Potassium — Benefits Deep Dive
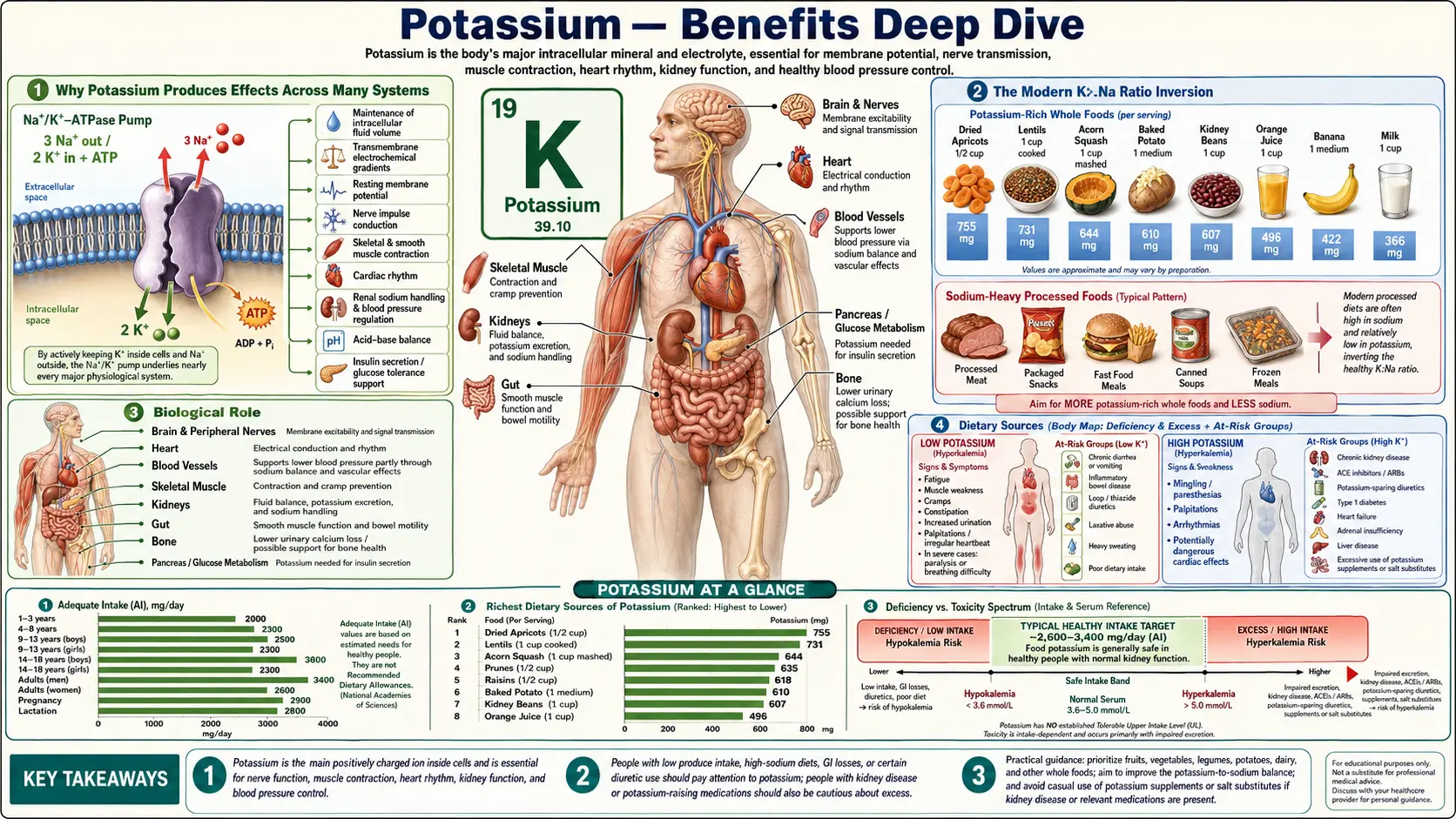
Potassium is the dominant intracellular cation in every cell of the human body. Approximately 98% of total body potassium — some 3,500 mEq in a typical 70 kg adult — resides inside cells at a concentration roughly 35× the extracellular level, while only 2% circulates in the blood and interstitial fluid. This steep gradient is established and maintained by the sodium-potassium ATPase pump, a membrane-spanning enzyme present in every cell of the body, which together with extracellular potassium produces the polarized resting membrane potential that makes every nerve impulse, every muscle contraction, every heartbeat, and every hormone-secreting cell function possible. The opposing role to extracellular sodium is the central design principle of vertebrate physiology — one cation is concentrated inside, the other outside, and life happens in the controlled flow between the two compartments. Humans evolved on a paleolithic diet delivering an estimated 7,000–10,000 mg of potassium per day against only 600–1,500 mg of sodium — a K:Na ratio of roughly 5:1 to 10:1. Industrialized diets have inverted that ratio almost perfectly: typical American intakes are 2,400–2,800 mg potassium against 3,400–4,500 mg sodium, a K:Na ratio of approximately 0.6:1. This modern inversion is the unifying mechanism behind much of the cardiovascular and renal disease burden of industrialized populations. Four deep-dive pages below explore the conditions where adequate potassium produces the largest clinical effect — blood pressure and stroke prevention, cardiac rhythm and sudden cardiac death prevention, muscle function and the exercise-cramp-paralysis continuum, and the practical dietary strategies for reaching adequate intake from whole foods.
