Herbal Antimicrobials for SIBO
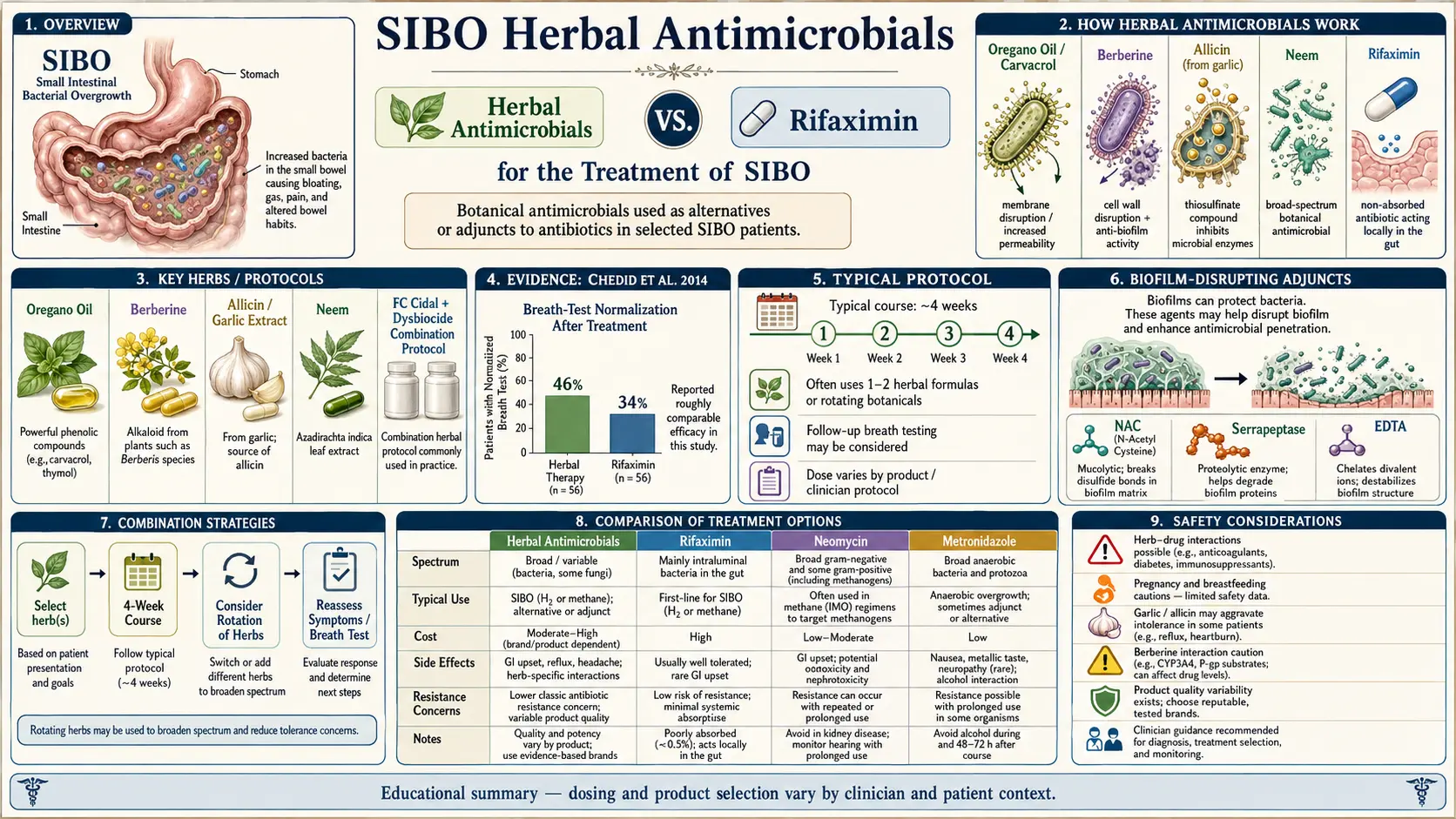
Table of Contents
- The Chedid Study — Why This Isn’t Hand-Waving
- How Herbal Antimicrobials Work
- The Core Herbs — Detailed Dosing
- The Two Branded Protocols (Used in the Chedid Study)
- Sample Combination Protocols
- Why 4 Weeks (vs. 2 Weeks for Rifaximin)
- Herxheimer (Die-Off) Reactions
- Rotation Protocols for Relapse
- Who Should Skip Herbal Protocols
- Herbs + Rifaximin Combined?
