Phosphorus – Essential Mineral for Human Health
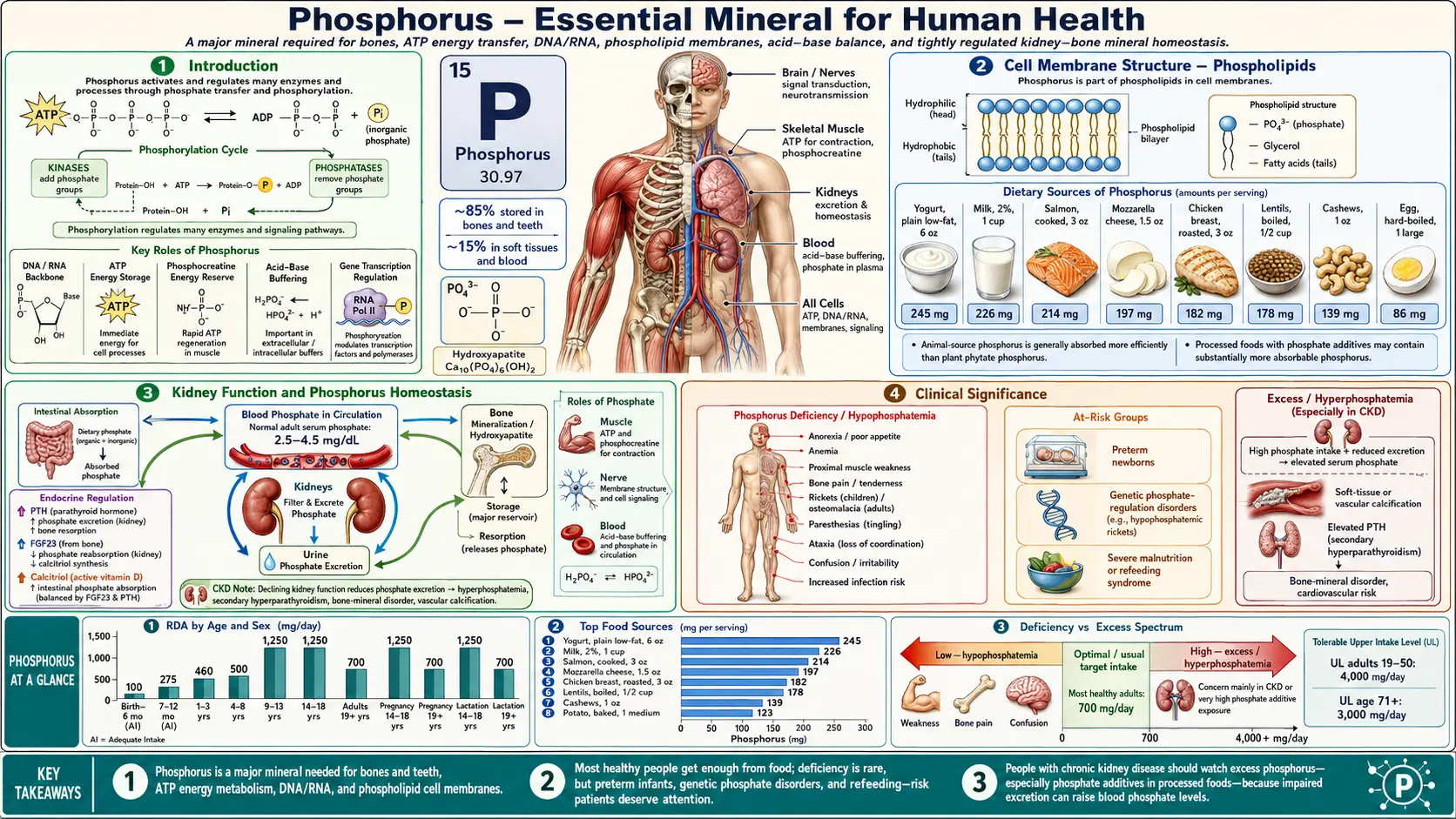

Table of Contents
- Introduction
- Bone and Teeth Structure
- Energy Metabolism – ATP and ADP
- Nucleic Acid Structure – DNA and RNA
- Cell Membrane Structure – Phospholipids
- Acid-Base Buffering
- Enzyme Activation – Phosphorylation
- Kidney Function and Phosphorus Homeostasis
- B Vitamin Activation
- Muscle Function
- Cell Signaling
- Clinical Significance
- Connections
Introduction
- Phosphorus is the second most abundant mineral in the human body after calcium, comprising approximately 1% of total body weight (600–700 grams in an adult).