Deep-Dive Articles
Blood Pressure
The DASH and DASH-Sodium NEJM trials, the Whelton 1997 JAMA meta-analysis of 33 RCTs showing 3.1 mmHg systolic and 2.0 mmHg diastolic reduction from supplementation, the INTERSALT confirmation that the sodium-to-potassium ratio predicts blood pressure better than either electrolyte alone, the SSaSS 2021 NEJM salt-substitute trial reducing stroke by 14%, vasodilation through endothelial nitric oxide and Kir channels, and the renal WNK-SPAK-NCC pathway that drives natriuresis when potassium intake is high.
Heart Rhythm
The cardiac action potential phase by phase, hypokalemic torsades de pointes and ventricular fibrillation, the digoxin interaction at the Na+/K+-ATPase pump, the progression of hyperkalemic ECG findings from peaked T waves through widened QRS to the sinusoidal pre-terminal rhythm, the magnesium co-replacement requirement for refractory hypokalemia, the cardiac-surgery ICU protocol of maintaining K+ > 4.0 mEq/L to prevent post-op atrial fibrillation, and the emergency calcium-insulin-glucose-bicarbonate-albuterol stack for life-threatening hyperkalemia.
Muscle Function
The Na+/K+-ATPase pump that consumes 20% of resting energy expenditure in muscle, the hypokalemic progression from leg cramps through flaccid paralysis to rhabdomyolysis, hyperkalemic paresthesias and ascending paralysis, the Adolph 1947 demonstration that exercise transiently elevates plasma potassium to 6–8 mEq/L, the rare hypo/hyperkalemic periodic paralysis channelopathies (CACNA1S, SCN4A, KCNJ2), dietary potassium for athletes, the dangerous refeeding hypokalemia of malnourished patients restarted on carbohydrate too aggressively, and smooth-muscle ileus from severe hypokalemia.
Rich Foods
A ranked table of 23 whole foods by potassium per 100 g, dominated by yam, white beans, avocado, plantain, pinto beans, and potatoes — with rice at the bottom for context. Per-gram density versus typical portion size, why leafy greens, edamame, and baked white potato were excluded from the ranking, cooking-method effects (boiling leaches, roasting preserves), illustrative daily menus reaching the 3,400 mg target, and cautions for patients with CKD or on RAAS-blocking medications.
Interactive Visualization The Sodium–Potassium Pump — why you have a voltage Run the pump that gives every cell its charge — three sodium out, two potassium in, on Mg-ATP — then drop the magnesium and see exactly why low potassium refuses to correct. Launch →
Table of Contents
- Deep-Dive Articles
- Why Potassium Produces Effects Across Many Systems
- The Modern K:Na Ratio Inversion
- Research Papers: Blood Pressure and Stroke
- Research Papers: Heart Rhythm and Sudden Cardiac Death
- Research Papers: Muscle, Exercise, and Periodic Paralysis
- Research Papers: Renal Handling and Aldosterone
- Research Papers: Bone, Acid-Base, and Metabolic Effects
- External Authoritative Resources
- Connections
- Featured Videos
Why Potassium Produces Effects Across Many Systems
Most minerals act through one principal mechanism — iron carries oxygen on hemoglobin, calcium triggers muscle contraction, zinc is a cofactor for specific enzymes. Potassium is different. It is the dominant intracellular ion in every cell of the body, and its concentration relative to extracellular sodium sets the resting membrane potential of every excitable cell — neurons, cardiac myocytes, skeletal and smooth muscle fibers, pacemaker cells, glandular epithelium, and immune cells alike. This means that potassium status simultaneously affects every system that depends on electrical signaling, ion-gradient-driven transport, or membrane-potential-regulated cell function.
