Fibromyalgia

Deep-Dive Articles
Central Sensitization Explained
Why the nervous system amplifies pain in fibromyalgia — nociplastic pain, the volume knob analogy, and what this means for treatment choices.
ACR 2016 Diagnostic Criteria
The Widespread Pain Index + Symptom Severity score replaced tender points in 2016. How clinicians actually diagnose fibromyalgia today.
Sleep & Non-Restorative Sleep
Alpha intrusion on EEG, stage N3 deficits, and why fixing sleep is often the highest-yield intervention. Sleep study interpretation, CPAP, and bedtime protocols.
Low-Dose Naltrexone (LDN)
Evidence, dosing (1.5-4.5 mg), titration schedules, compounding pharmacies, and what to expect in the first 8 weeks.
Exercise Pacing & Graded Movement
Why generic "push through it" advice backfires. Heart-rate-capped aerobic work, aquatic therapy, resistance training, and the pacing envelope.
Nutrient Gaps: Mg, D, B12
The nutrient deficiencies most consistently linked to fibro severity — magnesium, vitamin D, B12, and iron/ferritin — with target lab ranges and repletion protocols.
Small-Fiber Neuropathy Overlap
Around half of fibromyalgia patients have objective small-fiber neuropathy on skin biopsy. What this means for workup (skin biopsy, QSART) and treatment.
Fibromyalgia & ME/CFS Overlap
Where the two diagnoses converge and diverge, post-exertional malaise, the "fibromyalgia plus fatigue" phenotype, and why the distinction changes treatment.
Cannabis, CBD & Medical Marijuana
Endocannabinoid deficiency, THC:CBD ratios, dosing, and real-world evidence.
Table of Contents
- Deep-Dive Articles
- What Fibromyalgia Actually Is
- The Science: Central Sensitization
- Diagnosis: The 2016 ACR Criteria
- Symptoms Beyond Pain
- Fibro Fog: Cognitive Dysfunction
- Overlapping Conditions
- Treatment: What Actually Works
- Exercise: The Strongest Evidence
- Talking Therapies, Sleep and Pacing
- Medications
- Diet and Supplements: An Honest Look
- What Is Not Supported
- Living with Fibromyalgia
- Important Cautions
- Key Research Papers
- Connections
- Featured Videos
What Fibromyalgia Actually Is
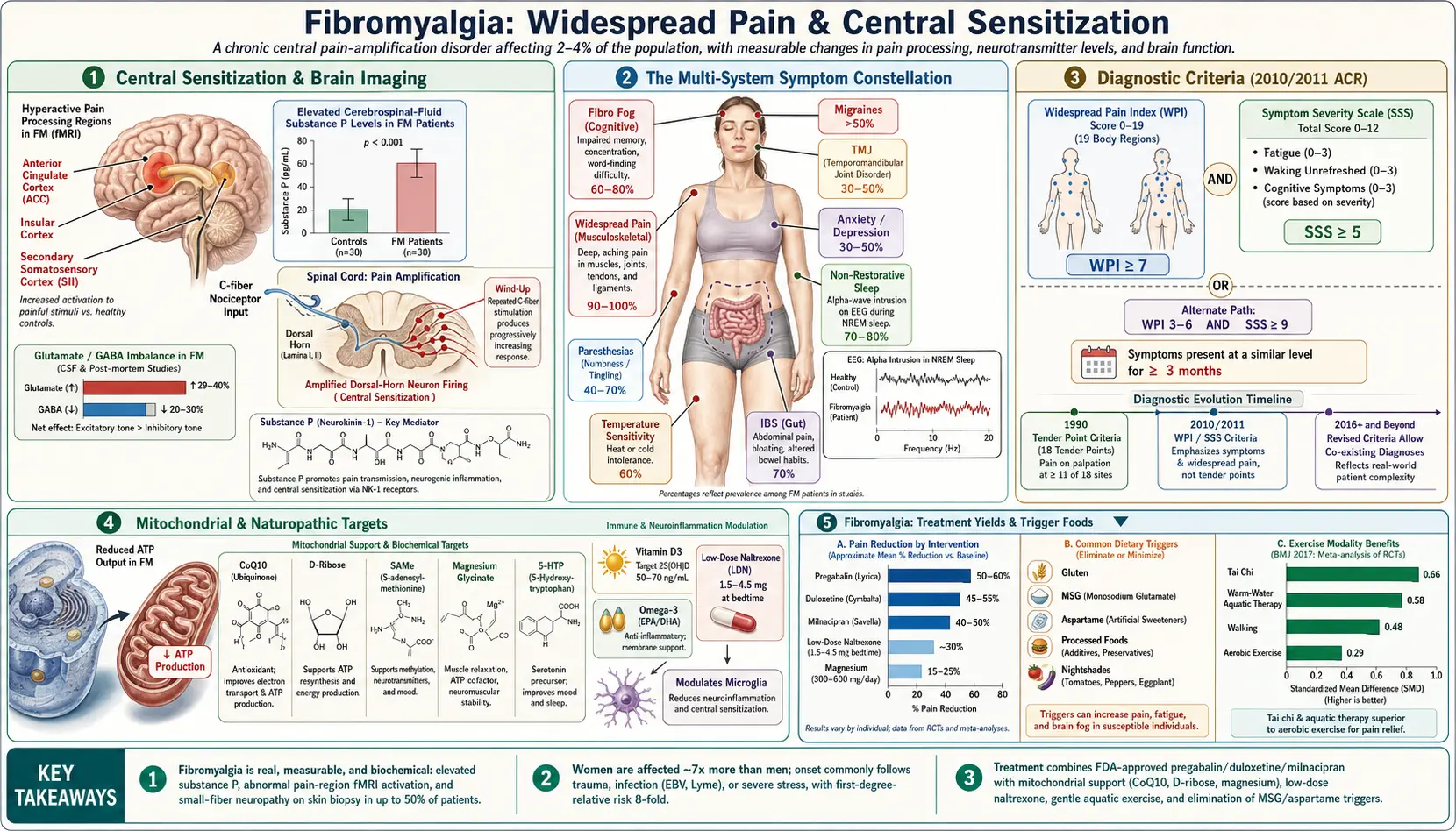
Fibromyalgia is a disorder of pain processing. The problem is not in your muscles or your joints — it is in the way your brain and spinal cord handle pain signals. The nervous system has turned its volume up and left it there. Ordinary sensations that should register as pressure, warmth or movement get amplified into pain before they ever reach conscious awareness.
Pain researchers call this central sensitization, and the resulting pain has a formal name: nociplastic pain. It sits alongside the two older categories — nociceptive pain (from tissue damage, like a broken bone) and neuropathic pain (from nerve damage, like sciatica). Nociplastic pain is real pain generated by a real, measurable change in a real organ. That organ happens to be the nervous system.
Let us be plain about what fibromyalgia is not, because patients are routinely disbelieved and the misinformation does genuine harm:
- It is not inflammation. CRP, ESR and every other standard inflammatory marker come back normal. This is precisely why anti-inflammatory drugs do so little.