- Approximately 85% of body phosphorus resides in bones and teeth as calcium phosphate salts, with the remaining 15% distributed in soft tissues and extracellular fluid.
- Phosphorus participates in more biological processes than any other mineral, including energy metabolism, structural integrity, genetic information storage, signal transduction, acid-base balance, and enzyme regulation.
- In the body, phosphorus exists primarily as phosphate (PO₄³⁻) in its various protonation states (H₂PO₄⁻ and HPO₄²⁻ at physiological pH).
- The recommended dietary allowance (RDA) for adults is 700 mg per day. Dietary sources include dairy products, meat, fish, poultry, legumes, nuts, and whole grains.
Bone and Teeth Structure
- Hydroxyapatite [Ca₁₀(PO₄)₆(OH)₂] is the principal mineral crystal of bone and tooth enamel. Phosphorus is an indispensable structural component, comprising approximately 50% of bone mineral by weight.
- Calcium phosphate deposition occurs on a collagen matrix during bone mineralization. Osteoblasts secrete alkaline phosphatase, which cleaves pyrophosphate (an inhibitor of mineralization) and increases local phosphate concentration to promote crystal formation.
- Both hypophosphatemia (low serum phosphate) and hyperphosphatemia (high serum phosphate) severely disrupt skeletal health. Hypophosphatemia causes rickets in children and osteomalacia in adults due to inadequate mineralization. Hyperphosphatemia drives secondary hyperparathyroidism and renal osteodystrophy.
- Tooth enamel contains a denser form of hydroxyapatite than bone. Fluorapatite, formed when fluoride substitutes into the crystal, is more resistant to acid dissolution, which is the basis for fluoride's cariostatic effect.
- The calcium-to-phosphorus ratio in the diet influences bone metabolism. Excessive phosphorus intake relative to calcium can increase parathyroid hormone secretion and promote bone resorption.
Energy Metabolism – ATP and ADP
- Adenosine triphosphate (ATP) is the universal energy currency of the cell. It contains three phosphate groups linked by high-energy phosphoanhydride bonds, each releasing approximately 7.3 kcal/mol of free energy upon hydrolysis.
- Hydrolysis of ATP to ADP (adenosine diphosphate) and inorganic phosphate (Pi) provides the energy that drives muscle contraction, active transport across membranes, biosynthetic reactions, and signal transduction.
- Further hydrolysis of ADP to AMP (adenosine monophosphate) and Pi provides additional energy for high-demand processes.
- GTP, UTP, and CTP are additional phosphorylated nucleotides that serve specialized energy-transfer functions in protein synthesis, glycogen synthesis, and lipid synthesis, respectively.
- The human body turns over its own weight in ATP approximately every day, underscoring the enormous demand for phosphate in energy metabolism.
Nucleic Acid Structure – DNA and RNA
- Phosphodiester bonds form the backbone of both DNA and RNA, linking the 3' carbon of one sugar to the 5' carbon of the next through a phosphate group. Without phosphorus, no nucleic acid polymer can be assembled.
- The negative charge of the phosphate backbone is essential for the structural stability of the double helix, interaction with histone proteins in chromatin, and binding of regulatory proteins to DNA.
- RNA molecules (mRNA, tRNA, rRNA, and regulatory RNAs) all require phosphodiester linkages. Given the high turnover of RNA in active cells, phosphorus demand for nucleic acid synthesis is substantial.
- Nucleotide synthesis (both de novo and salvage pathways) requires multiple phosphorylation steps, utilizing ATP and other phosphorylated donors. Phosphoribosyl pyrophosphate (PRPP) is a critical phosphorylated intermediate in both purine and pyrimidine biosynthesis.
Cell Membrane Structure – Phospholipids
- Phospholipids are the primary structural components of all biological membranes. They consist of a glycerol backbone esterified with two fatty acids and a phosphate group linked to a polar head group.
- Major membrane phospholipids include phosphatidylcholine, phosphatidylethanolamine, phosphatidylserine, phosphatidylinositol, and sphingomyelin. Each has distinct biophysical properties and signaling functions.
- The phosphate head group confers the amphipathic character essential for bilayer formation. The hydrophilic phosphate faces the aqueous environment while the hydrophobic fatty acid tails form the membrane interior.