- Cost Comparison
- What to Pair Herbs With
- Key Research Papers
- Research Papers (PubMed)
- Connections
- Featured Videos
1. The Chedid Study — Why This Isn’t Hand-Waving
For years, herbal antimicrobials for SIBO were treated as an alternative-medicine sideshow — something naturopaths did while real doctors prescribed rifaximin. That changed in 2014, when Victor Chedid and colleagues at the Johns Hopkins Division of Gastroenterology and Hepatology published a retrospective study in Global Advances in Health and Medicine that nobody in the SIBO world could ignore.
The design was simple: 104 SIBO patients, all with positive lactulose breath tests, divided between two treatment arms. One group received standard rifaximin (1,200 mg/day for 10 days). The other received a 4-week course of herbal antimicrobials (either Dysbiocide + FC Cidal or Candibactin-AR + Candibactin-BR). Everyone was re-tested after treatment.
The results:
- Herbal protocols: 46% eradication (normalization of lactulose breath test)
- Rifaximin: 34% eradication in the same patient population
The difference wasn’t statistically significant — the study was underpowered for that — but the point landed hard: herbs were at least as effective as the pharmaceutical gold standard, and trended better. In the rifaximin non-responder subgroup, herbs then rescued 57% of patients who had failed the drug. That changed the conversation. Today, most integrative GI practitioners and a growing number of conventional gastroenterologists consider herbal protocols a legitimate first-line or second-line option, not a last resort.
2. How Herbal Antimicrobials Work
Pharmaceutical antibiotics are generally single-molecule agents hitting a single bacterial target — rifaximin blocks RNA polymerase, metronidazole damages DNA, neomycin disrupts ribosomes. Clean, potent, and easy for bacteria to develop resistance to if the target mutates.
Herbal antimicrobials work differently. Each plant extract is a complex mixture of dozens of phytochemicals — volatile oils (carvacrol, thymol), alkaloids (berberine, sanguinarine), organosulfur compounds (allicin, diallyl sulfides), flavonoids, tannins, and saponins — all hitting multiple bacterial targets simultaneously. Mechanisms documented in the literature include:
- Membrane disruption — phenolics like carvacrol insert into bacterial lipid bilayers and leak cytoplasmic contents
- Quorum sensing interference — several herbs block the cell-to-cell signaling bacteria use to coordinate virulence
- Biofilm penetration — volatile oils dissolve the polysaccharide matrix protecting established bacterial colonies
- Direct bactericidal activity — berberine and allicin kill on contact rather than merely suppressing growth
- Efflux pump inhibition — some plant alkaloids disable the pumps bacteria use to expel antibiotics
Because each herb acts on several fronts at once, resistance is theoretically harder to develop — a single mutation can’t defeat all mechanisms at the same time. There is no documented widespread resistance to oregano oil or berberine in the way we see resistance to ciprofloxacin or amoxicillin.
3. The Core Herbs — Detailed Dosing
Allicin (Stabilized Garlic Extract)
Dose: 180–450 mg twice to three times daily, taken with meals. Allicin is the pungent organosulfur compound generated when garlic (Allium sativum) is crushed. Raw garlic produces allicin, but it’s digested before it reaches the small intestine, so for SIBO you need enteric-coated or chemically stabilized forms only. Garlic powder supplements from the grocery store are useless here.