Five distinct molecular mechanisms produce the spectrum of clinical effects:
- The Na+/K+-ATPase pump and resting membrane potential — the ATP-driven enzyme that establishes and maintains the steep transmembrane potassium and sodium gradients. The roughly −70 to −90 mV resting potential of excitable cells is overwhelmingly set by the ratio of intracellular to extracellular potassium through potassium-selective leak channels. Any disturbance of this gradient propagates to every cell type that depends on a polarized resting state — which is essentially all of them. This is the unifying mechanism underlying the cardiac action potential and skeletal muscle contraction.
- Cardiac action potential repolarization — the heart's electrical activity depends on precisely-timed opening of multiple distinct potassium channels (Ito, IKr, IKs, IK1) during phases 1, 2, 3, and 4 of the cardiac action potential. Even small deviations from normal extracellular potassium concentration disrupt this timing, producing the hypokalemic prolonged-QT-and-torsades pattern or the hyperkalemic peaked-T-wave-and-sinusoidal-QRS progression.
- Vascular smooth muscle relaxation — elevated extracellular potassium activates inward rectifier potassium channels (Kir) on vascular smooth muscle cells, hyperpolarizing them, closing voltage-gated calcium channels, and producing vasodilation. Potassium also stimulates endothelial nitric oxide synthase. The combination produces the consistent blood-pressure-lowering effect of dietary potassium documented in the DASH trials and the Whelton meta-analysis.
- Insulin-mediated potassium uptake — insulin stimulates the Na+/K+-ATPase in skeletal muscle and other tissues, driving potassium into cells along with glucose. This produces the dangerous post-prandial hypokalemia of refeeding syndrome and the post-prandial paralysis attacks of hypokalemic periodic paralysis. It also explains why insulin plus glucose is the second-line emergency treatment for severe hyperkalemia.
- Aldosterone feedback loop — rising serum potassium directly stimulates aldosterone release from the adrenal cortex, which in turn drives renal potassium excretion through ENaC and ROMK channels in the cortical collecting duct. This is the dominant chronic regulatory mechanism keeping serum potassium within the narrow 3.5–5.0 mEq/L range despite huge day-to-day variation in dietary intake. Disruption of this loop — primary hyperaldosteronism (Conn's syndrome), licorice-induced apparent mineralocorticoid excess, or ACE inhibitor / ARB / spironolactone use — produces the chronic hypokalemia or hyperkalemia syndromes most commonly seen in clinical practice.
The clinical translation: when potassium intake is inadequate or when one of these regulatory mechanisms is disrupted, the consequences spread across every organ system that depends on the potassium gradient. The same patient may simultaneously have leg cramps (skeletal muscle), constipation (gut smooth muscle), palpitations (cardiac), elevated blood pressure (vascular smooth muscle and renal sodium handling), and fatigue (CNS), all from one electrolyte disturbance.
The Modern K:Na Ratio Inversion
The single most important framing for understanding potassium and modern disease is the K:Na ratio inversion that industrialized food production has produced over the past 150 years. Humans evolved over millions of years on a diet of fruits, leaves, roots, tubers, nuts, seeds, lean game meat, and occasional eggs and shellfish. Reconstructions of paleolithic intake from comparative dietary anthropology suggest a daily potassium intake of approximately 7,000–10,000 mg against a sodium intake of approximately 600–1,500 mg. The K:Na molar ratio of that diet was approximately 5:1 to 10:1 — substantially more potassium than sodium.
