Heart Palpitations
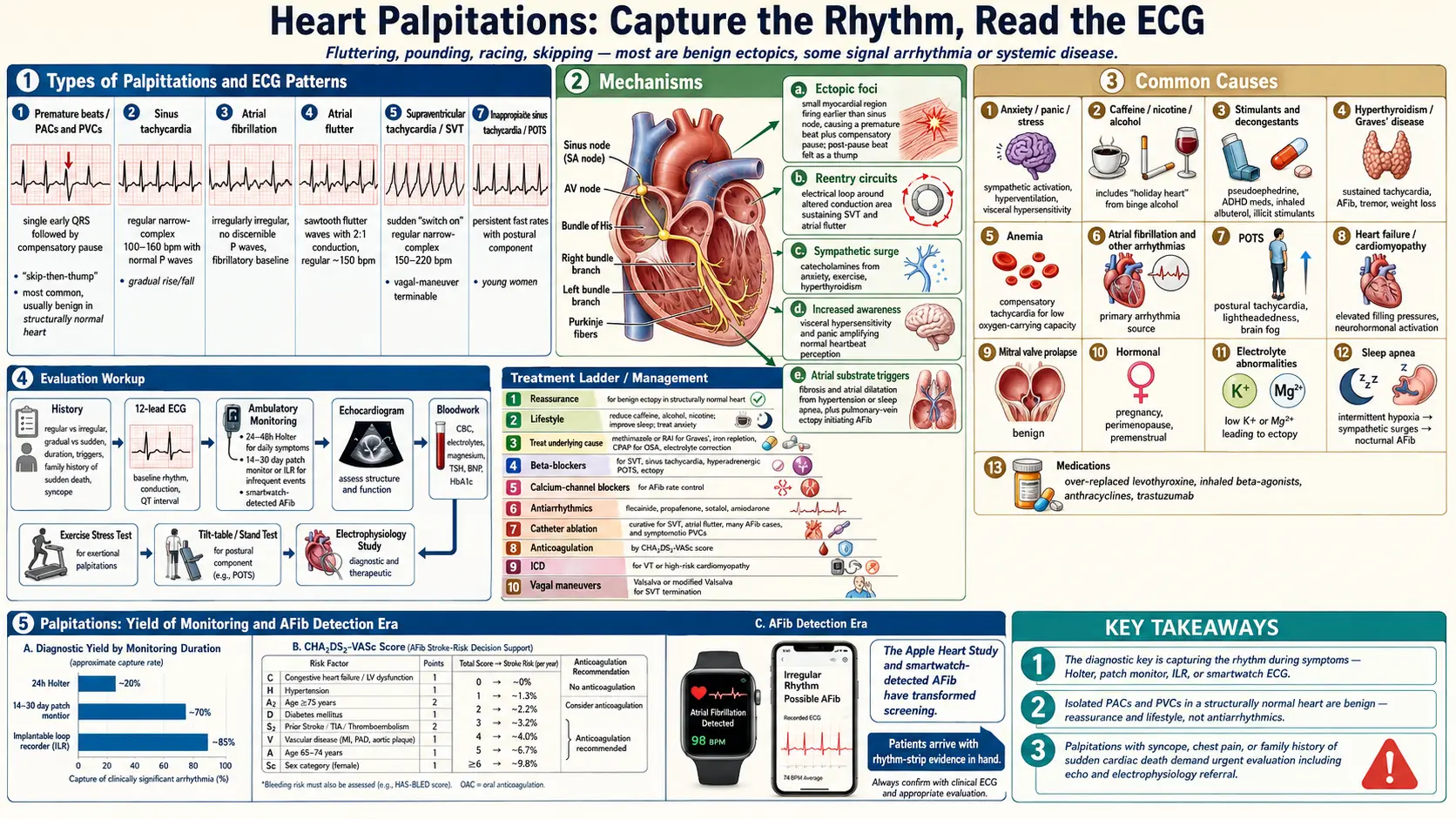

Table of Contents
- Overview
- Types of Palpitations
- Common Causes
- Mechanisms
- Evaluation
- Management
- When to Seek Medical Care
- Connections
- References & Research
- Featured Videos
Overview
Heart palpitations are the conscious awareness of the heart beating — described as fluttering, pounding, racing, skipping, or thumping. Most palpitations are benign and reflect ordinary ectopic beats (premature atrial or ventricular contractions), caffeine, sleep deprivation, anxiety, or hormonal shifts. A meaningful minority signal a treatable arrhythmia or systemic condition. The most useful question is what the palpitations do: a few skipped beats while resting feel different from a sudden rapid run lasting minutes, and the latter requires capture on a recording device for diagnosis.