Allicin’s killer feature: it is one of the very few natural compounds with documented anti-archaeal activity against Methanobrevibacter smithii, the methanogen that drives methane-dominant SIBO (IMO) and the constipation that comes with it. That makes allicin the go-to for methane. Products with clinical-grade allicin content: Allimax Pro, Allimed (each capsule standardized for allicin output).
Berberine
Dose: 500 mg three times daily (typically as berberine HCl). Berberine is a yellow alkaloid extracted from Hydrastis canadensis (goldenseal), Mahonia aquifolium (Oregon grape root), Berberis vulgaris (barberry), and Phellodendron amurense. Broad-spectrum against both Gram-negative and Gram-positive bacteria.
Bonus effects most herbs don’t offer: berberine is mildly prokinetic (helps the migrating motor complex — which matters for preventing relapse), anti-inflammatory, and clinically proven to lower blood glucose and LDL cholesterol. If you have metabolic syndrome or prediabetes alongside SIBO, this is a two-birds herb. Products: Integrative Therapeutics Berberine, Thorne Berberine-500, Designs for Health Berberine Synergy.
Oregano Oil
Dose: 200–600 mg daily, standardized to 60–75% carvacrol. Oregano oil (Origanum vulgare) contains the phenolic monoterpenoids carvacrol and thymol, which are the active antimicrobials. Broad-spectrum against Gram-negative, Gram-positive, and some fungi.
For SIBO, use enteric-coated capsules so the oil is delivered past the stomach into the small intestine where you need it. Raw oil drops burn the esophagus and largely release their payload too early. Quality brands: ADP (Biotics Research), Oregano Plus (Designs for Health), Thorne Oregano Oil. MLM oregano oils (Young Living, doTERRA) have highly variable carvacrol content and are not recommended for clinical dosing.
Neem
Dose: 300 mg three times daily. Neem (Azadirachta indica) is a cornerstone Ayurvedic antimicrobial with particular strength against Gram-negative bacteria and parasites. Often combined with berberine in protocols targeting mixed overgrowth or suspected protozoal co-infection. Products: Himalaya Neem, Solaray Neem, Banyan Botanicals Neem.
Supporting Players
Several other herbs rotate through combination formulas but rarely anchor a protocol alone:
- Uva ursi (Arctostaphylos uva-ursi) — urinary and GI antimicrobial via arbutin
- Goldenseal (Hydrastis canadensis) — berberine source, also contains hydrastine
- Olive leaf extract — oleuropein, mild broad-spectrum
- Wormwood (Artemisia absinthium) — artemisinin-class compounds, antiparasitic
- Black walnut hull (Juglans nigra) — juglone, antimicrobial and antiparasitic
- Thyme oil (Thymus vulgaris) — thymol, close cousin to oregano
4. The Two Branded Protocols (Used in the Chedid Study)
Biotics Research: FC Cidal + Dysbiocide
Chedid’s first herbal arm. Dose: 2 capsules of each, twice daily, for 4 weeks.
- FC Cidal — Indian tinospora (Tinospora cordifolia), horsetail, coptis, thyme, Achillea millefolium (yarrow)
- Dysbiocide — sage, celandine, yarrow, ginger, stemona, Indian tinospora
Metagenics: Candibactin-AR + Candibactin-BR
Chedid’s second herbal arm. Dose: 2 capsules of each, twice daily, for 4 weeks.
- Candibactin-AR — emulsified thyme oil, oregano oil, sage oil, lemon balm
- Candibactin-BR — berberine HCl, Oregon grape, coptis, Chinese goldthread, ginger, licorice
Both branded kits were used in the Chedid trial, so if you want to follow the evidence literally, one of these two combinations is the most defensible starting point.