Modern American adults consume on average approximately 2,400–2,800 mg of potassium against 3,400–4,500 mg of sodium. The K:Na molar ratio of this diet is approximately 0.6:1 — about 10× less potassium-rich relative to sodium than the diet our physiology evolved to handle. This inversion is not a small dietary preference shift — it is a wholesale flip of one of the fundamental boundary conditions our cellular machinery assumes.
Three changes produced the inversion:
- Salt as a preservative and flavoring agent — the rise of preserved meats (cured ham, salt pork), cheese, salted fish, pickled vegetables, and ultimately industrial bread baking and processed-food formulation pushed sodium intake from a small fraction of natural intake to multiples of physiological requirement.
- Refined cereal grains displacing high-K whole foods — wheat, refined rice, and corn (and the products made from them) are essentially potassium-free relative to fruits, tubers, and legumes. The shift from a fruit-tuber-legume-meat diet to a wheat-and-meat or rice-and-meat or corn-and-meat diet dropped potassium intake dramatically.
- Reduced fruit and vegetable consumption — per capita fruit and vegetable consumption in industrialized populations falls well short of the 8–10 servings per day that the original DASH trial used to deliver 4,700 mg of potassium. The "5-a-day" public health target, even when met, delivers only 2,500–3,500 mg of potassium — better than the average but still short of paleolithic intake.
The biological consequences of the K:Na inversion are visible across the population:
- Hypertension is the leading modifiable risk factor for cardiovascular disease worldwide — affecting more than one billion adults. The INTERSALT study established that populations consuming a paleolithic-like K:Na ratio (Yanomami of Brazil, Xingu of Brazil, some traditional rural Chinese populations) have essentially no hypertension at any age and no age-related rise in blood pressure. Populations with the most inverted K:Na ratios (industrialized countries with high salt intake and low fruit/vegetable intake) have the highest hypertension prevalence and the steepest age-related blood pressure rise.
- Stroke is the third leading cause of death globally — and the Aburto 2013 BMJ meta-analysis showed that higher potassium intake reduces stroke risk by approximately 24%, with much of this effect independent of blood pressure reduction.
- Sudden cardiac death — prospective cohort studies consistently link low serum and dietary potassium to elevated sudden-cardiac-death risk, particularly in patients on potassium-wasting diuretics.
- Chronic kidney disease progression — the high-sodium / low-potassium pattern accelerates the progression of established CKD, and the SSaSS 2021 NEJM trial demonstrated that even a modest shift toward higher potassium / lower sodium (substituting 25% of dietary salt with potassium chloride) reduced cardiovascular events by 13%.
- Osteoporosis and kidney stones — chronic acid load from sodium-rich processed diets pulls calcium out of bone for buffering and excretes it in urine, where it precipitates as calcium-oxalate or calcium-phosphate stones. The alkalinizing effect of potassium-rich fruits and vegetables (which deliver bicarbonate precursors as citrate and malate salts) neutralizes this acid load and partially reverses both bone loss and stone formation.
The therapeutic lever is straightforward: shift the K:Na ratio back toward the evolutionary range by increasing fruit, vegetable, legume, and tuber intake, and by reducing processed food intake. The Rich-Foods page ranks specific whole foods by their potassium density.