- It is not autoimmune. There is no autoantibody, no immune attack on your tissue, and no progressive destruction of joints or organs.
- It is not degenerative. Fibromyalgia does not damage your body over time. It is miserable, but it is not destroying you.
- It is not "in your head" — not in the dismissive sense people mean when they say it. The pain does not originate in your imagination, your personality, or a wish for attention.
That last point deserves more than a bullet. If you have been told your pain is not real, or that your tests are normal so nothing is wrong, you were told something false. The abnormality in fibromyalgia is simply not the kind a blood test or an X-ray is designed to find. When researchers do look in the right place, they find it every time:
- Measurably lower pain thresholds. Under quantitative sensory testing, pressure that healthy volunteers describe as merely firm is reported as painful by people with fibromyalgia — and their brains light up accordingly on functional MRI. The scanner does not know who is "supposed" to be in pain.
- Amplified central signalling. Cerebrospinal fluid studies find substance P — a pain-transmitting neuropeptide — elevated to roughly two to three times normal levels. Brain glutamate, the main excitatory neurotransmitter, is elevated in the insula, and the higher it runs, the more pain a person reports.
- Altered brain connectivity. The default mode network — the brain's idling circuitry — is abnormally wired into the insula, a key pain-processing hub. The strength of that connection tracks how much pain a person is in.
None of that is subtle, and none of it is psychological. Your pain has a neurological signature. It is the amplifier that is broken, not the person.
How common is it? Fibromyalgia affects roughly 2 to 4 percent of the population, making it one of the most common chronic pain conditions in medicine. It is more common in women, though by how much is genuinely contested: the old figure of "seven to nine times more common in women" came from the 1990 tender-point criteria, and the tender-point exam itself selected for women, who are on average more tender to pressure. Studies using the modern symptom-based criteria find a much narrower gap — closer to 2:1 or 3:1 — which suggests fibromyalgia in men has been substantially underdiagnosed for decades. It can begin at any age, including childhood, but most often appears between the ages of 30 and 55. Many patients can name a trigger — an injury, an operation, an infection, a bereavement, a period of severe stress — though plenty cannot, and the absence of a trigger means nothing.
The Science: Central Sensitization
If you take away one mechanism, take this one: in fibromyalgia the pain system amplifies its own signal and then fails to switch the amplification off. Here is how that happens, layer by layer.
Wind-Up in the Spinal Cord
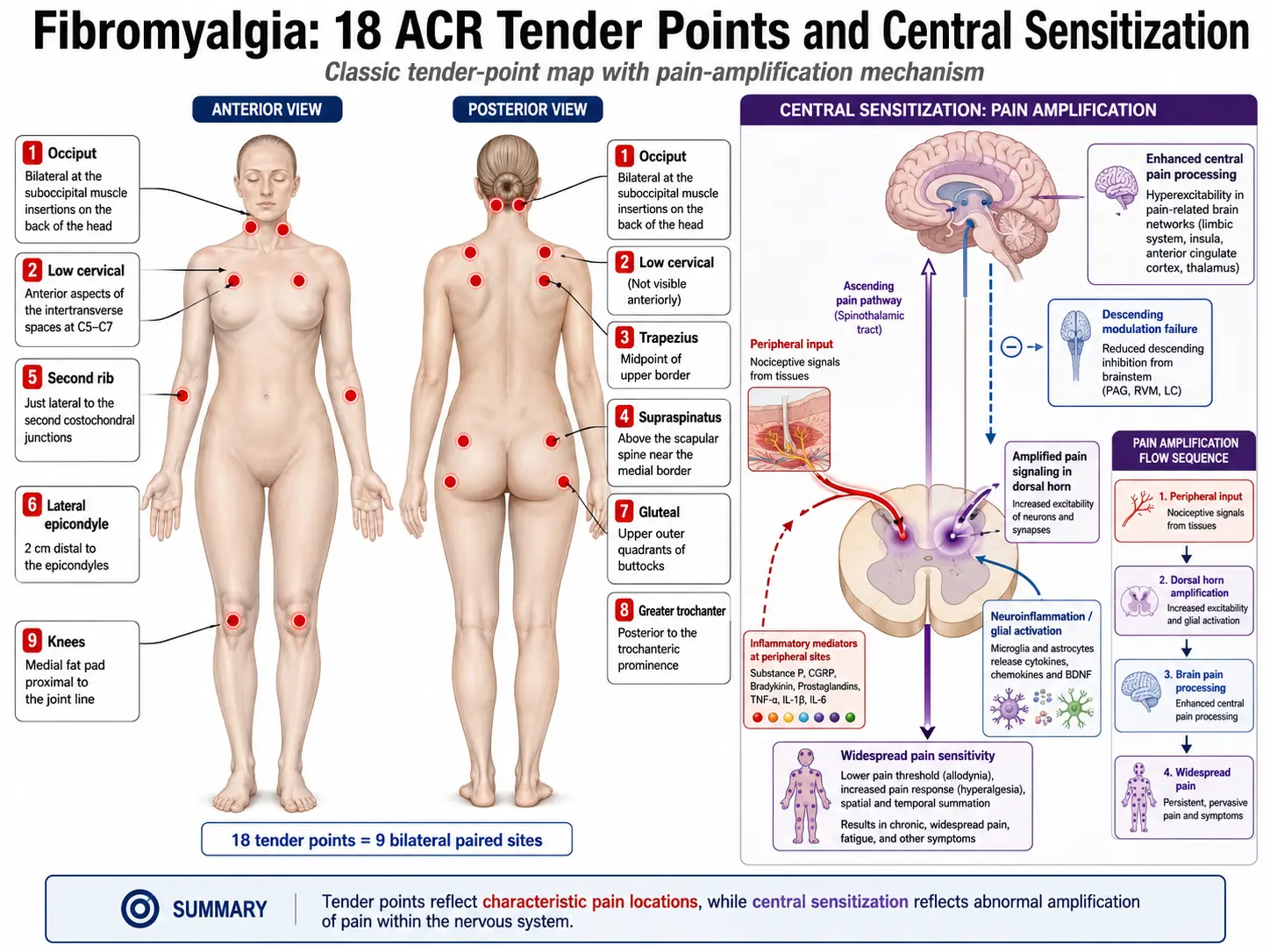
Pain signals from the body arrive first at the dorsal horn of the spinal cord, where they hand off to a second nerve cell that carries the message up to the brain. Repeated input makes that second cell progressively more excitable — it starts firing harder in response to the same stimulus. Neurologists call this wind-up. NMDA receptors get recruited, glutamate release climbs, and the threshold for transmitting pain drops.
In most people wind-up is temporary and settles once the input stops. In fibromyalgia it becomes self-sustaining. The amplifier keeps running after the original signal is long gone — which is exactly why hunting for the "hidden injury" that must be causing the pain is usually a dead end. There often isn't one anymore.
The Brakes Fail
Your brain does not just receive pain — it actively suppresses it. Descending pathways run from the periaqueductal gray and the brainstem back down the spinal cord, damping incoming signals before they ever surface. Those brakes run on serotonin and norepinephrine.