5. Sample Combination Protocols (Practical)
- Hydrogen-dominant SIBO: Berberine 500 mg TID + Oregano oil 200 mg BID × 4 weeks
- Methane-dominant SIBO (IMO): Allicin (Allimed) 450 mg TID + Oregano 200 mg BID × 4 weeks
- Mixed or refractory: Candibactin-AR + Candibactin-BR at label dose × 4 weeks, then reassess
- Hydrogen sulfide subtype: Bismuth subsalicylate 2 caplets QID + Oregano 200 mg BID × 4 weeks (emerging protocol, limited evidence but clinically reasonable)
Dose-limiting factor in most protocols is GI tolerance, not toxicity. Start at half the target dose for 2–3 days and titrate up if tolerated.
6. Why 4 Weeks (vs. 2 Weeks for Rifaximin)
Rifaximin is run for 14 days. Herbal protocols run for 28 days. Three reasons:
- Gentler kill curve. Herbal phytochemicals generally have lower peak antimicrobial activity per dose than a concentrated pharmaceutical, so they need more time to clear the population.
- Plasma pharmacokinetics matter less here. SIBO treatment is about luminal concentration, not blood levels. What matters is sustained delivery to the small-bowel lumen over many bacterial division cycles.
- Combination herbs cycle through reproductive phases. Different herbs hit bacteria at different stages (biofilm, planktonic, dormant). Four weeks gives the combination time to catch cells as they become vulnerable.
Shortening a herbal protocol to 2 weeks to mimic rifaximin timing is a common mistake and a common reason people report herbal protocols “didn’t work.” The Chedid protocol is 4 weeks. Stick with 4 weeks.
7. Herxheimer (Die-Off) Reactions
When bacteria die en masse, they release lipopolysaccharide (LPS) and other endotoxins into the gut lumen. Some of that leaks systemically and triggers immune activation. The result, in the first 3–7 days of any effective antimicrobial protocol — pharmaceutical or herbal — is:
- Flu-like fatigue
- Headache
- Brain fog
- Temporarily worsened bloating, gas, and bowel symptoms
- Mild body aches, night sweats
This is Herxheimer reaction, originally described for syphilis treatment in 1895 and now recognized across antimicrobial therapies. It typically peaks at day 3–5 and resolves by day 7–10.
Mitigation: binders like activated charcoal, zeolite, or chlorella can mop up endotoxins in the gut lumen — take them at least 2 hours away from herbs (binders will also adsorb your antimicrobials if dosed together). Drink more water. If symptoms are severe or functionally disabling, reduce the dose by 50% for 3 days and then titrate back up. Don’t abandon the protocol unless symptoms are truly intolerable — die-off is a sign it’s working.
8. Rotation Protocols for Relapse
SIBO recurrence after successful treatment is common — around 44% at 9–12 months with any modality. If it comes back, don’t just repeat the same herbs: rotate. A sensible rotation across cycles:
- Round 1: Berberine + oregano oil
- Round 2: Allicin + oregano (or add neem)
- Round 3: Candibactin-AR + Candibactin-BR (or FC Cidal + Dysbiocide)
The logic is the same as antibiotic stewardship: varying the selective pressure each round makes it harder for surviving bacterial populations to adapt habitually to a single agent. Between rounds, double down on root-cause work and prokinetic therapy — killing the bugs again without fixing the underlying motility problem is the definition of Sisyphean.
9. Who Should Skip Herbal Protocols
Herbals are not universally safer than pharmaceuticals. These are genuine contraindications:
- Severe malabsorption or significant weight loss. If you’re losing weight fast and nutritionally compromised, herbs’ slower kill curve is a luxury you can’t afford. Rifaximin or the elemental diet is more appropriate — faster knockdown so absorption can recover.
- Pregnancy. Berberine, wormwood, black walnut, goldenseal, and several others are contraindicated. Treatment should be deferred or managed by an obstetric specialist.
- Complex drug interactions. Berberine interacts with statins, warfarin, metformin, and cyclosporine. Goldenseal and berberine both inhibit CYP3A4, affecting dozens of drugs. If you’re on multiple prescriptions, review with a pharmacist before starting.
- Severe liver disease. Several herbs (wormwood, goldenseal, kava in some formulas) are hepatically metabolized and can stress a compromised liver.
