Kidney Disease
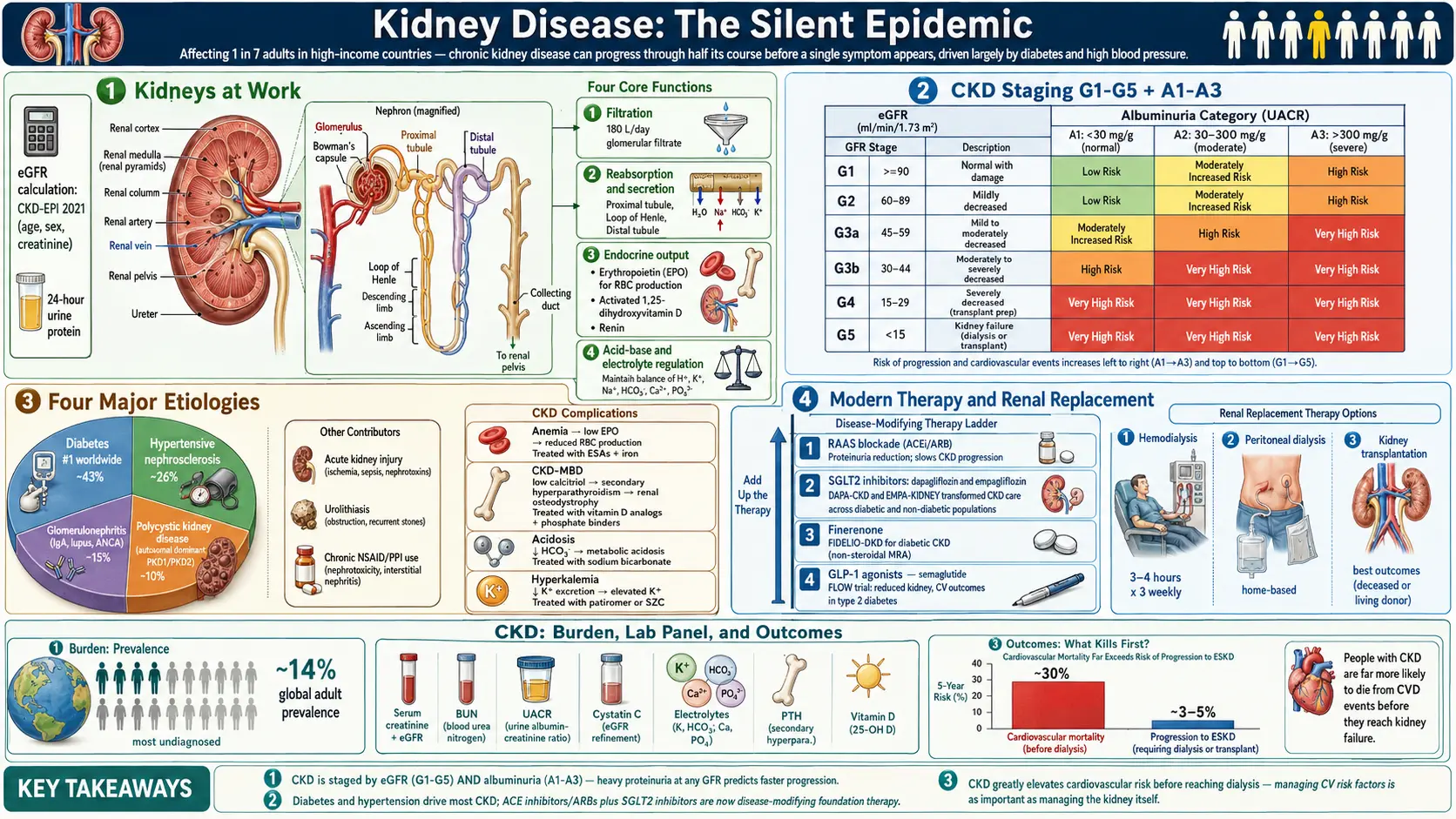
The kidneys are the body's silent chemists — two fist-sized organs that filter roughly 180 liters of blood per day, regulate blood pressure, balance electrolytes, activate vitamin D, produce erythropoietin for red blood cell formation, and quietly remove the metabolic waste generated by every cell in the body. When they start to fail, they fail quietly. Chronic kidney disease (CKD) can progress through half of its course before a single symptom appears, which is why it is sometimes called the silent epidemic: an estimated 1 in 7 adults in high-income countries have some degree of CKD, and most of them do not know it. The good news is that CKD is largely a disease of two other conditions — diabetes and high blood pressure — and is therefore substantially preventable and, especially in its earlier stages, slowable with the right medical, nutritional, and lifestyle strategies.
