Elemental Diet for SIBO
The elemental diet is the single most effective intervention for SIBO in trial data — and also the hardest to get through. Two weeks of a liquid-only medical formula, no food, no social meals, no coffee breaks with a pastry. This article covers how it works, whether it’s right for you, what products exist, how to make it yourself, and what the two weeks actually feel like.
Interactive Visualization The Gut Barrier & Your Microbiome Watch fibre become butyrate and butyrate tighten the gut wall — then starve the microbes and see them eat your mucus layer instead. Launch →
Table of Contents
- How the Elemental Diet Works
- The Success Rate — What the Research Shows
- Who the Elemental Diet Is For
- Who It’s NOT For
- Commercial Products — What’s Available
- Homemade Elemental Diet Recipe
- What the Two Weeks Actually Look Like
- Palatability Hacks
- Breaking the Diet Safely (Refeeding)
- Partial and Semi-Elemental Approaches
- Why Relapse Happens After Elemental
- Key Research Papers
- Featured Videos
1. How the Elemental Diet Works
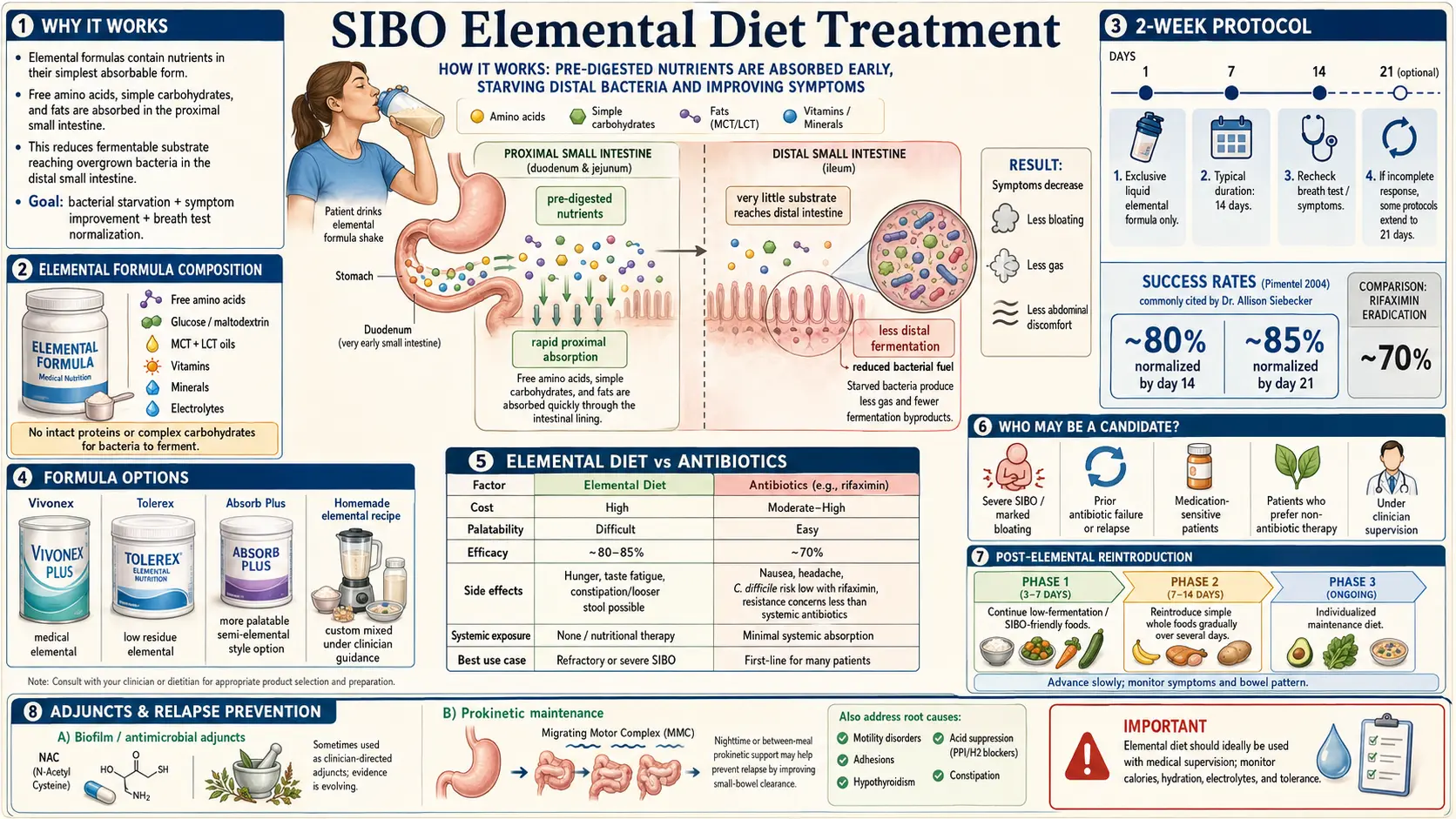
The elemental diet is a medical liquid formula of pre-digested nutrition. Instead of intact protein, it contains free amino acids. Instead of starches and complex carbohydrates, it contains monosaccharides — mostly dextrose (glucose) and maltodextrin. Instead of long-chain fats that require bile salts and pancreatic lipase to break down, it uses primarily medium-chain triglycerides (MCTs), with a small amount of long-chain fat to prevent essential fatty acid deficiency. A full spectrum of vitamins, minerals, and electrolytes rounds it out.