- Phosphatidylinositol and its phosphorylated derivatives (PIP, PIP₂, PIP₃) are critical signaling molecules. Phospholipase C cleavage of PIP₂ generates the second messengers inositol trisphosphate (IP₃) and diacylglycerol (DAG), which mediate calcium release and protein kinase C activation, respectively.
- Phosphatidylserine exposure on the outer leaflet of the plasma membrane serves as an "eat-me" signal for phagocytic clearance of apoptotic cells, a phosphorus-dependent process essential for tissue homeostasis.
Acid-Base Buffering
- The phosphate buffer system (H₂PO₄⁻ / HPO₄²⁻) is the principal intracellular buffering system and an important urinary buffer.
- With a pKa of 6.8, the phosphate buffer system operates near physiological intracellular pH (approximately 7.0–7.2), making it highly effective at resisting intracellular pH changes.
- In the kidneys, phosphate serves as a titratable acid. Filtered phosphate accepts secreted hydrogen ions in the renal tubule, forming H₂PO₄⁻ that is excreted in urine. This mechanism accounts for a significant portion of daily renal acid excretion.
- The phosphate buffer system complements the bicarbonate buffer system (the dominant extracellular buffer) and the protein/hemoglobin buffer systems in maintaining overall acid-base homeostasis.
Enzyme Activation – Phosphorylation
- Protein phosphorylation is the most prevalent post-translational modification in eukaryotic cells. Approximately one-third of all human proteins are phosphorylated at any given time.
- Protein kinases transfer the terminal (gamma) phosphate from ATP to serine, threonine, or tyrosine residues on target proteins. The human genome encodes over 500 protein kinases (the "kinome"), reflecting the extraordinary importance of this regulatory mechanism.
- Protein phosphatases remove phosphate groups, reversing kinase activity. The dynamic balance between kinase and phosphatase activity enables rapid, reversible regulation of virtually every cellular process.
- Phosphorylation regulates enzyme activity (activation or inhibition), protein-protein interactions, subcellular localization, and protein stability. Classic examples include glycogen phosphorylase (activated by phosphorylation), glycogen synthase (inactivated by phosphorylation), and pyruvate dehydrogenase (inactivated by phosphorylation).
- Receptor tyrosine kinases (EGFR, insulin receptor, PDGFR, VEGFR) initiate signaling cascades through autophosphorylation, triggering downstream pathways (RAS-MAPK, PI3K-AKT, JAK-STAT) that control cell growth, differentiation, survival, and metabolism.
Kidney Function and Phosphorus Homeostasis
- The kidneys are the primary regulators of phosphorus homeostasis. Approximately 80–90% of filtered phosphate is reabsorbed in the proximal tubule via sodium-phosphate cotransporters (NaPi-IIa and NaPi-IIc).
- Parathyroid hormone (PTH) decreases renal phosphate reabsorption by promoting internalization and degradation of NaPi-IIa transporters, resulting in phosphaturia. PTH is secreted in response to hypocalcemia and hyperphosphatemia.
- Fibroblast growth factor 23 (FGF23), produced by osteocytes, is a major phosphaturic hormone. It reduces renal phosphate reabsorption and suppresses 1,25-dihydroxyvitamin D synthesis, providing a bone-kidney feedback loop for phosphate regulation.
- 1,25-Dihydroxyvitamin D (calcitriol) increases intestinal phosphorus absorption and, to a lesser extent, renal reabsorption. Its synthesis is stimulated by PTH and suppressed by FGF23.
- Chronic kidney disease (CKD) progressively impairs phosphate excretion, leading to hyperphosphatemia, secondary hyperparathyroidism, renal osteodystrophy, and vascular calcification – a major contributor to cardiovascular mortality in CKD patients.
B Vitamin Activation
- Several B vitamins require phosphorylation to become metabolically active coenzymes, making phosphorus essential for their function.
- Thiamine (B1) is converted to thiamine pyrophosphate (TPP), the active coenzyme for pyruvate dehydrogenase, alpha-ketoglutarate dehydrogenase, and transketolase.
- Riboflavin (B2) is phosphorylated to form flavin mononucleotide (FMN) and further converted to flavin adenine dinucleotide (FAD), both essential electron carriers in oxidative metabolism.
- Niacin (B3) is incorporated into nicotinamide adenine dinucleotide (NAD⁺) and its phosphorylated form NADP⁺, both of which contain multiple phosphate groups and are central to hundreds of redox reactions.