Deep-Dive Articles
Kidney disease is a big topic, and most people arrive with one specific worry — a lab result, a new diagnosis, a diet question, or a decision about what comes next. The five guides below each go deep on one part of the journey. Start wherever you are.
Understanding Your eGFR & CKD Stage
What your eGFR number really means, how the G1–G5 stages and the albuminuria (UACR) axis combine in the KDIGO risk map, when creatinine misleads, and when to ask for a nephrologist.
The Kidney-Friendly Diet
Sodium, potassium, phosphorus, and protein in plain language — with real food lists, label-reading tricks, the potassium double-edge, and why the rules flip on dialysis.
Slowing CKD Progression
The modern toolkit that changed the outlook: SGLT2 inhibitors, finerenone, GLP-1s, ACE/ARBs, and blood-pressure targets — plus nephrotoxins to avoid and a what-to-ask-your-doctor checklist.
Diabetic Kidney Disease
The number-one cause of kidney failure: why diabetes harms the kidneys, the microalbuminuria early-warning test, and the four pillars of protection that can now slow it dramatically.
Dialysis & Transplant
Preparing for kidney failure without panic: hemodialysis vs peritoneal dialysis vs transplant vs conservative care, how access works, and why planning early matters.
Table of Contents
- Deep-Dive Articles
- What is Kidney Disease?
- Types of Kidney Disease
- Stages of Chronic Kidney Disease
- Common Symptoms
- Causes and Risk Factors
- Diagnosis
- Lab Tests to Monitor
- Treatment Options
- Natural & Nutritional Support
- Prevention and Management Strategies
- Complications of Kidney Disease
- References & Research
- Featured Videos
What is Kidney Disease?
Kidney disease refers to any condition that affects the kidneys' ability to filter waste and excess fluids from the blood to produce urine. When kidneys are damaged, waste can build up in the body, leading to a range of health problems. Kidney disease can be acute (sudden) or chronic (long-term), with chronic kidney disease (CKD) being more common and potentially leading to kidney failure if not managed properly.
Types of Kidney Disease
1. Chronic Kidney Disease (CKD)
- Long-term condition characterized by a gradual loss of kidney function over time.
- Common causes: Diabetes, high blood pressure, and glomerulonephritis.
2. Acute Kidney Injury (AKI)
- Sudden decrease in kidney function, often due to severe illness, injury, or certain medications.
- Can be reversible with prompt treatment.
3. Polycystic Kidney Disease (PKD)
- Genetic disorder that causes cysts to form in the kidneys, impairing their function.
- Can lead to CKD and kidney failure over time.
4. Glomerulonephritis
- Inflammation of the glomeruli, the tiny filtering units in the kidneys.
- Can be acute or chronic and may result from infections, autoimmune diseases, or other conditions.
Stages of Chronic Kidney Disease
CKD is classified into five stages based on the estimated glomerular filtration rate (eGFR), a measure of how much blood the kidneys filter each minute, normalized to body surface area. Staging guides both monitoring frequency and treatment intensity. An eGFR below 60 mL/min/1.73 m² sustained for more than three months is the clinical threshold for CKD.
| Stage | eGFR (mL/min/1.73 m²) | Description | Typical Management |
|---|---|---|---|
| Stage 1 | ≥ 90 | Normal filtration with evidence of kidney damage (e.g., protein in urine, imaging changes) | Treat underlying cause; control blood pressure and blood sugar |
| Stage 2 | 60–89 | Mildly reduced filtration with kidney damage | Aggressive risk-factor control; annual monitoring |
| Stage 3a | 45–59 | Mild to moderate loss of function | Every 6–12 months monitoring; ACE inhibitor or ARB; SGLT2 inhibitor if diabetic |
| Stage 3b | 30–44 | Moderate to severe loss of function | Nephrology referral; manage anemia, bone disease, acidosis |
| Stage 4 | 15–29 | Severe loss of function | Prepare for renal replacement therapy; dietary protein restriction |
| Stage 5 | < 15 | Kidney failure | Dialysis or kidney transplant required |
A separate albuminuria axis (A1, A2, A3) modifies the stage based on urine protein loss. A patient with stage 3a eGFR but heavy proteinuria (A3) has a substantially worse prognosis than stage 3a with minimal proteinuria (A1), which is why modern CKD guidelines describe patients by both dimensions.
Common Symptoms of Kidney Disease
Symptoms may not appear until the disease is advanced. Common signs include:
- Fatigue and weakness
- Swelling (edema) in the legs, ankles, or feet
- Frequent urination, especially at night
- Blood in the urine
- Foamy urine due to excess protein
- High blood pressure
- Loss of appetite
- Nausea and vomiting
Causes and Risk Factors
- Diabetes: High blood sugar can damage blood vessels in the kidneys.
- High blood pressure: Can damage the kidneys over time.