The key is where this mixture gets absorbed. Free amino acids and monosaccharides are absorbed in the proximal jejunum — roughly the first 20 inches of small intestine beyond the stomach. MCTs are absorbed even more proximally, often directly across the intestinal wall into the portal circulation without needing bile. By the time the formula has moved past the first foot or so of small intestine, there is essentially nothing left to feed bacteria. The overgrowth population downstream — in the distal jejunum, ileum, and especially any pockets of stasis — runs out of substrate.
Bacteria do not starve instantly. They consume residual mucus glycoproteins and shed epithelial cells for a few days. But with no dietary carbohydrate, protein, or fiber reaching them, populations collapse over the course of 10–14 days. This is also why the diet must be exclusive: a single piece of toast — a few grams of starch reaching the lower small bowel — resets the clock.
2. The Success Rate — What the Research Shows
The foundational data comes from Pimentel et al. (2004), published in Digestive Diseases and Sciences. In 93 patients with IBS and a positive lactulose breath test, a 14-day exclusive elemental diet normalized the breath test in 80% of patients. Extending to 21 days pushed normalization to 85%. Symptom improvement tracked the breath-test response.
No other single SIBO intervention comes close in published data. Rifaximin at standard dosing normalizes breath tests in roughly 50–65%. Herbal antimicrobials sit in a similar range. For refractory cases — patients who have already failed two or more rounds of rifaximin or herbals — the elemental diet is often the intervention that finally clears the overgrowth.
The catch: the 80–85% figure is in patients who completed the protocol. Completion rates in real-world use are significantly lower, because the diet is genuinely hard to get through. Clinician estimates put real-world completion somewhere between 50% and 75%, depending on support, product chosen, and patient circumstances.
3. Who the Elemental Diet Is For
- Patients who have failed two or more rounds of rifaximin or herbal antimicrobials and still have a positive breath test.
- Methane-dominant SIBO (IMO) that will not respond to rifaximin+neomycin or allicin-based herbal protocols. Methanogens are notoriously stubborn, and substrate starvation often works where antimicrobials don’t.
- Severe cases with documented malabsorption and malnutrition — the formula simultaneously treats the overgrowth and restores nutritional status, because it’s absorbed before bacteria can compete for it.
- Patients who cannot tolerate antibiotics (prior C. difficile, severe drug allergies, significant drug interactions).
- Patients who have made an informed choice to avoid antibiotics for personal or medical reasons.
- Refractory cases being prepared for retesting and rescue protocols — a 2-week elemental reset before a fresh breath test can clarify whether the overgrowth is truly the problem.
4. Who It’s NOT For
- History of anorexia, bulimia, or any eating disorder. Two weeks of liquid-only caloric restriction, constant hunger, rapid weight loss, and obsessive measurement is psychologically dangerous and can trigger relapse of the eating disorder. This is a hard contraindication, not a cautious footnote.
- Diabetes (type 1 or type 2). The formula is mostly monosaccharide carbohydrate — essentially glucose with some amino acids. Blood sugar excursions are severe, insulin dosing becomes extremely difficult, and hypoglycemia between feeds is a real risk. If attempted at all, it requires close endocrinology supervision and continuous glucose monitoring.
- Pregnancy and lactation. Not studied; caloric and micronutrient margins are too thin for fetal development.