- Pyridoxine (B6) is converted to pyridoxal 5'-phosphate (PLP), the active coenzyme required for over 140 enzymatic reactions including amino acid transamination, decarboxylation, and neurotransmitter synthesis.
- Pantothenic acid (B5) is incorporated into coenzyme A (CoA), which contains an ADP moiety with phosphate groups. CoA is essential for fatty acid oxidation, the citric acid cycle, and acetylation reactions.
Muscle Function
- ATP hydrolysis directly powers the myosin cross-bridge cycle in skeletal, cardiac, and smooth muscle. Without adequate phosphate for ATP regeneration, sustained muscle contraction is impossible.
- Creatine phosphate (phosphocreatine) serves as a rapidly mobilizable phosphate reserve in muscle. Creatine kinase transfers the phosphate group from phosphocreatine to ADP, regenerating ATP within seconds during high-intensity exercise.
- Calcium-ATPase (SERCA) in the sarcoplasmic reticulum uses ATP hydrolysis to pump calcium back into the SR after contraction, enabling muscle relaxation. This is a phosphorus-dependent process.
- Severe hypophosphatemia (serum phosphate below 1.0 mg/dL) can cause acute rhabdomyolysis, respiratory muscle failure, and cardiac dysfunction due to ATP depletion in muscle cells.
- 2,3-Bisphosphoglycerate (2,3-BPG) is a phosphorylated intermediate in erythrocytes that modulates hemoglobin oxygen affinity. Phosphate depletion reduces 2,3-BPG levels, shifting the oxygen dissociation curve leftward and impairing oxygen delivery to exercising muscles and other tissues.
Cell Signaling
- Cyclic AMP (cAMP) and cyclic GMP (cGMP) are phosphorylated second messengers derived from ATP and GTP, respectively. cAMP mediates the intracellular effects of numerous hormones including epinephrine, glucagon, ACTH, and TSH.
- Phosphoinositide signaling involves the sequential phosphorylation of phosphatidylinositol by PI3-kinase and other lipid kinases to generate PIP₂ and PIP₃, which recruit and activate downstream effectors such as AKT/protein kinase B, a master regulator of cell survival and metabolism.
- GTP-binding proteins (G proteins) act as molecular switches by cycling between GDP-bound (inactive) and GTP-bound (active) states. This phosphorus-dependent mechanism controls vision (transducin), neurotransmission, cell proliferation (RAS), vesicle trafficking (RAB proteins), and cytoskeletal dynamics (RHO/RAC).
- Phosphorylation cascades (e.g., the MAP kinase pathway: RAS → RAF → MEK → ERK) amplify extracellular signals and integrate multiple inputs to produce coordinated cellular responses. Dysregulation of these phosphorus-dependent pathways is a hallmark of cancer.
- ATP and its metabolites (ADP, AMP, adenosine) also serve as extracellular signaling molecules through purinergic receptors (P2X, P2Y, P1), mediating neurotransmission, platelet aggregation, immune regulation, and vasodilation.
Clinical Significance
Both too little and too much phosphate cause serious problems. Low phosphate (hypophosphatemia) arises from refeeding syndrome, chronic alcoholism, vitamin D deficiency, and renal wasting, and in severe cases can trigger muscle breakdown, respiratory failure, and cardiac dysfunction. High phosphate (hyperphosphatemia) is most common in chronic kidney disease and drives vascular calcification, secondary hyperparathyroidism, and renal osteodystrophy. For a full, patient-friendly guide to the symptoms, causes, and treatment, see Hypophosphatemia (Low Phosphate) and Hyperphosphatemia (High Phosphate).
Connections
- Hypophosphatemia (Low Phosphate)
- Hyperphosphatemia (High Phosphate)
- Phosphorus Benefits Deep Dive
- Phosphorus for Energy Production
- Phosphorus for Bone Mineralization
- Phosphorus for Cell Membranes
- Phosphorus for Acid-Base Balance
- Calcium
- Magnesium
- Kidney Function Tests
- Hyperparathyroidism
- Creatine
- Collagen
- Vitamin D3
- Vitamin K
- Osteoporosis
- Kidney Disease
- Potassium
- Iron
- Manganese
- Boron
- eGFR
- Cardiovascular Disease
- Eggs
- Beans for Kidney Health — why the phytate-bound phosphorus in beans is absorbed far less than phosphate additives.