Types of Palpitations
- Premature beats (PACs and PVCs) — the single most common cause; described as a skip, a hard beat, or a flip. Usually benign in the structurally normal heart.
- Sinus tachycardia — gradual rise and fall in rate, often tied to exertion, fever, anxiety, dehydration, or anemia.
- Atrial fibrillation — irregular and often rapid, may feel chaotic. Risk rises with age, hypertension, sleep apnea, alcohol, and hyperthyroidism.
- Atrial flutter — sudden onset, regular and rapid, often with 2:1 conduction.
- Supraventricular tachycardia (SVT) — sudden "switch on" of a regular fast rhythm at 150–220 bpm, often terminated by vagal maneuvers.
- Ventricular tachycardia — rapid, often associated with structural heart disease; medical emergency if sustained.
- Inappropriate sinus tachycardia and POTS — persistent fast rates with postural component, common in young women.
Common Causes
- Anxiety, panic, and stress — sympathetic activation, hyperventilation, and visceral hypersensitivity amplify ordinary heartbeat awareness.
- Caffeine, nicotine, alcohol — particularly binge alcohol intake ("holiday heart").
- Stimulants and decongestants — pseudoephedrine, ADHD medications, asthma inhalers (albuterol), illicit stimulants.
- Hyperthyroidism (Graves' disease) — produces sustained tachycardia, atrial fibrillation, tremor, and weight loss.
- Anemia — the heart compensates for low oxygen-carrying capacity by speeding up.
- Atrial fibrillation and other arrhythmias — structural and electrical disorders of the atria, AV node, ventricles.
- POTS — postural tachycardia, often with lightheadedness and brain fog.
- Heart failure and cardiomyopathy — can present with palpitations from arrhythmia or compensatory tachycardia.
- Mitral valve prolapse — benign, common, and a frequent source of palpitation awareness.
- Hormonal — pregnancy, perimenopause, premenstrual phase.
- Electrolyte abnormalities — low potassium or magnesium increases ectopy.
- Sleep apnea — intermittent hypoxia and surges in sympathetic tone trigger nocturnal palpitations and atrial fibrillation.
- Medications — thyroid replacement (over-replacement), inhaled beta-agonists, some chemotherapies (anthracyclines, trastuzumab).
Mechanisms
- Ectopic foci — a small region of myocardium fires earlier than the sinus node, producing a premature beat followed by a compensatory pause; the post-pause beat is often felt as a thump.
- Reentry circuits — an electrical impulse loops around an area of altered conduction, sustaining tachyarrhythmias such as SVT and atrial flutter.
- Sympathetic surge — catecholamines from anxiety, exercise, or hyperthyroidism increase rate and contractility.
- Increased awareness — visceral hypersensitivity and panic disorder amplify awareness of normal heartbeat.
- Triggers in atrial substrate — fibrosis, atrial dilatation (from hypertension or sleep apnea), and pulmonary-vein ectopy initiate atrial fibrillation.
Evaluation
- History — pattern (regular vs irregular), onset (gradual vs sudden), duration, triggers, family history of sudden death, syncope.
- 12-lead ECG — baseline rhythm, conduction abnormalities, QT interval.
- Ambulatory monitoring — 24- to 48-hour Holter for daily symptoms; 14- to 30-day patch monitor or implantable loop recorder for less frequent events.
- Echocardiogram — rule out structural heart disease, valvular disease, hypertrophy.
- Bloodwork — CBC, electrolytes, magnesium, TSH, BNP, HbA1c.
- Exercise stress testing — if exertional palpitations or risk factors for ischemia.
- Tilt-table or stand test — if postural component.
- Electrophysiology study — for sustained or unexplained arrhythmias and to guide ablation.
Management
- Reassurance for benign ectopy — in a structurally normal heart with normal monitor and echo, isolated PACs and PVCs warrant lifestyle measures, not antiarrhythmics.
- Lifestyle changes — reduce caffeine, alcohol, nicotine, and stimulants; improve sleep; treat anxiety; manage weight.