- Chronic kidney disease requiring protein restriction. Free amino acid loads are handled differently than whole protein and can stress a compromised kidney.
- Patients without social or home support. Doing this alone — cooking for your family while drinking a chalky beverage, watching everyone eat, handling a full work week at peak hunger on day 4 — is brutal. People who try it solo are the ones who quit on day 5.
- Children and adolescents outside a pediatric GI program.
5. Commercial Products — What’s Available
Four products dominate the market. They differ in cost, palatability, whether they are strictly “elemental” (free amino acids) or “semi-elemental” (partially hydrolyzed protein), and whether they were designed for SIBO or for something else.
| Product | Type | Cost (14 days) | Palatability | Notes |
|---|---|---|---|---|
| Vivonex Plus / T.E.N. (Nestlé) | True elemental (free amino acids) | ~$1,260 (~$15/packet × 6/day) | Widely described as “terrible” | The original medical elemental formula. Cheapest strictly-elemental option. Designed for short-bowel and critical care, repurposed for SIBO. |
| Physicians’ Elemental Diet (Integrative Therapeutics) | True elemental | ~$660 (~$110 × 6 containers) | Better than Vivonex, still chalky | Formulated specifically for SIBO by functional GI practitioners. Available dextrose-free version for candida concerns. |
| Absorb Plus (Imix Nutrition) | Semi-elemental (partially hydrolyzed whey) | ~$400–600 | Most palatable | Not strictly elemental — the protein is hydrolyzed, not broken into free amino acids. Better compliance in practice, slightly lower theoretical efficacy. |
| E028 Splash / Neocate | True elemental (pediatric) | Variable, often insurance-covered for pediatric GI | Flavored, more tolerable | Pediatric formulas used off-label in adults. Lower calorie density means drinking more volume. |
Insurance coverage for adult SIBO is rare. Some functional medicine clinics buy wholesale and pass savings along. Vivonex and Neocate are occasionally covered under medical-food benefits with a prescription and diagnostic codes.
6. Homemade Elemental Diet Recipe
Homemade elemental diets cost a fraction of commercial formulas (~$100–200 for two weeks) but are less validated in trials. Strict interpretation requires free-form amino acid powder, not protein isolate — because even a pure whey isolate is still intact protein that needs enzymatic breakdown. That said, many practitioners use whey protein isolate successfully in practice, especially for the semi-elemental variant.
Ingredients (per day, for a ~70 kg / 154 lb adult)
- Protein: 80–100 g free amino acid powder (or whey protein isolate, NOT concentrate) — split across 6 feeds
- Carbohydrate: 250–300 g dextrose (glucose) powder — this is the bulk of the calories
- Fat: 40–60 g MCT oil, plus 1 tbsp (~14 g) flaxseed or sunflower oil for essential fatty acids
- Multivitamin/mineral: a full-spectrum powdered multi (liquid or crushed-tablet form); avoid gummies, which contain sugar alcohols and gelatin
- Electrolytes: ~3–5 g sodium (sea salt), 2–3 g potassium (potassium chloride salt substitute), 300–400 mg magnesium glycinate
- Water: ~3 liters across all feeds plus between-meal hydration
Daily Macros Target
- Calories: ~1,800–2,200 kcal/day split across 6 feeds (~300–370 kcal each)
- Protein: ~80–100 g (roughly 1.2 g/kg body weight, on the low end to minimize nitrogen load)
- Carbohydrate: ~250–300 g (the dominant fuel source)
- Fat: ~55–75 g (mostly MCT)
Mixing
Blend each feed in a shaker or blender with 10–14 oz cold water. Drink within 15–20 minutes — amino acid solutions taste worse as they warm. Feeds are spaced every 2–3 hours. Do not snack between feeds; water, plain tea, and clear broth are allowed.
Caveat. Homemade protocols have less trial data than commercial elemental formulas. If you’re treating refractory SIBO and you only get one shot at two weeks of your life, a commercial product is more predictable. Homemade makes more sense for repeat protocols, semi-elemental approaches, or people with severe cost constraints.
7. What the Two Weeks Actually Look Like
Honest day-by-day, based on patient reports and clinical observation:
- Days 1–2: Novelty holds you. You feel fine. Hunger is manageable.
- Days 3–4: The worst stretch. Hunger peaks. You are not yet in ketosis, your stored glycogen is depleted, and your body is still expecting real food. Irritability, headaches, and obsessive food thoughts are common. Most people who quit, quit here.
