SIBO Root Causes: Why It Keeps Coming Back
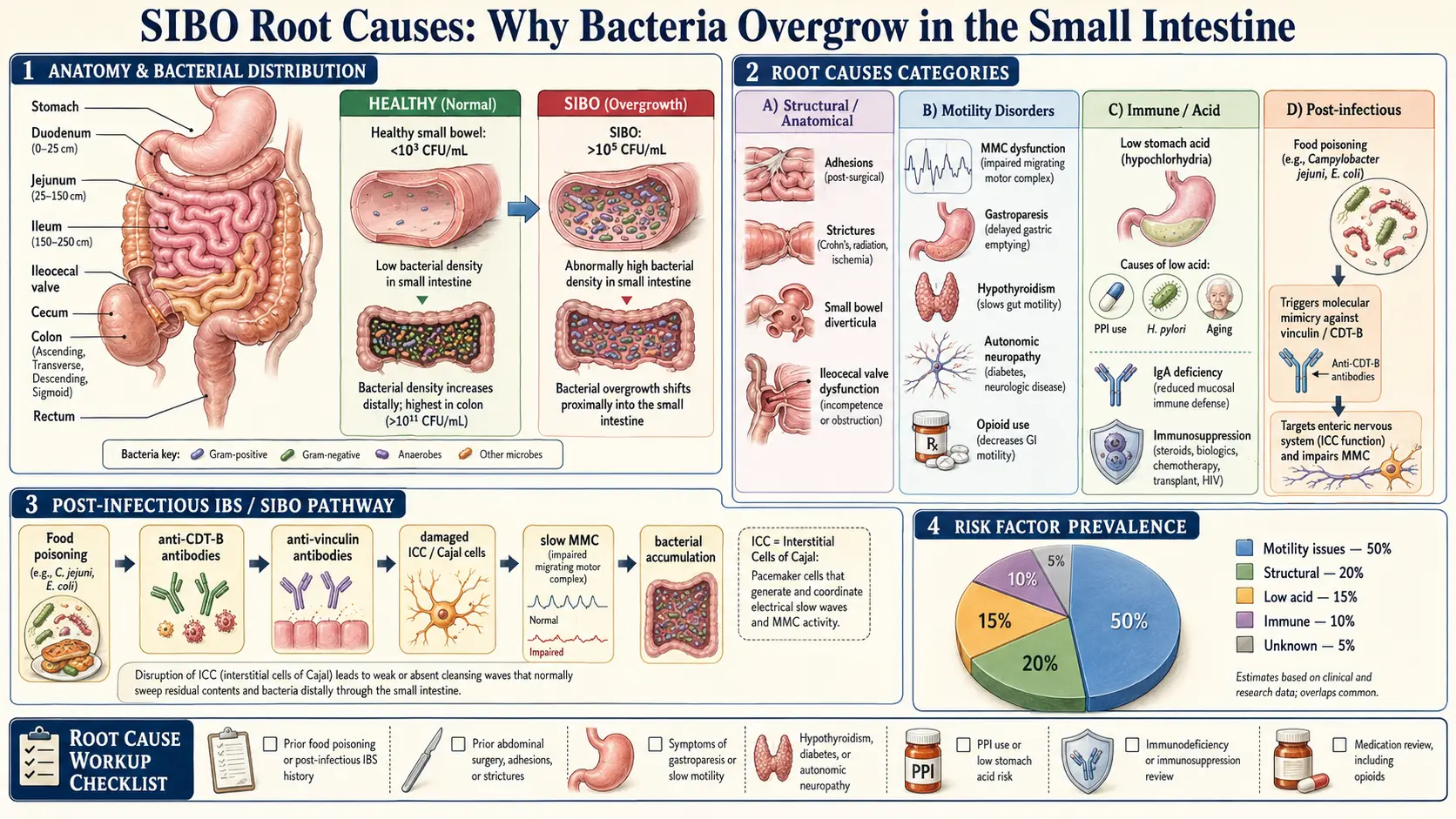
Table of Contents
- Why SIBO Is a Symptom, Not a Diagnosis
- Post-Infectious IBS (by far the most common)
- Ileocecal Valve (ICV) Dysfunction
- Abdominal Adhesions
- Hypothyroidism (including subclinical)
- Chronic PPI Use
- Ehlers-Danlos Syndrome and Hypermobility
- Diabetes and Autonomic Neuropathy
- Scleroderma / Systemic Sclerosis
- Structural Causes (Less Common but Important)
- Stress, Vagus Nerve, and the Brain-Gut Axis
- Food Poisoning History Taking
- The Root-Cause Workup (a practical list)
- Key Research Papers
- Connections
- Featured Videos
1. Why SIBO Is a Symptom, Not a Diagnosis
If you’ve been treated for SIBO three times and it keeps coming back, you’re not broken. Something upstream is broken.