In fibromyalgia the braking system underperforms. This is not a side note — it is the single most practically useful fact on this page, because it explains why the drugs that work in fibromyalgia are the ones that boost serotonin and norepinephrine (duloxetine, milnacipran, amitriptyline), and why the drugs that target inflammation do essentially nothing. The problem is a failure of inhibition, so the treatments that help are the ones that restore inhibition.
Excitatory Chemistry Runs Hot
Cerebrospinal fluid studies consistently find substance P elevated two- to three-fold in fibromyalgia. Nerve growth factor is elevated too. Brain imaging spectroscopy finds raised glutamate in the insula, and the level correlates with how much experimental pain a person feels. Accelerator up, brakes down.
Glial Activation: Neuroinflammation Without Inflammation
Microglia are the immune cells of the central nervous system. In fibromyalgia they appear to shift into an activated, inflammatory state, releasing cytokines that sensitize the neurons around them.
This is worth stating carefully, because it is easy to misread. This is neuroinflammation confined to the nervous system — it does not show up as inflammation in your blood, and it does not make fibromyalgia an inflammatory disease in the way rheumatoid arthritis is. Your CRP will still be normal. What it does explain is why a drug like low-dose naltrexone, which quiets microglia, is a plausible treatment while ibuprofen is not.
Rewired Brain Connectivity
Functional MRI shows increased connectivity between the default mode network and the insula, and the strength of that abnormal connection tracks clinical pain intensity. Gentle pressure that produces no pain and no brain response in a healthy volunteer produces both in a person with fibromyalgia. Mechanistically, fibromyalgia is a disorder of how the brain interprets sensation.
The Peripheral Twist: Small-Fiber Neuropathy
The "purely central" story turned out to be incomplete. In 2013, two independent groups took skin punch biopsies from fibromyalgia patients and found reduced density of small nerve fibers — objective, visible-under-a-microscope small-fiber neuropathy — in roughly 40 to 50 percent of them.
This matters for two reasons. First, it is more hard evidence that fibromyalgia is a physical disease. Second, it suggests fibromyalgia is not one thing: there is likely a substantial subgroup in whom damaged peripheral nerves are feeding the central amplifier. If your fibromyalgia comes with prominent burning, numbness or tingling, this subgroup is worth asking your neurologist about — a skin biopsy is a real test with a real answer.
Sleep: Both Symptom and Engine
Non-restorative sleep is nearly universal in fibromyalgia, and it is not merely a consequence of hurting at night. Sleep studies show alpha-wave intrusion into deep delta sleep — the brain repeatedly flickering toward wakefulness without the person actually waking — and a shortage of restorative stage N3 sleep.
The direction of causation runs both ways, which was demonstrated as far back as 1975: deliberately depriving healthy volunteers of deep sleep produced fibromyalgia-like musculoskeletal pain and tenderness. Poor sleep amplifies pain; pain wrecks sleep; the loop tightens. It also means that fixing sleep is a genuine treatment for pain, not just a comfort measure — which is why sleep gets its own section below.
Diagnosis: The 2016 ACR Criteria
Fibromyalgia is a positive clinical diagnosis. It is diagnosed by recognising a characteristic pattern — not by ruling out everything else until nothing is left. This is a genuine change from how the condition was taught for decades, and it matters: "diagnosis of exclusion" thinking is what sends patients through years of scans and specialist referrals that were never going to find anything.
There is no blood test and no scan for fibromyalgia. That is not a gap in the workup; it is a feature of what the condition is.
The Obsolete Tender-Point Exam
The 1990 ACR criteria required a doctor to press on 18 designated body sites with about 4 kg of pressure — roughly the force that blanches a fingernail — and find tenderness in at least 11 of them, alongside widespread pain lasting three months.
This exam is obsolete and should no longer be used to diagnose fibromyalgia. It was abandoned because it was unreliable between examiners, because tenderness fluctuates day to day, because it was never designed as a diagnostic tool (it was a research classification tool), and because it wrongly excluded large numbers of genuine patients — particularly men. If a clinician tells you that you cannot have fibromyalgia because you failed a tender-point count, that clinician is working from a standard that was replaced in 2010.
What Replaced It: WPI + SS
The 2010 criteria, revised in 2016, are based on two things you report — not on what a doctor can feel.
The Widespread Pain Index (WPI) is a simple count. Of 19 defined body areas, how many hurt in the last week? The areas are: left and right jaw, shoulder girdle, upper arm, lower arm, hip/buttock, upper leg and lower leg (that is seven pairs), plus neck, upper back, lower back, chest and abdomen. Score: 0 to 19.
The Symptom Severity scale (SS) rates three core symptoms — fatigue, waking unrefreshed, and cognitive symptoms — from 0 (none) to 3 (severe). That gives 0 to 9. Then 0 to 3 more points are added for the burden of other somatic symptoms (headaches, lower abdominal pain or cramps, depression). Total: 0 to 12.
You meet criteria for fibromyalgia when all three of the following are true:
- WPI ≥ 7 and SS ≥ 5, or WPI 4–6 and SS ≥ 9.
- Pain is generalized: present in at least 4 of 5 body regions (upper left, upper right, lower left, lower right, and axial).
- Symptoms have been present at roughly this level for at least 3 months.
Two points about the 2016 revision are easy to miss and both are liberating. First, fibromyalgia does not exclude any other diagnosis. You can have fibromyalgia and rheumatoid arthritis, and lupus, and osteoarthritis — and many people do. Having another condition does not disqualify you, and getting the fibromyalgia diagnosis does not mean your other condition was imaginary. Second, the diagnosis is valid regardless of what caused it. You do not need a trigger, and you do not need to justify it.
The Mimics: What Should Be Screened For
A positive diagnosis is not the same as no workup. Several treatable conditions produce widespread pain and fatigue that look very like fibromyalgia, and it would be a shame to spend a decade managing "fibromyalgia" that was actually a vitamin deficiency. A reasonable screen covers:
- Hypothyroidism — an underactive thyroid causes widespread aching, profound fatigue, cold intolerance and cognitive slowing. Check TSH. This is the classic mimic and it is trivially treatable.
- Vitamin D deficiency — can cause diffuse musculoskeletal pain and proximal muscle weakness in its own right. Check 25-hydroxyvitamin D.
- Polymyalgia rheumatica — in patients over about 50, with shoulder and hip girdle stiffness that is dramatically worse in the morning, and a raised ESR/CRP. It responds to low-dose steroids almost overnight; fibromyalgia does not.
- Inflammatory arthritis — rheumatoid arthritis, psoriatic arthritis, ankylosing spondylitis. Look for genuinely swollen joints, morning stiffness lasting over an hour, and raised inflammatory markers. Note the trap: you can have both, and unrecognised fibromyalgia on top of RA is a common reason a patient's RA appears "uncontrolled" despite quiet joints.
- Obstructive sleep apnoea — grossly underdiagnosed in fibromyalgia and a direct driver of unrefreshing sleep, fatigue and pain. If you snore, wake gasping, or wake exhausted after eight hours in bed, push for a sleep study. Treating apnoea can substantially reduce pain.