- Day 5: Mild ketosis sets in (despite the carbohydrate load, because total calories are below baseline for most adults). Hunger blunts noticeably.
- Day 7: Energy often stabilizes. Bloating is noticeably down. Many people report their first day of flat abdomen in years.
- Days 8–10: Mental steadiness. Food cravings shift from “I need to eat” to a more detached awareness.
- Days 11–14: Physically easier but psychologically grinding. You want to chew something.
Constipation is common during the protocol — not because of slowed transit, but because with bacterial populations and fiber intake both collapsing, there is genuinely less stool to pass. One bowel movement every 3–4 days is normal. Do not add fiber to “fix” this; it defeats the point.
Social isolation is the underrated cost. No meals with family. No coffee meetings. No work lunches. Plan for this: tell people in advance, choose a low-social two weeks (not the holidays), and don’t schedule anything food-adjacent. Broth, plain tea, plain coffee (if tolerated), and water are allowed between feeds. A cup of warm water with a pinch of salt helps both hydration and the psychological need for “something warm.”
8. Palatability Hacks
- Cold. Chill the formula overnight in the fridge. Cold mutes the amino acid bitterness.
- Fast. Drink in 10–15 minutes, not 45. Do not savor it.
- Straw. A straw bypasses most of your taste buds. This single change is what makes Vivonex tolerable.
- Stevia + vanilla + cinnamon. Pure stevia extract (no erythritol or other sugar alcohols, which ferment), a few drops of vanilla extract, and a shake of cinnamon transform the flavor without adding fermentable substrate.
- Pinch of salt. Counterintuitive, but a small amount of salt blunts bitter amino acids the way it does in cooking.
- Do not mix with milk, juice, or anything creamy. Water only. Any fermentable substrate defeats the protocol.
9. Breaking the Diet Safely (Refeeding)
Do not walk out of day 14 into a pizza. After two weeks without whole food, your bacterial populations are at their lowest point since whenever your SIBO began — and you can re-seed a disordered small-bowel microbiome in 48 hours of bad eating. The first week back is as important as the two weeks you just finished.
- Days 15–17: Bone broth, simple steamed proteins (white fish, poached chicken, eggs), plain white rice, well-cooked zucchini or carrots. Small portions, 4–5 meals spaced 4 hours apart. No raw vegetables, no beans, no dairy yet, no fermented foods, no alcohol.
- Days 18–21: Expand to cooked low-FODMAP vegetables, additional proteins, moderate fat. Still no fiber bombs, no FODMAP triggers, no alcohol.
- Week 2 post-diet: Begin structured low-FODMAP reintroduction to identify personal triggers.
- Week 3 onward: Gradually expand toward a normal, whole-food diet you can actually live on.
Start a prokinetic immediately — day 15 at the latest. This is the single biggest determinant of whether the elemental diet holds. Low-dose naltrexone, prucalopride, low-dose erythromycin, or a structured ginger protocol should be in place before you eat your first real meal. Without prokinetic support, the 44–46% one-year recurrence rate applies just as much to elemental-diet responders as to rifaximin responders. See Prokinetics and Relapse Prevention.
10. Partial and Semi-Elemental Approaches
Not everyone needs — or can do — a full 14-day exclusive protocol. Several modified versions exist:
- Half-elemental. Replace 2 of 3 daily meals with elemental formula and eat one real, low-FODMAP meal per day for 2–4 weeks. Much more sustainable. Reported eradication rates are lower (roughly 50–60%) but still meaningful for moderate cases.
- Rotating protocols. 5 days elemental, 2 days simple real food, repeated for 3–4 weeks. Preserves social life and motivation at the cost of slower bacterial starvation.
- Mini-elemental weekend resets. Friday evening through Sunday evening on elemental formula, repeated once monthly, as a maintenance tool after a full protocol or antibiotic course.
- Semi-elemental (Absorb Plus and similar). Partially hydrolyzed whey protein instead of free amino acids. More palatable, better compliance, slightly less efficacy on paper.
11. Why Relapse Happens After Elemental
The elemental diet clears the overgrowth. It does not fix why the overgrowth happened. If your migrating motor complex (MMC) is impaired — from post-infectious autoimmunity, hypothyroidism, diabetic autonomic neuropathy, chronic opioid use, or structural issues — bacteria will recolonize the small intestine within weeks to months, no matter how clean you got it.