- Treat the underlying condition — methimazole or radioactive iodine for Graves', iron repletion for anemia, CPAP for sleep apnea, electrolyte correction.
- Beta-blockers — rate control and symptom relief for SVT, sinus tachycardia, hyperadrenergic POTS, and benign ectopy.
- Calcium-channel blockers — rate control in atrial fibrillation when beta-blockers are not tolerated.
- Antiarrhythmic drugs — flecainide, propafenone, sotalol, amiodarone for rhythm control.
- Catheter ablation — curative for SVT, atrial flutter, and many cases of atrial fibrillation and symptomatic PVCs.
- Anticoagulation — for atrial fibrillation based on stroke risk (CHA2DS2-VASc).
- Implantable cardioverter-defibrillator — for ventricular tachycardia or high-risk cardiomyopathy.
- Vagal maneuvers — the Valsalva or modified Valsalva (lying back, leg raise) can terminate SVT.
When to Seek Medical Care
- Palpitations with chest pain, pressure, or jaw or arm pain.
- Loss of consciousness or near-syncope during palpitations.
- Palpitations that last more than several minutes, or that recur frequently.
- Family history of sudden cardiac death, particularly under age 50.
- Palpitations with new shortness of breath, leg swelling, or exercise intolerance.
- Known structural heart disease, prior heart attack, or cardiomyopathy.
- Palpitations with weight loss, tremor, and heat intolerance (rule out hyperthyroidism).
Connections
- Anxiety
- Atrial Fibrillation
- POTS
- Cardiomyopathy
- Anemia
- Arrhythmia
- Heart Failure
- Obstructive Sleep Apnea
- Graves' Disease
- Hypertension
- Lightheadedness
- Thyroid Disorders
- Magnesium
- Potassium
- Shortness of Breath
- Chest Pain
- Insomnia
- MSG
References & Research
Historical Background
Awareness of the heartbeat has been recorded since antiquity, but Holter's 1949 invention of the portable ECG monitor made systematic study of palpitations possible. The 21st century has produced increasingly sophisticated wearables, from patch monitors to consumer smartwatches that detect atrial fibrillation, transforming an occasionally elusive symptom into one frequently caught on tape before the doctor visit.
Key Research Papers
- Raviele A, Giada F, Bergfeldt L, et al. Management of patients with palpitations: a position paper from the European Heart Rhythm Association. Europace. 2011;13(7):920-934.
- Hindricks G, Potpara T, Dagres N, et al. 2020 ESC guidelines for the diagnosis and management of atrial fibrillation. European Heart Journal. 2021;42(5):373-498.
- Weber BE, Kapoor WN. Evaluation and outcomes of patients with palpitations. American Journal of Medicine. 1996;100(2):138-148.
- Page RL, Joglar JA, Caldwell MA, et al. 2015 ACC/AHA/HRS guideline for the management of adult patients with supraventricular tachycardia. Circulation. 2016;133(14):e506-e574.
- Perez MV, Mahaffey KW, Hedlin H, et al. Large-scale assessment of a smartwatch to identify atrial fibrillation. New England Journal of Medicine. 2019;381(20):1909-1917.
- January CT, Wann LS, Calkins H, et al. 2019 AHA/ACC/HRS focused update of the 2014 guideline for the management of patients with atrial fibrillation. Circulation. 2019;140(2):e125-e151.
- Marcus GM, Vittinghoff E, Whitman IR, et al. Acute consumption of alcohol and discrete atrial fibrillation events. Annals of Internal Medicine. 2021;174(11):1503-1509.
- Linz D, McEvoy RD, Cowie MR, et al. Sleep-disordered breathing and atrial fibrillation. JAMA Cardiology. 2018;3(6):532-540.
- Locati ET, Vecchi AM, Vargiu S, et al. Role of extended external loop recorders for the diagnosis of unexplained syncope, presyncope, and sustained palpitations. Pacing and Clinical Electrophysiology. 2014;37(12):1720-1728.
- Barsky AJ. Palpitations, arrhythmias, and awareness of cardiac activity. Annals of Internal Medicine. 2001;134(9 Pt 2):832-837.
PubMed Topic Searches
- Evaluation of palpitations
- Atrial fibrillation screening with wearables
- Premature ventricular contractions: benign or pathologic?
- Hyperthyroidism and atrial fibrillation
- POTS and inappropriate sinus tachycardia
- Panic disorder and palpitations