- Vitamin B12 deficiency — causes fatigue, cognitive fog, and paraesthesias. Easily checked, easily corrected.
- Others worth a thought — anaemia, coeliac disease, hepatitis C, and (rarely) myositis or lupus, guided by symptoms.
A sensible baseline panel is: full blood count, CRP and ESR, TSH, 25-hydroxyvitamin D, B12, and a basic metabolic panel. If those are unremarkable and the WPI/SS pattern fits, that is the diagnosis — you do not need to keep searching.
Symptoms Beyond Pain
The name focuses on pain, but ask any patient which symptom they would delete first and a great many say fatigue or the fog. Fibromyalgia is a multi-system condition, and the four core features are widespread pain, profound fatigue, non-restorative sleep, and cognitive dysfunction.
- Widespread pain. Deep, aching, burning; migrating from place to place; worse with cold, stress and weather change. Often accompanied by allodynia (things that should not hurt do — a waistband, a hug, a bedsheet) and hyperalgesia (things that should hurt a little hurt a lot).
- Profound fatigue. Not ordinary tiredness. A heavy, whole-body exhaustion that rest does not fix — many people describe waking as if they had been "hit by a truck", or run over and then run over again.
- Non-restorative sleep. You sleep, and it does not count. Eight hours in bed and you wake as though you had two. See the mechanism above: this is the alpha-intrusion pattern, and it feeds the pain directly.
- Cognitive dysfunction ("fibro fog"). Its own section, below.
- Morning stiffness — sometimes lasting hours, easing with gentle movement.
- Headache and migraine — chronic tension-type headache and migraine are several times more common than in the general population.
- Irritable bowel symptoms — bloating, abdominal pain, alternating constipation and diarrhoea, in a large fraction of patients.
- Paraesthesias — numbness, tingling, pins-and-needles, burning, particularly in hands and feet. In some people this reflects the small-fiber neuropathy described above.
- Sensory overwhelm — the amplifier is not pain-specific. Bright light, loud noise, strong smells and crowded spaces can become genuinely intolerable. Supermarkets are a common nemesis.
- Temperature dysregulation — poor tolerance of both cold and heat.
- Autonomic symptoms — light-headedness on standing, palpitations, dry eyes and mouth.
- Mood disturbance — depression and anxiety are considerably more common than in the general population. Read the next paragraph carefully.
On mood, and on the order of causation. Depression and anxiety are common in fibromyalgia, and this fact has been weaponised against patients for decades — as if a low mood proved the pain was psychosomatic. It does not. Two things are true at once: living with unrelenting pain, exhaustion and disbelief is itself depressing, and the same serotonin and norepinephrine pathways that regulate mood are the ones that regulate descending pain inhibition. Shared neurochemistry, shared symptoms. Depression is not the cause of fibromyalgia, and plenty of people have fibromyalgia with no mood disorder at all. But it is worth treating when it is there — not to prove anything, but because it lowers the pain threshold and makes everything else harder.
Fibro Fog: Cognitive Dysfunction
"Fibro fog" is the patient's word for it, and it covers a specific cluster: trouble concentrating, losing words mid-sentence, short-term memory lapses, slowed thinking, and an inability to hold two tasks in mind at once. People describe it as thinking through treacle, or as having the mental bandwidth of a much older person on a bad day.
It is measurable. This is not patients being vague about being tired. On formal neuropsychological testing, people with fibromyalgia show real deficits in processing speed, working memory and attention against healthy controls. On functional MRI during cognitive tasks, the prefrontal cortex — the brain's executive controller — shows reduced engagement. The subjective experience of mental sluggishness has an objective correlate.
What drives it. Fog severity tracks most closely with sleep quality and pain intensity. That is good news disguised as a mechanism: it means fog is not a fixed, separate disease process to be endured, but a downstream consequence of two things that can be worked on. Pain consumes cognitive resources — a brain that is busy processing pain has less capacity left for finding the word "colander".
What actually helps:
- Fix sleep first. The single highest-yield intervention. Even modest improvements in sleep quality tend to produce noticeable gains in clarity.
- Bring the pain down. Any route that works — the cognitive benefit follows.
- Pace cognitive work like physical work. Fog has a boom-bust cycle too. Space demanding tasks; rest deliberately between them; do the hard thinking in your best hours.
- Cut the sensory load. Background noise, competing screens and multitasking demands all consume the bandwidth you are short of. A quiet room is a cognitive intervention.
- Externalise your working memory. Lists, alarms, notes, calendars. Stop trying to win a fight against a system that is currently under-resourced — offload it instead. This is not defeat; it is engineering.
- Audit your medications. Anticholinergic drugs — including amitriptyline at higher doses — can worsen cognition. If your fog got noticeably worse after starting a drug, that is worth raising; a dose reduction or a switch may buy back clarity.
Overlapping Conditions
Fibromyalgia rarely arrives alone. It belongs to a family of conditions — sometimes called the central sensitivity syndromes — that share the same underlying feature of amplified sensory processing. Recognising the whole pattern matters, because treating fibromyalgia while ignoring an active, treatable overlap is a common reason management stalls.
- Irritable bowel syndrome (IBS). The most common overlap by far. Estimates vary widely by study and criteria, but a large minority to a majority of fibromyalgia patients have IBS. Same amplification, different nerve supply: visceral hypersensitivity in the gut mirrors somatic hypersensitivity in the body. A low-FODMAP trial often reduces gut symptoms and, in doing so, lowers total pain burden.
- ME/CFS (myalgic encephalomyelitis / chronic fatigue syndrome). The overlap is substantial, and the distinction changes treatment. The discriminating feature is post-exertional malaise — a disproportionate, delayed crash after physical or mental effort. If PEM is prominent, graded exercise must be approached far more cautiously, with strict pacing rather than progressive loading. Getting this wrong causes real harm. See the ME/CFS overlap deep-dive.
- Migraine and chronic headache. Roughly half of patients. The trigeminal pain system is running the same sensitization playbook.
- POTS and dysautonomia. Light-headedness, palpitations and exercise intolerance on standing. Worth screening, because POTS has its own specific management and treating it makes exercise achievable.
- MCAS (mast cell activation syndrome). Flushing, hives, food and chemical sensitivities. Recognised increasingly often alongside fibromyalgia.
- Hypermobility (hEDS / hypermobility spectrum disorder). Connective tissue laxity is over-represented. The proposed cascade runs: lax joints → repeated micro-trauma → chronic peripheral pain input → central sensitization. A Beighton score takes two minutes and is worth doing, especially in younger patients.
- Restless legs syndrome. Several times the population rate, and a further tax on sleep.
- Interstitial cystitis / bladder pain syndrome and temporomandibular disorder (TMD). Both are central sensitization syndromes wearing different clothes.
- Autoimmune disease. Rheumatoid arthritis, lupus, Sjögren's and Hashimoto's thyroiditis coexist with fibromyalgia at elevated rates. Remember: this is an overlap, not a contradiction.
- Depression and anxiety. Common, bidirectional, worth treating. See the note above.