Research Papers: Blood Pressure and Stroke
- Appel LJ, Moore TJ, Obarzanek E, et al. (1997). A clinical trial of the effects of dietary patterns on blood pressure (DASH). New England Journal of Medicine;336(16):1117-1124. — DOI: 10.1056/NEJM199704173361601
- Sacks FM, Svetkey LP, Vollmer WM, et al. (2001). Effects on blood pressure of reduced dietary sodium and the DASH diet (DASH-Sodium). New England Journal of Medicine;344(1):3-10. — DOI: 10.1056/NEJM200101043440101
- Whelton PK, He J, Cutler JA, et al. (1997). Effects of oral potassium on blood pressure: meta-analysis of randomized controlled clinical trials. JAMA;277(20):1624-1632. — DOI: 10.1001/jama.1997.03540440058033
- Aburto NJ, Hanson S, Gutierrez H, Hooper L, Elliott P, Cappuccio FP. (2013). Effect of increased potassium intake on cardiovascular risk factors and disease: systematic review and meta-analysis. BMJ;346:f1378. — DOI: 10.1136/bmj.f1378
- Neal B, Wu Y, Feng X, et al. (2021). Effect of salt substitution on cardiovascular events and death (SSaSS). New England Journal of Medicine;385(12):1067-1077. — DOI: 10.1056/NEJMoa2105675
- INTERSALT Cooperative Research Group (1988). INTERSALT: an international study of electrolyte excretion and blood pressure. BMJ;297(6644):319-328. — PubMed
- D'Elia L, Barba G, Cappuccio FP, Strazzullo P. (2011). Potassium intake, stroke, and cardiovascular disease: a meta-analysis. Journal of the American College of Cardiology;57(10):1210-1219. — DOI: 10.1016/j.jacc.2010.09.070
- Mente A, O'Donnell M, Rangarajan S, et al. (2014). Association of urinary sodium and potassium excretion with blood pressure (PURE). NEJM;371(7):601-611. — DOI: 10.1056/NEJMoa1311989
- PubMed — Potassium, vascular endothelium, and nitric oxide
- PubMed — DASH diet long-term cardiovascular outcomes
Research Papers: Heart Rhythm and Sudden Cardiac Death
- Macdonald JE, Struthers AD. (2004). What is the optimal serum potassium level in cardiovascular patients? Journal of the American College of Cardiology;43(2):155-161. — DOI: 10.1016/j.jacc.2003.06.021
- Goyal A, Spertus JA, Gosch K, et al. (2012). Serum potassium levels and mortality in acute myocardial infarction. JAMA;307(2):157-164. — DOI: 10.1001/jama.2011.1967
- Cohn JN, Kowey PR, Whelton PK, Prisant LM. (2000). New guidelines for potassium replacement in clinical practice. Archives of Internal Medicine;160(16):2429-2436. — DOI: 10.1001/archinte.160.16.2429
- Roden DM (2008). Long-QT syndrome. New England Journal of Medicine;358(2):169-176. — DOI: 10.1056/NEJMcp0706513
- PubMed — Serum potassium and sudden cardiac death (cohort studies)
- PubMed — IKr / hERG potassium channel and long QT syndrome
- PubMed — Torsades de pointes, hypokalemia, and early afterdepolarizations
- PubMed — Emergency management of hyperkalemia
- PubMed — Post-cardiac-surgery potassium and atrial fibrillation
- PubMed — Patiromer and sodium zirconium cyclosilicate
Research Papers: Muscle, Exercise, and Periodic Paralysis
- Clausen T (2003). Na+-K+ pump regulation and skeletal muscle contractility. Physiological Reviews;83(4):1269-1324. — DOI: 10.1152/physrev.00011.2003
- Sejersted OM, Sjøgaard G (2000). Dynamics and consequences of potassium shifts in skeletal muscle and heart during exercise. Physiological Reviews;80(4):1411-1481. — DOI: 10.1152/physrev.2000.80.4.1411
- Lindinger MI, Sjøgaard G (1991). Potassium regulation during exercise and recovery. Sports Medicine;11(6):382-401. — PubMed
- Adolph EF and Associates (1947). Physiology of Man in the Desert. Interscience Publishers, New York. — classic exercise-induced hyperkalemia documentation. — PubMed
- Cannon SC (2010). Voltage-sensor mutations in channelopathies of skeletal muscle. Journal of Physiology;588(11):1887-1895. — DOI: 10.1113/jphysiol.2010.186874
- Statland JM, Tawil R (2018). Periodic Paralysis. Continuum (Minneap Minn);24(6):1696-1711. — DOI: 10.1212/CON.0000000000000676
- Mehanna HM, Moledina J, Travis J (2008). Refeeding syndrome: what it is, and how to prevent and treat it. BMJ;336(7659):1495-1498. — DOI: 10.1136/bmj.a301
- Schwellnus MP, Drew N, Collins M (2008). Muscle cramping in athletes — risk factors, clinical assessment, and management. Clinics in Sports Medicine;27(1):183-194. — PubMed