The two interventions that meaningfully reduce post-elemental relapse:
- Prokinetic therapy started the day you refeed and continued for at least 3–6 months. See Prokinetics and Relapse Prevention.
- Treating the root cause. PPIs discontinued where possible, thyroid optimized, glucose controlled, opioids weaned, structural issues evaluated. See Root Causes.
An elemental diet without follow-through is a very expensive, very unpleasant temporary reset.
12. Key Research Papers
Peer-reviewed evidence supporting the elemental diet as a 14- to 21-day intervention for refractory SIBO, plus related work on enteral nutrition and bowel rest. Each citation links to the full text via DOI.
- Pimentel M, Constantino T, Kong Y, Bajwa M, Rezaei A, Park S. A 14-Day Elemental Diet Is Highly Effective in Normalizing the Lactulose Breath Test. Digestive Diseases and Sciences. 2004;49(1):73–77.
- Pimentel M, Saad RJ, Long MD, Rao SSC. ACG Clinical Guideline: Small Intestinal Bacterial Overgrowth. American Journal of Gastroenterology. 2020;115(2):165–178.
- Rezaie A, Buresi M, Lembo A, et al. Hydrogen and Methane-Based Breath Testing in Gastrointestinal Disorders: The North American Consensus. American Journal of Gastroenterology. 2017;112(5):775–784.
- Pimentel M, Chow EJ, Lin HC. Eradication of Small Intestinal Bacterial Overgrowth Reduces Symptoms of Irritable Bowel Syndrome. American Journal of Gastroenterology. 2000;95(12):3503–3506.
- Olendzki BC, Silverstein TD, Persuitte GM, Ma Y, Baldwin KR, Cave D. An Anti-Inflammatory Diet as Treatment for Inflammatory Bowel Disease: A Case Series Report. Nutrition Journal. 2014;13:5.
- O'Morain C, Segal AW, Levi AJ. Elemental Diet as Primary Treatment of Acute Crohn's Disease: A Controlled Trial. British Medical Journal. 1984;288(6434):1859–1862.
- Zoli G, Care M, Parazza M, et al. A Randomized Controlled Study Comparing Elemental Diet and Steroid Treatment in Crohn's Disease. Alimentary Pharmacology & Therapeutics. 1997;11(4):735–740.
- Chedid V, Dhalla S, Clarke JO, et al. Herbal Therapy Is Equivalent to Rifaximin for the Treatment of Small Intestinal Bacterial Overgrowth. Global Advances in Health and Medicine. 2014;3(3):16–24.
- Pimentel M, Park S, Mirocha J, Kane SV, Kong Y. The Effect of a Nonabsorbed Oral Antibiotic (Rifaximin) on the Symptoms of the Irritable Bowel Syndrome: A Randomized Trial. Annals of Internal Medicine. 2006;145(8):557–563.
- Bures J, Cyrany J, Kohoutova D, et al. Small Intestinal Bacterial Overgrowth Syndrome. World Journal of Gastroenterology. 2010;16(24):2978–2990.
- Lauritano EC, Gabrielli M, Scarpellini E, et al. Small Intestinal Bacterial Overgrowth Recurrence after Antibiotic Therapy. American Journal of Gastroenterology. 2008;103(8):2031–2035.
- Quigley EMM. The Spectrum of Small Intestinal Bacterial Overgrowth (SIBO). Current Gastroenterology Reports. 2019;21(1):3.
Live PubMed Searches
Live PubMed queries that update as new papers are indexed.
- PubMed: elemental diet and SIBO
- PubMed: elemental diet and lactulose breath test
- PubMed: elemental nutrition and small bowel
- PubMed: Vivonex and SIBO
- PubMed: semi-elemental diet and bacterial overgrowth
- PubMed: elemental diet for methane / IMO
- PubMed: elemental diet refeeding
- PubMed: elemental diet and IBS
Connections
- The Gut Barrier & Your Microbiome — interactive animation
- SIBO Overview
- Prokinetics and Relapse Prevention
- Root Causes
- Herbal Antimicrobials
- Rifaximin Protocols
- Low-FODMAP Diet
- Hydrogen vs Methane vs Hydrogen Sulfide
- Breath Test Guide
- IMO and Constipation
- Irritable Bowel Syndrome
- Celiac Disease
- Elimination Diet
- Gut Healing
- Probiotics
- Crohn's Disease
- Bloating
- Bone Broth
- IBS and SIBO Overlap