- Genetic disorders: Such as polycystic kidney disease.
- Infections and autoimmune diseases: Such as lupus and glomerulonephritis.
- Prolonged use of certain medications: Such as NSAIDs and some antibiotics.
- Age: Risk increases with age, particularly after 60.
Diagnosis
- Blood tests: To measure levels of creatinine and estimate the glomerular filtration rate (eGFR).
- Urine tests: To check for protein or blood in the urine.
- Imaging tests: Ultrasound or CT scans to examine the structure of the kidneys.
- Kidney biopsy: To take a small tissue sample for examination.
Lab Tests to Monitor
Routine kidney-function monitoring relies on a small, focused panel of tests. Most of these are components of the Comprehensive Metabolic Panel ordered at a typical annual physical, plus a dedicated urine test.
- Serum creatinine: A waste product of muscle metabolism that the kidneys filter. Rising levels indicate declining function, though values vary with muscle mass.
- Estimated glomerular filtration rate (eGFR): Calculated from creatinine, age, and sex using the 2021 CKD-EPI equation. The single most important number for staging CKD.
- Blood urea nitrogen (BUN): Another nitrogen-containing waste product. Elevated levels can reflect reduced filtration, dehydration, or high protein intake.
- Urine albumin-to-creatinine ratio (UACR): Detects small amounts of albumin leaking into the urine — often the earliest sign of kidney damage, years before eGFR drops.
- Cystatin C: An alternative marker independent of muscle mass, useful in elderly, very lean, or very muscular patients where creatinine is misleading.
- Serum electrolytes: Potassium, sodium, bicarbonate, calcium, and phosphorus all shift as kidney function declines and must be monitored regularly.
- Parathyroid hormone (PTH) and vitamin D: CKD-mineral and bone disorder (CKD-MBD) develops as kidneys lose the ability to activate vitamin D, driving secondary hyperparathyroidism.
Treatment Options
- Medications:
- Blood pressure drugs: Such as ACE inhibitors or ARBs to manage blood pressure and slow kidney damage.
- Diuretics: To reduce swelling.
- Medications for diabetes: To control blood sugar levels.
- Dietary changes:
- Limit sodium to control blood pressure and reduce fluid retention.
- Reduce protein intake to decrease the workload on the kidneys.
- Stay hydrated and maintain a balanced diet.
- Dialysis:
- Hemodialysis: Filters blood outside the body using a machine.
- Peritoneal dialysis: Uses the lining of the abdomen to filter blood inside the body.
- Kidney transplant: For end-stage kidney disease, a healthy kidney from a donor is transplanted to replace the damaged kidneys.
Natural & Nutritional Support
Medical therapy slows CKD; nutrition and targeted micronutrients protect the downstream systems that fail alongside the kidneys. These are adjuncts to conventional care, not substitutes, and every one of them interacts with kidney clearance — talk to your nephrologist before starting anything new, especially at stages 3b and beyond.
- Vitamin D3: Healthy kidneys convert 25(OH)D to the active hormone 1,25(OH)₂D. In CKD this conversion falters, contributing to secondary hyperparathyroidism, bone loss, and immune dysfunction. Supplementation is routinely used in CKD under clinician guidance.
- Magnesium: Often low in early CKD and important for blood pressure control, vascular calcification resistance, and glucose handling. In advanced CKD, however, magnesium can accumulate — dose only with lab monitoring.
- Potassium: A double-edged sword. A potassium-rich plant-forward diet lowers blood pressure and protects early-stage kidneys, but in stages 3b–5 the kidneys lose the ability to excrete potassium, and hyperkalemia becomes life-threatening. Know your stage.
- Turmeric (curcumin): Anti-inflammatory and antifibrotic in animal models of diabetic nephropathy and obstructive uropathy. Early human trials are promising but small; avoid high doses with blood thinners.
- Dietary protein: Moderate restriction (0.6–0.8 g/kg/day) may slow progression in stages 3–4, but must be individualized. Plant-based protein sources appear gentler on the kidneys than red meat.
- Sodium restriction: Keep intake below 2,000 mg/day. This single change can lower blood pressure as effectively as adding a second antihypertensive medication.
- Omega-3 fatty acids: Associated with reduced proteinuria and slower progression in IgA nephropathy trials. Food-first from oily fish is safest.
Prevention and Management Strategies
- Manage blood pressure and diabetes to prevent kidney damage.
- Maintain a healthy diet with low sodium and low protein.
- Stay hydrated and avoid dehydration.
- Limit use of NSAIDs and other medications that can affect kidney function.
- Quit smoking and avoid excessive alcohol consumption.
- Regular check-ups: Monitor kidney function if at risk for kidney disease.
Complications of Kidney Disease
- Fluid retention: Can lead to swelling, high blood pressure, and pulmonary edema.