Treatment: What Actually Works
Here is the honest summary, and it is not the one most people expect:
Non-drug treatment is first-line, and it outperforms the drugs. This is not a wellness platitude or a way of fobbing you off with lifestyle advice instead of real medicine. It is the conclusion of the European (EULAR) treatment recommendations, of multiple Cochrane reviews, and of the large meta-analyses of non-pharmacological interventions. Exercise, in particular, beats every licensed drug on the numbers.
To put rough figures on it — and these are approximations from different literatures, so treat them as a sense of scale rather than a league table:
- Graded aerobic exercise — the largest and most consistent effect of any single intervention. Roughly one in three people gets a meaningful reduction in pain, plus gains in function, fatigue and mood that the drugs do not deliver.
- CBT and related talking therapies — small-to-moderate but genuine and durable benefits on pain, function and mood.
- Duloxetine, milnacipran, pregabalin — modest average benefit. Roughly one in four to one in five people gets a clinically meaningful (30%+) pain reduction that they would not have got from placebo. Which means most people who take them do not get that.
- Amitriptyline at low dose — helps a minority, mostly via sleep, and has been in use so long that its evidence base is old and thin by modern standards.
- Opioids — not recommended. See below; this one is important.
Why "modest average benefit" is not the same as "does not work". Fibromyalgia drug trials show a consistent pattern: a minority of people respond well, and everyone else responds barely at all. Averaging those two groups produces an unimpressive mean that describes almost nobody. So the practical approach is a series of honest, time-limited trials — try a drug properly, decide within a couple of months whether you are one of the responders, and if you are not, stop it and try another rather than accumulating a drawer full of medications that are each doing 5% of nothing. Being clear-eyed about this is what keeps you from being both in pain and over-medicated.
Multimodal beats any single thing. The strongest long-term outcomes come from combining approaches — movement, a talking therapy, sleep repair, and a medication if it earns its place — rather than searching for one intervention that fixes everything. There isn't one.
Exercise: The Strongest Evidence
Exercise is the best-supported treatment for fibromyalgia. It is also the one most likely to be recommended badly, and a bad recommendation does real damage — a patient who is told to "just push through" and is flattened for a week learns, entirely rationally, that exercise is dangerous. Then they stop. So the how matters as much as the what.
The Cardinal Rule: Start Absurdly Low
Start below what you think you can do, and increase more slowly than you think you should. If you can manage five minutes of walking without a flare, then five minutes is your starting dose — and you do five minutes daily for a couple of weeks before you add a single minute. This feels pathetically slow. It is also the approach that works, because the alternative — an enthusiastic first week followed by a three-day crash — puts you back to zero and costs you your confidence.
Post-exertional flares are the thing to avoid. Overdoing it does not build tolerance in fibromyalgia the way it does in a healthy athlete; it provokes a symptom flare that can last for days. Aim to finish every session feeling like you could have done a bit more. That leftover capacity is not wasted — it is what makes tomorrow's session possible.
If you have prominent post-exertional malaise — the ME/CFS pattern of a delayed, disproportionate crash — then progressive exercise is not the right frame at all, and strict pacing within your energy envelope should come first. This distinction is genuinely important and is covered in the ME/CFS overlap article.
What to Actually Do
- Walking — the most accessible option and perfectly legitimate. Five to ten minutes, most days, built up over months toward 30.
- Warm-water exercise — outstanding for people who cannot tolerate weight-bearing movement. Buoyancy removes the load, warmth eases stiffness, and the water provides gentle resistance. The Cochrane evidence for aquatic training is positive across pain, function and wellbeing. If land-based exercise flares you, start here.
- Stationary cycling — low-impact, easy to dose precisely, easy to stop.
- Tai chi — a randomized trial in the BMJ found tai chi equal or superior to aerobic exercise for fibromyalgia symptoms, with better adherence. For a condition where the main barrier is people quitting, an intervention people actually stick with is worth a great deal.
- Yoga — gentle, restorative or yin styles. Avoid hot yoga and aggressive vinyasa, which reliably provoke flares.
- Resistance training — light weights, started gently, improve strength and function over months. Do not skip this out of fear; just start with the lightest thing in the room.
Why it works. Exercise is not just distraction or general fitness. It lowers substance P, improves sleep architecture, normalises stress-axis function and recruits the body's own descending inhibition. It is treating the mechanism.
Expect the first two to three weeks to feel worse before they feel better. That is normal, it is not damage, and it passes. What you are looking for is the trend over months, not how you feel on Tuesday.
Talking Therapies, Sleep and Pacing
Cognitive Behavioural Therapy (CBT)
Let us clear the obvious objection first: being offered CBT does not mean your doctor thinks the pain is imaginary. The offer is frequently taken that way — understandably, given how often patients have been dismissed — and some people refuse a genuinely useful treatment because of it.
CBT for chronic pain is not CBT for depression, and it is not about persuading you that the pain is not there. It targets specific, well-defined mechanisms: pain catastrophizing (the spiral where a flare becomes proof that everything is about to collapse), fear-avoidance (not moving because moving hurt once, which leads to deconditioning, which leads to more pain), and the practical business of building a life around a fluctuating condition. The meta-analyses find small-to-moderate but real and durable improvements in pain, function and mood. It works on your nervous system's interpretation layer — which, as established above, is the actual site of the disease.
Acceptance and commitment therapy (ACT) and mindfulness-based stress reduction (MBSR) perform comparably and suit people who bounce off classic CBT.
Pain Neuroscience Education
Simply explaining central sensitization to patients — properly, in plain language, as a real mechanism — measurably reduces fear-avoidance and improves function. Understanding that the pain is an amplifier problem rather than evidence of ongoing damage changes what you are willing to do with your body. In a real sense, reading this page is a low dose of the intervention.
Sleep
Repairing sleep is a pain treatment, not a luxury. The basics are unglamorous and they work:
- Same bed time, same wake time — including weekends. The single most effective sleep intervention and the one most people skip.
- Cool, dark, quiet room. Around 18–20°C / 65–68°F.
- No screens for an hour before bed.
- Caffeine cut-off by midday; alcohol at least four hours before bed. Alcohol is a particular trap: it gets you to sleep and then shreds the second half of the night, which is exactly the deep sleep you cannot afford to lose.
- Get sleep apnoea ruled out if you snore or wake unrefreshed after adequate hours. This is the most commonly missed, most treatable driver in the whole condition.
- A warm bath before bed — helps stiffness and sleep onset, costs nothing, interacts with nothing.
- If behavioural measures are not enough, low-dose amitriptyline, cyclobenzaprine or trazodone are the usual pharmacological options, discussed below. CBT for insomnia (CBT-I) is a strong non-drug option and is worth asking for by name.
Long-term benzodiazepines and "z-drugs" are a poor bargain here: tolerance builds, sleep architecture degrades over time, and dependence is real. They make sleep feel shorter to wait through, without restoring the deep sleep you actually need.
Pacing
Pacing is the skill of spending your energy deliberately rather than reactively. The pattern it fixes is the boom-bust cycle, and every fibromyalgia patient knows it intimately: a good day arrives, you seize it and do everything you have been putting off, and you then pay for it for three days. The crash lifts, another good day comes, and you do it again.