SIBO — small intestinal bacterial overgrowth — is not really a diagnosis. It’s what happens when the body’s defenses against bacteria colonizing the small intestine fail. Finding which defense failed is the actual diagnosis. Everything else is whack-a-mole.
The small intestine is supposed to be nearly sterile. It stays that way because of a stack of overlapping defenses: stomach acid kills incoming bacteria, the migrating motor complex (MMC) sweeps the small bowel clean between meals, the ileocecal valve keeps colonic bacteria from washing backward, bile and pancreatic enzymes are bacteriostatic, and secretory IgA mops up what survives. When one or more of those defenses fails, bacteria move in, ferment your food, and you get the bloating, gas, diarrhea, or constipation that sent you to the doctor.
Here is the part most patients are never told: rifaximin, herbal antimicrobials, and the elemental diet all kill bacteria. None of them restore the defense that failed. This is why 44–46% of patients relapse within 9 to 12 months of a successful eradication. It’s not bad luck and it’s not your fault — it’s the predictable result of killing the bugs without fixing the upstream problem.
This article is a walk through the upstream problems. If you find yours here, you can finally stop cycling antibiotics and start treating the actual disease.
2. Post-Infectious IBS (by far the most common)
This is the single most under-diagnosed cause of chronic, relapsing SIBO. If you can point to a specific gastroenteritis episode — a bad shrimp in Mexico, a chicken sandwich from a gas station, a stomach bug that went through the family — and your gut was never quite the same afterward, you very likely have post-infectious IBS.
The Autoimmune Mechanism
Acute food poisoning from Campylobacter jejuni, Salmonella, Shigella, enterotoxigenic E. coli, or norovirus can trigger a chain reaction that outlasts the infection by years or decades. These bugs produce a toxin called cytolethal distending toxin B (CdtB). Your immune system makes antibodies against CdtB — which is what it’s supposed to do.
The problem is that CdtB is structurally similar to a human intestinal protein called vinculin, which lives in the interstitial cells of Cajal (ICC) — the pacemaker cells of the small intestine. Through a process called molecular mimicry, the anti-CdtB antibodies cross-react and begin attacking vinculin, producing anti-vinculin antibodies that damage your own pacemaker cells.
The result is a permanent slowing of the MMC. The bowel’s “housekeeping wave” becomes weak and infrequent, bacteria are never swept clear, and SIBO becomes the steady state of your gut. You can eradicate the bacteria all day long — the motility defect is still there, so the bacteria come back.
The ibs-smart Test
The ibs-smart blood test (about $250) measures both anti-CdtB and anti-vinculin antibodies. A positive result carries a positive predictive value greater than 95% for post-infectious IBS. If you test positive, the implication is enormous: your root cause is autoimmune damage to the MMC, and the long-term strategy is not more antibiotics but permanent prokinetic support (low-dose naltrexone, prucalopride, low-dose erythromycin, ginger) to compensate for the pacemaker damage. See Prokinetics and Relapse Prevention for the specific agents and protocols.
This diagnosis alone — knowing that your SIBO is autoimmune, not a character flaw or a dietary sin — is often a watershed moment for patients. It reframes the illness from “I keep failing treatment” to “I have a chronic autoimmune condition that requires ongoing management.”
3. Ileocecal Valve (ICV) Dysfunction
The ileocecal valve is a one-way sphincter between the end of the small intestine (terminal ileum) and the start of the colon (cecum). It exists specifically to prevent the dense colonic bacterial population — on the order of 1011 to 1012 organisms per gram of stool — from backflowing into the small bowel, which is supposed to be a thousand times less populated.