- Children under 12. Dosing and safety data are extrapolated and uncertain.
- Known allergies. Mint-family allergies (oregano, thyme, sage) and sulfur sensitivity (allicin) are real.
10. Herbs + Rifaximin Combined?
Some integrative gastroenterologists combine pharmaceutical and herbal therapy for severe refractory SIBO: rifaximin for the standard 14 days, with herbs overlapping from week 2 through week 6. The theory is that rifaximin front-loads the kill and herbs finish off rifaximin-tolerant subpopulations and penetrate biofilms.
There are no randomized trial data on this approach yet. Anecdotally, practitioners report it works for patients who failed rifaximin alone and failed herbs alone. It is not a first-line strategy — save it for the refractory cases.
11. Cost Comparison
This is the elephant in the exam room for many patients:
- Herbal 4-week course: approximately $120–250 out of pocket, depending on brand and whether a branded kit (Candibactin, FC Cidal/Dysbiocide) or individual bulk herbs are used.
- Rifaximin (Xifaxan) 14-day course: approximately $1,800–2,500 cash price. Insurance coverage is highly variable — many plans require prior authorization and still deny. Patient assistance programs from Salix help some but not all.
For patients without insurance, with high-deductible plans, or whose insurer refuses coverage, the math isn’t close. That is why a huge fraction of real-world SIBO treatment now starts with herbs — not because they’re philosophically preferred, but because they’re an order of magnitude cheaper with similar efficacy.
12. What to Pair Herbs With
Killing the bacteria is one step in a three-step job. Without the other two, you’ll be back in six months.
- Prokinetic therapy after the 4-week kill phase to restore MMC activity and prevent relapse — see Prokinetics & Relapse Prevention.
- Low-FODMAP eating during treatment to reduce fermentable substrate and symptom intensity — see Low-FODMAP Diet. Reintroduce FODMAPs after treatment; long-term restriction starves beneficial commensals.
- Root-cause work — hypothyroidism, adhesions, ileocecal valve dysfunction, post-infectious antibodies, PPIs, opioid motility suppression — see Root Causes.
13. Key Research Papers
- Chedid V, Dhalla S, Clarke JO, et al. Herbal therapy is equivalent to rifaximin for the treatment of small intestinal bacterial overgrowth. Global Advances in Health and Medicine. 2014;3(3):16–24.
- Pimentel M, Saad RJ, Long MD, Rao SSC. ACG Clinical Guideline: Small Intestinal Bacterial Overgrowth. American Journal of Gastroenterology. 2020;115(2):165–178.
- Logan AC, Beaulne TM. The treatment of small intestinal bacterial overgrowth with enteric-coated peppermint oil: a case report. Alternative Medicine Review. 2002;7(5):410–417.
- Chen C, Tao C, Liu Z, et al. A randomized clinical trial of berberine hydrochloride in patients with diarrhea-predominant irritable bowel syndrome. Phytotherapy Research. 2015;29(11):1822–1827.
14. Research Papers
Live PubMed searches for the peer-reviewed literature on herbal antimicrobial therapy in SIBO and related gut conditions.
- PubMed: SIBO herbal antimicrobial
- PubMed: Berberine and IBS
- PubMed: Allicin against Methanobrevibacter
- PubMed: Oregano oil antibacterial activity
- PubMed: Neem antimicrobial
- PubMed: Berberine and gut motility
- PubMed: Herbal SIBO clinical trials
- PubMed: Carvacrol and gut bacteria
Connections
- The Gut Barrier & Your Microbiome — interactive animation
- SIBO Overview
- Root Causes
- Low-FODMAP Diet
- Prokinetics and Relapse Prevention
- Rifaximin Protocols
- Hydrogen vs Methane vs Hydrogen Sulfide
- Breath Test Guide
- Elemental Diet
- IMO and Constipation
- Oregano
- Berberine
- Peppermint
- Neem
- Goldenseal
- Garlic
- Irritable Bowel Syndrome
- Celiac Disease
- Probiotics