The counterintuitive rule is: on good days, do less than you feel capable of. Stop while you still have something left. You are not wasting a good day — you are converting an unpredictable sawtooth into a sustainable baseline that slowly rises. Activity logs, heart-rate ceilings and timers all help. An occupational therapist who specialises in chronic pain can build this with you properly, and it is worth asking for a referral.
Medications
Medication is a supporting player, not the lead. Used with realistic expectations it is genuinely worth having; used as the whole plan it disappoints.
The Three Licensed Drugs (US)
- Duloxetine (Cymbalta) — an SNRI, typically 30–60 mg daily. Restores the failed descending inhibition. Helps pain, and often fatigue and mood too. Roughly one in four to one in five people gets a meaningful response beyond placebo. Side effects: nausea (usually settles), dry mouth, insomnia, sexual dysfunction. Must be tapered — stopping abruptly causes a genuinely unpleasant discontinuation syndrome.
- Milnacipran (Savella) — an SNRI weighted more toward norepinephrine, 100–200 mg daily in split doses. Some people who fail duloxetine do well on it. Side effects: nausea, headache, raised heart rate. Licensed for fibromyalgia in the US but not in Europe.
- Pregabalin (Lyrica) — an alpha-2-delta calcium channel ligand that reduces excitatory neurotransmitter release; 150–450 mg daily. Helps pain and sleep. Roughly one in five gets a meaningful response. Side effects: dizziness, sedation, weight gain, ankle swelling, and cognitive dulling — which is a real consideration if fibro fog is already one of your worst symptoms.
Head-to-head network meta-analysis finds these three broadly comparable in efficacy, differing mainly in side-effect profile. So the choice is often best made on which side effects you can most afford to tolerate: if sleep is your worst problem, pregabalin's sedation is a feature; if fog is your worst problem, it is a bug.
Commonly Used Off-Label
- Amitriptyline — a tricyclic at low dose (10–50 mg at night, far below antidepressant dosing). Works mainly by improving sleep. One of the oldest options; the honest position is that a minority of people benefit clearly and the quality of the supporting evidence is low by modern standards. Watch for morning grogginess, dry mouth and cognitive dulling.
- Cyclobenzaprine — structurally a tricyclic relative, 5–10 mg at night. Helps sleep and morning stiffness.
- Gabapentin — pregabalin's cheaper cousin, similar mechanism, weaker evidence in fibromyalgia specifically.
- Low-dose naltrexone (LDN) — 1.5–4.5 mg at night, a tiny fraction of the dose used to block opioids. It appears to quiet microglial activation via TLR4 and to nudge endorphin production upward. The trial evidence is genuinely promising and genuinely small — a handful of studies, mostly modest in size, showing around 30% pain reduction with a very good safety profile. It is not a miracle and it is not snake oil; it is a plausible, cheap, low-risk option with an evidence base that has not yet caught up with its popularity. See the LDN deep-dive.
- Tramadol — a weak opioid that also inhibits serotonin and norepinephrine reuptake; the SNRI action is probably what helps. Sometimes used short-term when first-line options fail, but it is still an opioid and the caution below still applies.
Opioids: Not Recommended
This deserves to be stated without hedging. Standard opioids should not be used for fibromyalgia.
The reasons are mechanistic, not moralistic:
- They do not work for this kind of pain. Opioids act on nociceptive pain — pain from tissue damage. Fibromyalgia is nociplastic pain. Trials do not show meaningful benefit.
- They can make it worse. Long-term opioid use causes opioid-induced hyperalgesia: the drug itself sensitizes the pain system, which is precisely the mechanism already misfiring in fibromyalgia. You end up feeding the fire you are trying to put out. There is also evidence that endogenous opioid receptor availability is already altered in fibromyalgia, which may be part of why exogenous opioids disappoint.
- The long-term outcomes are worse. Fibromyalgia patients on chronic opioids do worse on pain, function and disability than those managed without — alongside the familiar risks of tolerance, dependence and withdrawal.
If you are currently on opioids for fibromyalgia, this is not an accusation and it is not a reason to stop abruptly — abrupt withdrawal is dangerous and you should never do it unsupervised. It is a reason to have a conversation about a slow, supported taper alongside starting the treatments that do work. Many people find their pain is no worse, and their fog is considerably better, on the other side.
NSAIDs and Steroids
NSAIDs (ibuprofen, naproxen) do not work for fibromyalgia pain as monotherapy, and this follows directly from the mechanism: there is no inflammation for them to act on. They are worth taking for a genuinely inflammatory co-existing problem — an arthritic joint, a period — but they will not touch the fibromyalgia itself, and they carry real gastrointestinal, kidney and cardiovascular risks if taken continuously for years in the hope that they might.
Corticosteroids have no role in fibromyalgia, for the same reason, and carry substantial long-term harms.
Diet and Supplements: An Honest Look
This is the area where fibromyalgia patients are most heavily marketed to, and where the gap between what is claimed and what is known is widest. Here is a straight account.
Worth Doing
- Correct a real vitamin D deficiency. Not "optimise" it — correct it. Deficiency is common, it is associated with worse pain, and a randomized placebo-controlled trial found that supplementing genuinely deficient fibromyalgia patients improved pain. Get the blood test; treat the number if it is low. If your level is already normal, more vitamin D will not help you.
- Correct a real B12 or iron deficiency. Same logic. Test, then treat what is actually low.
- Eat in a way that supports the rest of the plan. A Mediterranean-style pattern — vegetables, fruit, fish, olive oil, nuts, minimal ultra-processed food — is associated with better pain and mood scores. The mechanism is probably unglamorous and general (better sleep, better weight, better mood, better energy for exercise) rather than anything fibromyalgia-specific. It is still worth doing.
- Address obesity if it is present. Body mass index is independently associated with fibromyalgia severity, pain threshold and physical function. This is stated as a fact, not a reproach — and losing weight while exhausted and in pain is genuinely hard, which is why it belongs downstream of sleep and movement rather than at the top of the list.
- A low-FODMAP trial if you have IBS. It reliably helps the gut symptoms, and reducing that input often lowers total pain burden. Do it as a structured, temporary elimination with reintroduction — not as a permanent restriction.
Plausible, Low-Risk, Weak Evidence
- Magnesium — a natural NMDA-receptor antagonist, and NMDA receptors drive the wind-up described above, so the rationale is sound. The clinical trial evidence in fibromyalgia is small and preliminary. It is cheap, safe, and helps sleep and muscle cramps in many people. Reasonable to try at 200–400 mg of a well-absorbed form such as magnesium glycinate at night. Do not expect it to be the answer.
- Coenzyme Q10 — small trials suggest benefit for pain and fatigue. Preliminary. Low risk, moderate cost.
- Melatonin — low dose (0.5–3 mg) for circadian support if sleep timing is the problem.
- Acupuncture — trial results are genuinely mixed. Low risk. If you try it and it helps you, that is a legitimate reason to continue; if six sessions do nothing, stop.
The honest framing for everything in this group: a reasonable experiment, not a treatment plan. Try one thing at a time, give it a defined window, and be willing to conclude it did nothing.