- Heart disease: Increased risk due to high blood pressure and fluid buildup.
- Anemia: Reduced production of erythropoietin, leading to fewer red blood cells.
- Bone health issues: Imbalances in calcium and phosphorus can lead to bone weakening.
- Electrolyte imbalances: Affecting heart and muscle function.
- Kidney failure: Requires dialysis or kidney transplant for survival.
References & Research
Historical Background
Richard Bright, a physician at Guy's Hospital in London, first described the connection between kidney disease and protein in the urine in 1827, and chronic kidney disease was long known as "Bright's disease." The development of hemodialysis by Willem Kolff in 1943 in the Netherlands and the first successful kidney transplant by Joseph Murray in 1954 (for which he received the 1990 Nobel Prize) were transformative milestones in nephrology.
Key Research Papers
- Levey AS, Coresh J. Chronic kidney disease. The Lancet. 2012;379(9811):165-180.
- Levey AS, Stevens LA, Schmid CH, et al. A new equation to estimate glomerular filtration rate. Annals of Internal Medicine. 2009;150(9):604-612.
- Jha V, Garcia-Garcia G, Iseki K, et al. Chronic kidney disease: global dimension and perspectives. The Lancet. 2013;382(9888):260-272.
- Brenner BM, Cooper ME, de Zeeuw D, et al. Effects of losartan on renal and cardiovascular outcomes in patients with type 2 diabetes and nephropathy (RENAAL trial). New England Journal of Medicine. 2001;345(12):861-869.
- Lewis EJ, Hunsicker LG, Clarke WR, et al. Renoprotective effect of the angiotensin-receptor antagonist irbesartan in patients with nephropathy due to type 2 diabetes (IDNT trial). New England Journal of Medicine. 2001;345(12):851-860.
- Perkovic V, Jardine MJ, Neal B, et al. Canagliflozin and renal outcomes in type 2 diabetes and nephropathy (CREDENCE trial). New England Journal of Medicine. 2019;380(24):2295-2306.
- Heerspink HJL, Stefansson BV, Correa-Rotter R, et al. Dapagliflozin in patients with chronic kidney disease (DAPA-CKD trial). New England Journal of Medicine. 2020;383(15):1436-1446.
- National Kidney Foundation. K/DOQI clinical practice guidelines for chronic kidney disease: evaluation, classification, and stratification. American Journal of Kidney Diseases. 2002;39(2 Suppl 1):S1-266.
- KDIGO CKD Work Group. KDIGO 2024 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney International. 2024;105(4S):S117-S314.
- GBD Chronic Kidney Disease Collaboration. Global, regional, and national burden of chronic kidney disease, 1990-2017. The Lancet. 2020;395(10225):709-733.
- Bakris GL, Agarwal R, Anker SD, et al. Effect of finerenone on chronic kidney disease outcomes in type 2 diabetes (FIDELIO-DKD trial). New England Journal of Medicine. 2020;383(23):2219-2229.
- Go AS, Chertow GM, Fan D, et al. Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. New England Journal of Medicine. 2004;351(13):1296-1305.
Research Papers
Explore current literature on chronic kidney disease via PubMed topic searches. These links open live PubMed searches for the listed keywords — results update as new studies are indexed.
- Clinical trials on chronic kidney disease — PubMed search
- Clinical trials on diabetic nephropathy — PubMed search
- Clinical trials on SGLT2 inhibitors kidney — PubMed search
- Clinical trials on CKD progression — PubMed search
- Clinical trials on end-stage renal disease dialysis — PubMed search
- Clinical trials on kidney transplantation — PubMed search
- Clinical trials on KDIGO CKD guidelines — PubMed search
Connections
- Nephrology & Hepatology
- How Your Body Makes Red Blood Cells (EPO) — interactive animation
- SGLT2: Why Diabetes Drugs Make You Pee Sugar — interactive animation
- Blood pH: The Acid–Base Balancing Act — interactive animation
- How Your Body Controls Blood Pressure — interactive animation
- Kidney Nephron — interactive animation
- Pyelonephritis (Kidney Infection)
- Deep Dives: eGFR & Staging · Kidney-Friendly Diet · Slowing Progression · Diabetic Kidney Disease · Dialysis & Transplant · History & Discovery
- Beans for Kidney Health
- Glomerulonephritis
- Acute Kidney Injury
- Nephrotic Syndrome
- Diabetes
- Hypertension
- Potassium
- Magnesium
- Vitamin D3
- Comprehensive Metabolic Panel
- eGFR
- Creatinine
- Kidney Function Tests
- Anemia
- Osteoporosis
- Turmeric
- Lupus
- Edema
- Lead
- Kidney Cancer
- Diabetic Retinopathy
- Polycystic Kidney Disease