food diary.
- Lower NSAID requirement without worse pain.
If none of those move after 8 strict weeks, the diet is probably not your lever. That is useful information too — AS is heterogeneous, and not every patient's disease is driven by the same gut biology.
Limits and Risks
Honesty again:
- It is not a cure. Nobody — not Ebringer, not his patients, not any forum — has reversed established spinal fusion with diet. Best case, you slow disease activity and reduce symptom burden.
- It does not replace biologics or NSAIDs. If your rheumatologist has recommended a TNF or IL-17 inhibitor, the diet is not an alternative — it is a companion. Untreated active AS can fuse your spine. See the biologics guide.
- Nutritional risks. Aggressively low-starch eating can drop fiber intake, cause constipation, and in rare cases shortchange B vitamins if you also cut grains and legumes. Compensate with plenty of non-starchy vegetables, nuts, and seeds.
- Orthorexia risk. Restrictive diets can tip into disordered eating, particularly in patients with a pre-existing anxious relationship with food. If the diet starts to dominate your social life, your mood, or your thinking, step back.
- Not a reason to delay diagnosis or disease-modifying therapy. Some patients spend years "trying the diet first" and arrive in the rheumatologist's office with irreversible fusion. If you already meet AS criteria, pursue real treatment in parallel.
What Researchers Are Watching
The gut-joint axis in AS is one of the hotter areas of rheumatology research right now. Developments worth tracking:
- Fecal microbiota transplantation (FMT) for spondyloarthritis — early-phase trials are ongoing. Results in ulcerative colitis suggest transplanted microbiota can reshape immune phenotype.
- Precision probiotics — specific strains engineered or selected to compete with Klebsiella and similar pathobionts.
- Butyrate and short-chain fatty acid therapies — trying to restore the anti-inflammatory metabolites produced by a healthy gut.
- IL-23 blockade in AS (risankizumab, guselkumab) — whether gut-derived IL-23 is the link between Klebsiella overgrowth and spinal inflammation.
- Large prospective diet trials — the kind of RCT Ebringer never got the funding to run. A few European groups have proposals in the pipeline.
It is entirely possible that within a decade some modernized version of Ebringer's central intuition — feed the right microbes, starve the wrong ones, and AS calms down — will be standard adjunctive care. It is also possible the specific starch-Klebsiella story will be superseded by something more granular. Either way, Ebringer asked the right question forty years early.
Key Research Papers
- Costello ME, et al. Brief report: intestinal dysbiosis in ankylosing spondylitis. Arthritis Rheumatol. 2015;67(3):686–691.
- Breban M, et al. Faecal microbiota study reveals specific dysbiosis in spondyloarthritis. Ann Rheum Dis. 2017;76(9):1614–1622.
- Rashid T, Ebringer A. Ankylosing spondylitis is linked to Klebsiella — the evidence. Clin Rheumatol. 2007;26(6):858–864.
- Ebringer A, Rashid T, Wilson C. Rheumatoid arthritis, Proteus, anti-CCP antibodies and Karl Popper. Autoimmun Rev. 2010 (molecular-mimicry framework paper).
Live PubMed Searches
For further reading, the following PubMed topic searches return peer-reviewed work on the Ebringer hypothesis, the low-starch diet, and the AS gut microbiome:
- Ebringer, Klebsiella, and ankylosing spondylitis
- Low-starch diet and ankylosing spondylitis
- HLA-B27 and the gut microbiome
- Klebsiella pneumoniae and spondylitis
- Molecular mimicry in ankylosing spondylitis
- Gut-joint axis and spondyloarthritis
- Probiotics and ankylosing spondylitis
- Fecal microbiota transplantation in spondyloarthritis
Connections
- Ankylosing Spondylitis
- HLA-B27 Explained
- Biologics Guide
- AS and IBD Overlap
- Exercise and PT Protocol
- NSAID Strategy
- Morning Stiffness Management
- Pregnancy and AS
- Uveitis and Eye Involvement
- Arthritis
- SIBO
- Crohn's Disease
- Ulcerative Colitis
- Inflammatory Bowel Disease
- Klebsiella Pneumoniae
- Probiotics
- Vitamin D3