What Is Not Supported
Being told the truth about what does not work is as valuable as being told what does — it is your money, your hope and your time, and all three are finite.
- Most supplement protocols. The elaborate multi-supplement "fibromyalgia protocols" sold online — stacks of a dozen products taken together — have no evidence base as protocols. The individual ingredients are mostly untested in fibromyalgia, the combinations entirely so, and the cost is substantial. Correcting a documented deficiency is medicine. Taking fifteen capsules a day on the theory that one of them might be doing something is not.
- "Adrenal fatigue." This is not a recognised medical diagnosis and there is no evidence it exists. Systematic reviews have looked and found nothing. It is true that the HPA (stress) axis behaves abnormally in fibromyalgia — but "your adrenal glands are exhausted and need supplements to recover" is a marketing story, not a physiological one. The tests sold to diagnose it (typically salivary cortisol panels) do not diagnose anything. Be especially wary when the diagnosis arrives bundled with the supplements that treat it.
- Elimination diets as a cure. Cutting out gluten, nightshades, dairy or lectins does not cure fibromyalgia, and no trial shows that it does. Some individuals do feel better on a restricted diet — often those with genuine coeliac disease or IBS, both of which are worth testing for properly. But a permanent, ever-narrowing diet is a real cost: it is socially isolating, nutritionally risky, and it can turn eating into another source of anxiety. If you want to trial an elimination, do it as a structured 4–6 week experiment with systematic reintroduction, and hold yourself to honest results.
- Chronic Lyme / systemic candida / "toxic mould" as a universal explanation. Where these are real, diagnosed conditions, they should be treated. As blanket explanations for fibromyalgia — usually accompanied by expensive non-validated testing and long courses of treatment — they are not supported, and long-term antibiotics in particular carry genuine harm.
- Detoxes, cleanses, and heavy-metal chelation. No evidence in fibromyalgia. Chelation carries real risks and has caused deaths.
- Opioids. Covered above, and worth repeating here because it belongs on this list.
- NSAIDs and steroids as primary therapy. Wrong mechanism, real harms.
- Anything promising a cure. There is currently no cure for fibromyalgia. There is meaningful, sometimes dramatic improvement — many people get substantially better and build full lives — but anyone selling a cure is selling something. The strongest predictor of improvement is patient, consistent, multimodal management, which is unfortunately much harder to package and sell than a bottle.
None of this means "nothing works". It means the things that work are the unglamorous ones near the top of this page, and the fact that they are unglamorous is not evidence against them.
Living with Fibromyalgia
Fibromyalgia is a manageable condition, not a progressive one. It does not damage your body, it does not shorten your life, and it is not a slow slide downhill. Most people improve considerably with the right combination of treatment and self-management — though "improve" usually means good stretches, flares that get shorter, and a life built to fit, rather than a single day when it all stops.
You Will Have to Advocate for Yourself
Many patients spend years being disbelieved before they are diagnosed, and some are disbelieved afterwards too. A few things help:
- Bring data. The Fibromyalgia Impact Questionnaire (FIQ-R) is a validated, scored questionnaire you can complete yourself and take to appointments. It converts "I feel awful" into a number that can be tracked over time — and a number is much harder to wave away. It is also useful evidence for work accommodations, insurance appeals and disability applications.
- Track symptoms briefly, not obsessively. Enough to spot patterns and show a clinician a trend. Not so much that your condition becomes your full-time occupation.
- Find a clinician who believes you. This is a legitimate criterion, not a luxury. A doctor who takes fibromyalgia seriously will get better results from the same treatments than one who thinks you are exaggerating, and you are allowed to keep looking.
At Work
Common accommodations that make employment sustainable: flexible or variable hours to absorb bad days, permission to move or change position, a proper ergonomic assessment, reduced multitasking demands, quieter workspaces, and the option to work from home during flares. In the United States, fibromyalgia is covered by the Americans with Disabilities Act where it substantially limits major life activities; similar protections exist under the Equality Act in the UK and equivalent legislation elsewhere.
Explaining It to People Who Cannot See It
Fibromyalgia is invisible, it fluctuates unpredictably, and you may look completely well on a day you can barely function. People find that hard to hold in their heads — so they reach for explanations that fit their model instead, which is where "but you were fine last week" comes from.
The spoon theory (Christine Miserandino's metaphor) is the most useful shortcut ever devised for this: you start each day with a limited number of spoons, every activity costs one, and when they are gone they are gone — and borrowing against tomorrow means tomorrow starts short. It gives people a model where none of your behaviour looks like inconsistency or laziness. It is worth ten minutes of explanation to the people you live with.
Support and Resources
- National Fibromyalgia Association — fmaware.org
- American Chronic Pain Association — theacpa.org
- Fibromyalgia Action UK — fmauk.org
A last word, because it is the thing most worth saying: the pain is real, you are not imagining it, and you are not weak for finding it hard. You have a condition with a measurable neurological basis, a name, a diagnostic standard and a set of treatments that genuinely help. Being believed should never have been the difficult part.
Important Cautions
- Never stop opioids abruptly. If you are on them, taper slowly and with medical supervision. Abrupt withdrawal is dangerous.
- Low-dose naltrexone must not be combined with opioids. It blocks opioid receptors and will precipitate acute withdrawal. You must be off opioids before starting LDN.
- Do not combine 5-HTP, St John's wort or tryptophan with an SSRI or SNRI (including duloxetine and milnacipran) without medical supervision — risk of serotonin syndrome, which can be life-threatening. This is a real interaction, and these supplements are sold freely to exactly the population most likely to be on an SNRI.
- Taper duloxetine, do not stop it suddenly. Discontinuation syndrome is unpleasant and avoidable.
- Do not "push through" a flare. Post-exertional flares can cost you days. Backing off is not giving up; it is how you get to exercise again next week.
- Get the mimics screened before settling on the diagnosis — thyroid, vitamin D, B12, inflammatory markers, and a sleep study if you snore or wake unrefreshed. Not because fibromyalgia is a diagnosis of exclusion (it is not), but because these are treatable and it would be a waste to miss one.
- Tell your doctor about every supplement you take. "Natural" does not mean "no interactions", and several common supplements interact with fibromyalgia medications.
- Be sceptical of anything sold as a cure, particularly if the person diagnosing you also sells the treatment.
- Improvement is gradual. Meaningful change is measured over months. A treatment that has done nothing in a week has not necessarily failed; a treatment that has done nothing in three months probably has.
Key Research Papers
Every citation below has been checked against the PubMed record it links to. Each link opens the paper's PubMed entry.
What Fibromyalgia Is
- Clauw DJ. Fibromyalgia: a clinical review. JAMA. 2014;311(15):1547-1555.
- Häuser W, et al. Fibromyalgia. Nature Reviews Disease Primers. 2015;1:15022.
- Fitzcharles MA, et al. Nociplastic pain: towards an understanding of prevalent pain conditions. The Lancet. 2021;397(10289):2098-2110.
- Goldenberg DL, et al. Management of fibromyalgia syndrome. JAMA. 2004;292(19):2388-2395.