When the ICV stays open, flaps incompetently, or has been surgically removed, colonic bacteria wash backward and recolonize the distal ileum. You eradicate them, and within weeks they seep back in from the other side.
Common Causes of ICV Dysfunction
- Prior abdominal surgery, especially appendectomy (the appendix sits right next to the ICV, and surgical scarring can tether or distort the valve)
- Chronic constipation (sustained colonic distension stretches the valve open)
- Crohn’s disease of the terminal ileum (inflammation and scarring directly destroy the valve)
- Pelvic floor dysfunction and chronic straining
- Post-infectious scarring after severe gastroenteritis or C. difficile colitis
Treatment
Osteopathic / visceral manipulation by a trained osteopath or physical therapist is the most common non-surgical approach. Many functional practitioners also teach patients the “Gut Bug Massage” — a gentle self-massage over the lower right abdomen (where the ICV sits, roughly halfway between your belly button and your right hip bone) performed before meals to encourage the valve to close. Surgical correction of a failing ICV is rare and reserved as a last resort, because abdominal surgery creates new adhesions that can create their own motility problems.
4. Abdominal Adhesions
Every time the abdomen is opened — C-section, appendectomy, endometriosis excision, hernia repair, gallbladder removal — the body lays down scar tissue (adhesions) as it heals. These bands of fibrous tissue can physically tether loops of small intestine to each other, to the abdominal wall, or to pelvic organs. Pelvic inflammatory disease and endometriosis create their own adhesion patterns without any surgery at all.
Adhesions don’t just cause pain. They create mechanical bottlenecks: narrow passages where intestinal contents slow down, bacteria accumulate, and the MMC’s sweeping contractions can’t fully clear the segment. It’s a plumbing problem, not a microbiome problem.
How to Diagnose
- MR enterography or CT enterography: can show kinking, tethering, or focal dilation upstream of a narrowed segment
- Upper GI series with small bowel follow-through: shows delayed transit and abnormal loop positions in real time
- Visceral osteopathic exam: a trained clinician can often feel restricted mobility of bowel loops through the abdominal wall
Treatment Options
Visceral manipulation (the Wurn Technique / Clear Passage protocol) is a manual therapy specifically developed for post-surgical and endometriosis-related adhesions, with published data on improved motility and reduced obstructive symptoms. Pelvic floor physical therapy helps where pelvic adhesions are involved. Adhesiolysis surgery — cutting the adhesions — is a blunt tool: it creates new adhesions as it heals, and the cost-benefit has to be weighed carefully. It’s usually reserved for patients with documented partial obstruction or severe pain.
5. Hypothyroidism (including subclinical)
This one is enormous and routinely missed. Studies show that 54% of hypothyroid patients have SIBO. Thyroid hormone — specifically active T3 — powers intestinal smooth muscle contraction. When T3 is low, peristalsis slows, the MMC weakens, and bacteria accumulate.
The Full Thyroid Panel
A TSH alone is not enough. You need: TSH, Free T3, Free T4, reverse T3, TPO antibodies, and thyroglobulin (TG) antibodies. Reverse T3 (a metabolically inactive form) rises during stress and illness and can blunt T3’s effects even when T4 looks fine. TPO and TG antibodies identify Hashimoto’s thyroiditis, which can produce symptoms years before TSH crosses the diagnostic threshold.
The “Subclinical” Trap
Standard lab reference ranges label a TSH of 4.5 as normal. Many thyroid specialists consider a TSH above 2.5 suboptimal, especially when paired with symptoms — fatigue, cold intolerance, hair thinning, constipation, weight gain, and (of course) bloating and relapsing SIBO. If your TSH is 3.8 and your doctor says you’re fine but your SIBO won’t stop, get a second opinion. See Thyroid Disorders for a full workup guide.
6. Chronic PPI Use (Omeprazole, Pantoprazole, etc.)
Proton pump inhibitors — omeprazole (Prilosec), pantoprazole (Protonix), esomeprazole (Nexium), lansoprazole (Prevacid) — raise gastric pH above 4 and effectively eliminate the acid barrier that kills swallowed bacteria. They were designed for 4 to 8 weeks of use. Millions of patients have been on them for 10 or 20 years.