- PubMed — Severe hypokalemia and rhabdomyolysis
- PubMed — Na/K-ATPase in skeletal muscle and exercise training
Research Papers: Renal Handling and Aldosterone
- Palmer BF (2015). Regulation of potassium homeostasis. Clinical Journal of the American Society of Nephrology;10(6):1050-1060. — DOI: 10.2215/CJN.08580813
- Welling PA (2013). Regulation of renal potassium secretion: molecular mechanisms. Seminars in Nephrology;33(3):215-228. — DOI: 10.1016/j.semnephrol.2013.04.002
- Wang WH, Giebisch G (2009). Regulation of potassium (K) handling in the renal collecting duct. Pflugers Archiv;458(1):157-168. — DOI: 10.1007/s00424-008-0593-3
- Funder JW, Carey RM, Mantero F, et al. (2016). The Management of Primary Aldosteronism: An Endocrine Society Clinical Practice Guideline. Journal of Clinical Endocrinology & Metabolism;101(5):1889-1916. — DOI: 10.1210/jc.2015-4061
- Subramanya AR, Ellison DH (2014). Distal convoluted tubule. Clinical Journal of the American Society of Nephrology;9(12):2147-2163. — DOI: 10.2215/CJN.05920613
- PubMed — WNK kinase, NCC regulation, and distal nephron potassium handling
- PubMed — ROMK renal potassium channel
- PubMed — Gitelman syndrome (NCC mutation, thiazide-like)
- PubMed — Bartter syndrome (loop diuretic-like)
- PubMed — Conn's syndrome / primary aldosteronism
Research Papers: Bone, Acid-Base, and Metabolic Effects
- Sebastian A, Harris ST, Ottaway JH, et al. (1994). Improved mineral balance and skeletal metabolism in postmenopausal women treated with potassium bicarbonate. NEJM;330(25):1776-1781. — DOI: 10.1056/NEJM199406233302502
- New SA, Macdonald HM, Campbell MK, et al. (2004). Lower estimates of net endogenous noncarbonic acid production are positively associated with indexes of bone health in premenopausal and perimenopausal women. American Journal of Clinical Nutrition;79(1):131-138. — DOI: 10.1093/ajcn/79.1.131
- Lemann J Jr, Bushinsky DA, Hamm LL (2003). Bone buffering of acid and base in humans. American Journal of Physiology - Renal Physiology;285(5):F811-F832. — DOI: 10.1152/ajprenal.00115.2003
- Frassetto LA, Morris RC Jr, Sellmeyer DE, Sebastian A (2008). Adverse effects of sodium chloride on bone in the aging human population resulting from habitual consumption of typical American diets. Journal of Nutrition;138(2):419S-422S. — DOI: 10.1093/jn/138.2.419S
- Eaton SB, Konner M (1985). Paleolithic nutrition. A consideration of its nature and current implications. NEJM;312(5):283-289. — DOI: 10.1056/NEJM198501313120505
- PubMed — Potassium citrate and kidney-stone prevention
- PubMed — Insulin-mediated potassium uptake
- PubMed — Potassium intake and bone mineral density
- PubMed — Dietary acid load (PRAL) and net endogenous acid production
- PubMed — Chronic hypokalemic nephropathy
External Authoritative Resources
- Linus Pauling Institute — Potassium Micronutrient Information Center — the single most authoritative scientific summary of potassium biology, regularly updated
- NIH Office of Dietary Supplements — Potassium Fact Sheet (Health Professionals)
- Harvard T.H. Chan School of Public Health — The Nutrition Source: Potassium
- National Academies of Sciences, Engineering, and Medicine — Dietary Reference Intakes for Sodium and Potassium (2019)
- USDA FoodData Central — primary database of potassium content for all foods
- WHO Healthy Diet Fact Sheet — includes the Na:K ratio recommendation
- PubMed — All research on potassium intake and cardiovascular disease
Connections
- The Sodium–Potassium Pump — interactive animation
- Potassium (Main Page)
- Potassium for Blood Pressure
- Potassium for Heart Rhythm
- Potassium for Muscle Function
- Hypokalemia (Low Potassium) Symptoms
- Potassium-Rich Foods
- All Minerals
- Magnesium (Na/K-ATPase Cofactor)
- Magnesium and Heart Health
- Calcium
- Phosphorus
- Hypertension
- Arrhythmia
- Atrial Fibrillation
- Heart Failure
- Stroke
- Kidney Disease
- Heart Palpitations
- Bananas
- Avocado
- Spinach
- Sweet Potatoes
- Lentils
- Broccoli
- Celery Juice and Blood Pressure
- Cramp Prevention
- Magnesium Replenishment
- Comprehensive Metabolic Panel