Diagnostic Criteria
- Wolfe F, et al. The American College of Rheumatology 1990 criteria for the classification of fibromyalgia. Arthritis & Rheumatism. 1990;33(2):160-172.
- Wolfe F, et al. The American College of Rheumatology preliminary diagnostic criteria for fibromyalgia and measurement of symptom severity. Arthritis Care & Research. 2010;62(5):600-610.
- Wolfe F, et al. 2016 revisions to the 2010/2011 fibromyalgia diagnostic criteria. Seminars in Arthritis and Rheumatism. 2016;46(3):319-329.
Mechanism: Central Sensitization
- Russell IJ, et al. Elevated cerebrospinal fluid levels of substance P in patients with the fibromyalgia syndrome. Arthritis & Rheumatism. 1994;37(11):1593-1601.
- Harris RE, et al. Elevated insular glutamate in fibromyalgia is associated with experimental pain. Arthritis & Rheumatism. 2009;60(10):3146-3152.
- Napadow V, et al. Intrinsic brain connectivity in fibromyalgia is associated with chronic pain intensity. Arthritis & Rheumatism. 2010;62(8):2545-2555.
- Oaklander AL, et al. Objective evidence that small-fiber polyneuropathy underlies some illnesses currently labeled as fibromyalgia. Pain. 2013;154(11):2310-2316.
- Üçeyler N, et al. Small fibre pathology in patients with fibromyalgia syndrome. Brain. 2013;136(6):1857-1867.
- Moldofsky H, et al. Musculoskeletal symptoms and non-REM sleep disturbance in patients with "fibrositis syndrome" and healthy subjects. Psychosomatic Medicine. 1975;37(4):341-351.
Non-Drug Treatment
- Macfarlane GJ, et al. EULAR revised recommendations for the management of fibromyalgia. Annals of the Rheumatic Diseases. 2017;76(2):318-328.
- Bidonde J, et al. Aerobic exercise training for adults with fibromyalgia. Cochrane Database of Systematic Reviews. 2017;(6):CD012700.
- Häuser W, et al. Efficacy of different types of aerobic exercise in fibromyalgia syndrome: a systematic review and meta-analysis of randomised controlled trials. Arthritis Research & Therapy. 2010;12(3):R79.
- Bidonde J, et al. Aquatic exercise training for fibromyalgia. Cochrane Database of Systematic Reviews. 2014;(10):CD011336.
- Busch AJ, et al. Resistance exercise training for fibromyalgia. Cochrane Database of Systematic Reviews. 2013;(12):CD010884.
- Wang C, et al. Effect of tai chi versus aerobic exercise for fibromyalgia: comparative effectiveness randomized controlled trial. BMJ. 2018;360:k851.
- Bernardy K, et al. Efficacy, acceptability and safety of cognitive behavioural therapies in fibromyalgia syndrome — a systematic review and meta-analysis of randomized controlled trials. European Journal of Pain. 2018;22(2):242-260.
- Kundakci B, et al. Efficacy of nonpharmacological interventions for individual features of fibromyalgia: a systematic review and meta-analysis of randomised controlled trials. Pain. 2022;163(8):1432-1445.
- Bidonde J, et al. Effectiveness of non-pharmacological interventions for fibromyalgia and quality of review methods: an overview of Cochrane Reviews. Seminars in Arthritis and Rheumatism. 2023;63:152248.
Medications
- Arnold LM, et al. A double-blind, multicenter trial comparing duloxetine with placebo in the treatment of fibromyalgia patients with or without major depressive disorder. Arthritis & Rheumatism. 2004;50(9):2974-2984.
- Crofford LJ, et al. Pregabalin for the treatment of fibromyalgia syndrome: results of a randomized, double-blind, placebo-controlled trial. Arthritis & Rheumatism. 2005;52(4):1264-1273.
- Lee YH, Song GG. Comparative efficacy and tolerability of duloxetine, pregabalin, and milnacipran for the treatment of fibromyalgia: a Bayesian network meta-analysis of randomized controlled trials. Rheumatology International. 2016;36(5):663-672.
- Moore RA, et al. Amitriptyline for fibromyalgia in adults. Cochrane Database of Systematic Reviews. 2019;CD011824.
- Younger J, et al. Low-dose naltrexone for the treatment of fibromyalgia: findings of a small, randomized, double-blind, placebo-controlled, counterbalanced, crossover trial assessing daily pain levels. Arthritis & Rheumatism. 2013;65(2):529-538.
- Painter JT, Crofford LJ. Chronic opioid use in fibromyalgia syndrome: a clinical review. Journal of Clinical Rheumatology. 2013;19(2):72-77.
Diet, Nutrients and Lifestyle
- Wepner F, et al. Effects of vitamin D on patients with fibromyalgia syndrome: a randomized placebo-controlled trial. Pain. 2014;155(2):261-268.
- Okifuji A, et al. Relationship between fibromyalgia and obesity in pain, function, mood, and sleep. The Journal of Pain. 2010;11(12):1329-1337.
Live PubMed Searches
- Fibromyalgia central sensitization
- Fibromyalgia ACR 2016 criteria
- Pregabalin, duloxetine, milnacipran
- Low-dose naltrexone in fibromyalgia
- Fibromyalgia exercise and tai chi
- Fibromyalgia cognitive behavioural therapy
- Fibromyalgia and opioid-induced hyperalgesia
- Fibromyalgia small-fiber neuropathy
- Fibromyalgia sleep architecture
- Fibromyalgia neuroinflammation and microglia
- Fibromyalgia and vitamin D (randomized trials)
- Fibromyalgia and ME/CFS overlap
Connections
- Deep Dives: Central Sensitization Explained · ACR 2016 Diagnostic Criteria · Sleep & Non-Restorative Sleep · Low-Dose Naltrexone · Exercise Pacing & Graded Movement · Nutrient Gaps: Mg, D, B12 · Small-Fiber Neuropathy Overlap · Fibromyalgia & ME/CFS Overlap · Cannabis, CBD & Medical Marijuana · History of Fibromyalgia
- Chronic Pain
- Central Sensitization & Nociplastic Pain
- Non-Opioid Medications for Chronic Pain
- Sleep, Exercise & Lifestyle for Chronic Pain
- Neuropathic Pain
- Complex Regional Pain Syndrome
- Migraine
- Mast Cell Activation Syndrome
- POTS
- Ehlers-Danlos Syndrome
- Rheumatoid Arthritis
- Lupus
- Osteoarthritis
- Arthritis
- Low Back Pain
- Insomnia
- Depression
- Anxiety
- Sleep Hygiene
- Stress Management
- Low-Dose Naltrexone
- Anti-Inflammatory Diet
- Magnesium
- Magnesium Glycinate
- Vitamin D3
- Omega-3 Fatty Acids
- Muscle Contraction — interactive animation
- Cryotherapy for Pain, Arthritis and Inflammation
- Magnesium Glycinate for Muscle Relaxation — dosing protocol for fibromyalgia tender points, cramps and the sleep disruption that comes with them.
- Low-Dose Naltrexone for Pain and Fibromyalgia — the Younger and Mackey trials and the microglial model behind LDN's effect on central pain.