Chronic PPI use doubles to quadruples SIBO risk. Up to 50% of chronic PPI users have measurable SIBO. Without a working acid barrier, every mouthful of salad or sip of tap water seeds the small intestine with organisms that healthy stomach acid would have killed in seconds.
How to Come Off PPIs Safely
You can’t just stop. Abrupt PPI discontinuation causes rebound acid hypersecretion for 2 to 8 weeks — even in people who never had real reflux to begin with — and patients almost always conclude they “need” the drug and go back on it. A sane taper looks like this:
- Taper over 4 to 8 weeks: halve the dose, then every-other-day, then stop
- Swap to an H2 blocker for the transition: famotidine 20–40 mg at bedtime covers nocturnal acid without the microbiome effects of a PPI
- Use temporary coating agents for breakthrough symptoms: Gaviscon (sodium alginate) after meals, sucralfate 1 g before meals
- Fix the upstream cause: hiatal hernia, H. pylori infection, food triggers (coffee, alcohol, chocolate, spicy, fatty), late-night eating, obesity, tight waistbands
Most patients on chronic PPIs never needed them in the first place — and if they did, the underlying driver was never addressed.
7. Ehlers-Danlos Syndrome and Hypermobility Spectrum
If you’re unusually flexible, bruise easily, get lightheaded when you stand up, and have a gut that just won’t behave — this cluster deserves a serious look. Hypermobile Ehlers-Danlos Syndrome (hEDS) and the broader Hypermobility Spectrum Disorder (HSD) are connective tissue disorders in which collagen is structurally fragile. That fragility affects the smooth muscle and fascia of the gut just as much as it affects joints.
A loose, overly compliant intestinal wall doesn’t contract cleanly. Motility patterns become disorganized, the MMC loses amplitude, and bacteria set up shop. Many hEDS patients develop gastroparesis, chronic constipation, and chronic relapsing SIBO.
The Triad
hEDS comes with a well-recognized triad:
- hEDS / HSD — joint hypermobility, soft stretchy skin, poor wound healing
- POTS (Postural Orthostatic Tachycardia Syndrome) — dizziness and racing heart on standing, driven by autonomic dysfunction and vascular compliance problems
- MCAS (Mast Cell Activation Syndrome) — food reactions, flushing, hives, unexplained allergic-style symptoms
If you’re flexible and dizzy and bloated, you may well have this cluster. Get a Beighton score assessment (a 9-point test of joint hypermobility; 5 or more in adults is suggestive), and ask for a referral to a geneticist or an EDS-literate rheumatologist for formal hEDS classification.
8. Diabetes and Autonomic Neuropathy
Between 8% and 44% of diabetics have SIBO, with the higher numbers in long-standing or poorly controlled disease. The mechanism is diabetic autonomic neuropathy: chronic hyperglycemia damages the small, unmyelinated autonomic nerves that control the MMC and gastric emptying. The result is gastroparesis upstream and SIBO downstream.
Treatment is twofold: tight glycemic control (HbA1c ideally below 7.0 for motility preservation, lower for the youngest patients) and prokinetics to compensate for the nerve damage. Once the nerves are dead they don’t come back, so the strategy is prevention in early diabetes and chronic prokinetic support in established autonomic neuropathy.
9. Scleroderma / Systemic Sclerosis
SIBO prevalence in systemic sclerosis runs 43% to 55% — among the highest of any medical condition. The underlying mechanism is direct: the autoimmune fibrosis that thickens scleroderma patients’ skin also fibroses the smooth muscle of the esophagus, stomach, and small intestine. Muscle that’s been replaced by scar tissue doesn’t contract. The MMC fails and bacteria overgrow.
Scleroderma-associated SIBO is generally not curable in the usual sense. The long-term plan is cycling rifaximin — typically a 2-week course once a month, or alternating rifaximin and herbal antimicrobials month to month — combined with a prokinetic and dietary management. The goal shifts from eradication to symptom control.
10. Structural Causes (Less Common but Important)
A minority of patients have a physical abnormality that creates a bacterial hideout antibiotics can’t reach.
- Small intestinal diverticulosis — outpouchings in the jejunum or ileum where bacteria nest and re-seed the lumen. Visible on small-bowel imaging.
- Surgical blind loops — after Billroth II gastrectomy or Roux-en-Y gastric bypass, a defunctionalized loop of bowel receives no digestive flow and becomes a bacterial reservoir.
- Strictures — from Crohn’s disease, chronic NSAID use, or radiation enteritis. Contents dam up behind the narrowing and bacteria proliferate.
- Intestinal malrotation — a congenital anomaly where the bowel didn’t rotate normally in utero. Often caught in childhood, but mild cases can present in adulthood as chronic SIBO with odd loop positions on imaging.
If you have a surgical history, significant Crohn’s disease, or breath-test findings that don’t match a straightforward small-bowel pattern, imaging (MR enterography is the workhorse) is warranted.
11. Stress, Vagus Nerve, and the Brain-Gut Axis
This is the cause people roll their eyes at — and then it turns out to be their answer. Chronic sympathetic (“fight-or-flight”) overdrive directly inhibits the MMC via vagal withdrawal. The vagus nerve is the primary parasympathetic driver of gut motility; when it’s chronically suppressed by stress, trauma, or anxiety, the MMC never fires cleanly.
This is not airy-fairy. It’s well-documented in the motility literature. Patients with histories of severe stress, PTSD, eating disorders, or prolonged illness frequently have measurably weakened MMCs that don’t normalize until the vagal tone is rebuilt. Techniques with actual evidence include slow diaphragmatic breathing, cold-water face immersion, humming and gargling (stimulate the vagus via the pharyngeal branches), and specific gut-directed hypnotherapy programs such as Nerva. See Prokinetics and Relapse Prevention for the specific vagal-tone protocols.
12. Food Poisoning History Taking
If there is one question every SIBO patient should be asked, it is: “Did any of this start after you got food poisoning?”
Most GI visits skip it. The classic post-infectious pattern looks like this:
- A specific gastroenteritis episode — often travel-related (“Delhi belly,” cruise ship norovirus), shellfish, raw chicken, undercooked eggs, contaminated produce
- The acute illness resolves in 3 to 7 days
- For 3 to 6 months afterward, the patient has “IBS-like” symptoms that are usually dismissed as post-viral
- Those symptoms never fully resolve, and over the following year the picture evolves into frank, relapsing SIBO
Document the timeline. Write it down, with approximate dates. This history plus a positive ibs-smart test essentially confirms post-infectious SIBO, and the long-term treatment plan pivots from repeated antimicrobials to chronic prokinetics plus low-dose naltrexone (LDN). That’s a completely different disease trajectory than “another round of rifaximin.”
13. The Root-Cause Workup (a practical list)
Bring this list to your next appointment. If your clinician isn’t ordering most of these and you’re on your third relapse, you need a different clinician.
- Trio-smart breath test — establishes the gas subtype (hydrogen, methane, hydrogen sulfide) and baseline severity
- ibs-smart antibodies — anti-vinculin + anti-CdtB, to identify post-infectious autoimmune SIBO
- Full thyroid panel — TSH, Free T3, Free T4, reverse T3, TPO, TG antibodies
- HbA1c and fasting insulin — identifies diabetes, pre-diabetes, and insulin resistance
- Comprehensive metabolic panel + celiac panel (tTG-IgA with total IgA) — rules out celiac, liver disease, kidney disease
- Beighton hypermobility score — a 2-minute bedside screen for hEDS / HSD
- MR enterography — if adhesions, strictures, diverticula, or Crohn’s are suspected
- Comprehensive stool test (GI-MAP, GI Effects, or equivalent) — screens for dysbiosis, pathogens, pancreatic elastase, calprotectin
- Medication review — PPIs, opioids, anticholinergics, GLP-1 agonists, tricyclic antidepressants (all slow motility)
14. Key Research Papers
Peer-reviewed literature on the underlying drivers of SIBO — post-infectious autoimmunity, motility disorders, structural anomalies, connective-tissue disease, and medication-related risk. Each citation links to the full text via DOI.
- Pimentel M, Morales W, Pokkunuri V, et al. Autoimmunity Links Vinculin to the Pathophysiology of Chronic Functional Bowel Changes Following Campylobacter jejuni Infection in a Rat Model. Digestive Diseases and Sciences. 2015;60(5):1195–1205.
- Pimentel M, Saad RJ, Long MD, Rao SSC. ACG Clinical Guideline: Small Intestinal Bacterial Overgrowth. American Journal of Gastroenterology. 2020;115(2):165–178.
- Bures J, Cyrany J, Kohoutova D, et al. Small Intestinal Bacterial Overgrowth Syndrome. World Journal of Gastroenterology. 2010;16(24):2978–2990.
- Pimentel M, Soffer EE, Chow EJ, Kong Y, Lin HC. Lower Frequency of MMC Is Found in IBS Subjects with Abnormal Lactulose Breath Test, Suggesting Bacterial Overgrowth. Digestive Diseases and Sciences. 2002;47(12):2639–2643.
- Lin HC. Small Intestinal Bacterial Overgrowth: A Framework for Understanding Irritable Bowel Syndrome. JAMA. 2004;292(7):852–858.
- Marie I, Ducrotté P, Denis P, Menard JF, Levesque H. Small Intestinal Bacterial Overgrowth in Systemic Sclerosis. Rheumatology. 2009;48(10):1314–1319.
- Lo WK, Chan WW. Proton Pump Inhibitor Use and the Risk of Small Intestinal Bacterial Overgrowth: A Meta-Analysis. Clinical Gastroenterology and Hepatology. 2013;11(5):483–490.
- Lauritano EC, Bilotta AL, Gabrielli M, et al. Association between Hypothyroidism and Small Intestinal Bacterial Overgrowth. Journal of Clinical Endocrinology & Metabolism. 2007;92(11):4180–4184.
- Reddymasu SC, McCallum RW. Small Intestinal Bacterial Overgrowth in Gastroparesis: Are There Any Predictors? Journal of Clinical Gastroenterology. 2010;44(1):e8–e13.
- Cuoco L, Salvagnini M. Small Intestine Bacterial Overgrowth in Irritable Bowel Syndrome: A Retrospective Study with Rifaximin. Minerva Gastroenterologica e Dietologica. 2006;52(1):89–95.
- Rao SSC, Bhagatwala J. Small Intestinal Bacterial Overgrowth: Clinical Features and Therapeutic Management. Clinical and Translational Gastroenterology. 2019;10(10):e00078.
- Pimentel M, Wallace D, Hallegua D, et al. A Link between Irritable Bowel Syndrome and Fibromyalgia May Be Related to Findings on Lactulose Breath Testing. Annals of the Rheumatic Diseases. 2004;63(4):450–452.
- Roland BC, Ciarleglio MM, Clarke JO, et al. Small Intestinal Transit Time Is Delayed in Small Intestinal Bacterial Overgrowth. Journal of Clinical Gastroenterology. 2015;49(7):571–576.
Live PubMed Searches
Live PubMed queries that update as new papers are indexed.
- PubMed: post-infectious IBS and vinculin
- PubMed: ileocecal valve and SIBO
- PubMed: abdominal adhesions and obstruction
- PubMed: SIBO and hypothyroidism
- PubMed: SIBO and proton pump inhibitors
- PubMed: Ehlers-Danlos and GI disease
- PubMed: SIBO in scleroderma / systemic sclerosis
- PubMed: diabetic autonomic neuropathy and the gut
- PubMed: vagus nerve and gut motility
Connections
- The Gut Barrier & Your Microbiome — interactive animation
- SIBO Overview
- Prokinetics and Relapse Prevention
- Herbal Antimicrobials
- Elemental Diet
- Rifaximin Protocols
- Low-FODMAP Diet
- Hydrogen vs Methane vs Hydrogen Sulfide
- Breath Test Guide
- POTS
- MCAS
- Thyroid Disorders
- Diabetes
- Irritable Bowel Syndrome
- Celiac Disease
- Crohn's Disease
- Alpha-Gal Syndrome
- Gut Healing
- Ehlers-Danlos Syndrome