Vitamin D3 (Cholecalciferol): The Sunshine Hormone, Immune Commander, and Master Gene Regulator
Vitamin D3, known chemically as cholecalciferol, occupies a position unlike any other vitamin in human biology. Technically, it is not a vitamin at all — it is a secosteroid prohormone that the body synthesizes in the skin upon exposure to ultraviolet B (UVB) radiation from sunlight, converts through a cascade of enzymatic reactions in the liver and kidneys into its active hormonal form calcitriol (1,25-dihydroxyvitamin D3), and then deploys to regulate the expression of over 1,000 genes — approximately 5% of the entire human genome. In natural medicine, Vitamin D3 is regarded as perhaps the single most important and most commonly deficient nutrient in the modern world. The global epidemic of Vitamin D insufficiency — estimated to affect over 1 billion people worldwide — has been linked to increased risk of nearly every major chronic disease: osteoporosis, cancer, cardiovascular disease, autoimmune conditions, diabetes, depression, infectious disease, and premature death. Humans evolved under equatorial sunlight, and our modern indoor lifestyles, sunscreen use, northern latitudes, and clothing coverage have created a profound mismatch between our biological needs and our actual Vitamin D status.
Interactive Visualization Bone Remodeling & Calcium Balance Watch osteoclasts tunnel and osteoblasts rebuild — then drop vitamin D and see PTH quietly strip calcium out of your skeleton. Launch → Interactive Visualization How Your Skin Makes Vitamin D Hit 7-dehydrocholesterol with UVB and follow it through liver and kidney to the active hormone — then try winter, sunscreen, darker skin, or low magnesium. Launch →Table of Contents
- Synthesis, Activation, and the Vitamin D Endocrine System
- Bone Health and Calcium-Phosphorus Homeostasis
- Immune System — The Master Immune Modulator
- Cancer Prevention and Anticancer Mechanisms
- Mental Health — Depression, Seasonal Affective Disorder, and Cognitive Function
- Cardiovascular Health
- Blood Sugar Regulation and Diabetes
- Muscle Function and Physical Performance
- Pregnancy and Fetal Development
- Respiratory Health
- Thyroid Health
- Gut Health
- Skin Health
- Fertility and Reproductive Health
- Sources of Vitamin D3
- Recommended Daily Intake and Optimal Levels
- Supplemental Forms
- Synergistic Nutrients — The Critical Partners
- Populations at Higher Risk of Deficiency
- Signs of Deficiency
- Toxicity and Safety
- Special Therapeutic Applications
- Historical Medical Use & the Dosing Story (1926–1972)
- Connections
- Featured Videos
1. Synthesis, Activation, and the Vitamin D Endocrine System
Understanding Vitamin D3 begins with understanding its unique synthesis and activation pathway — a process that makes it more akin to a hormone than a traditional vitamin.
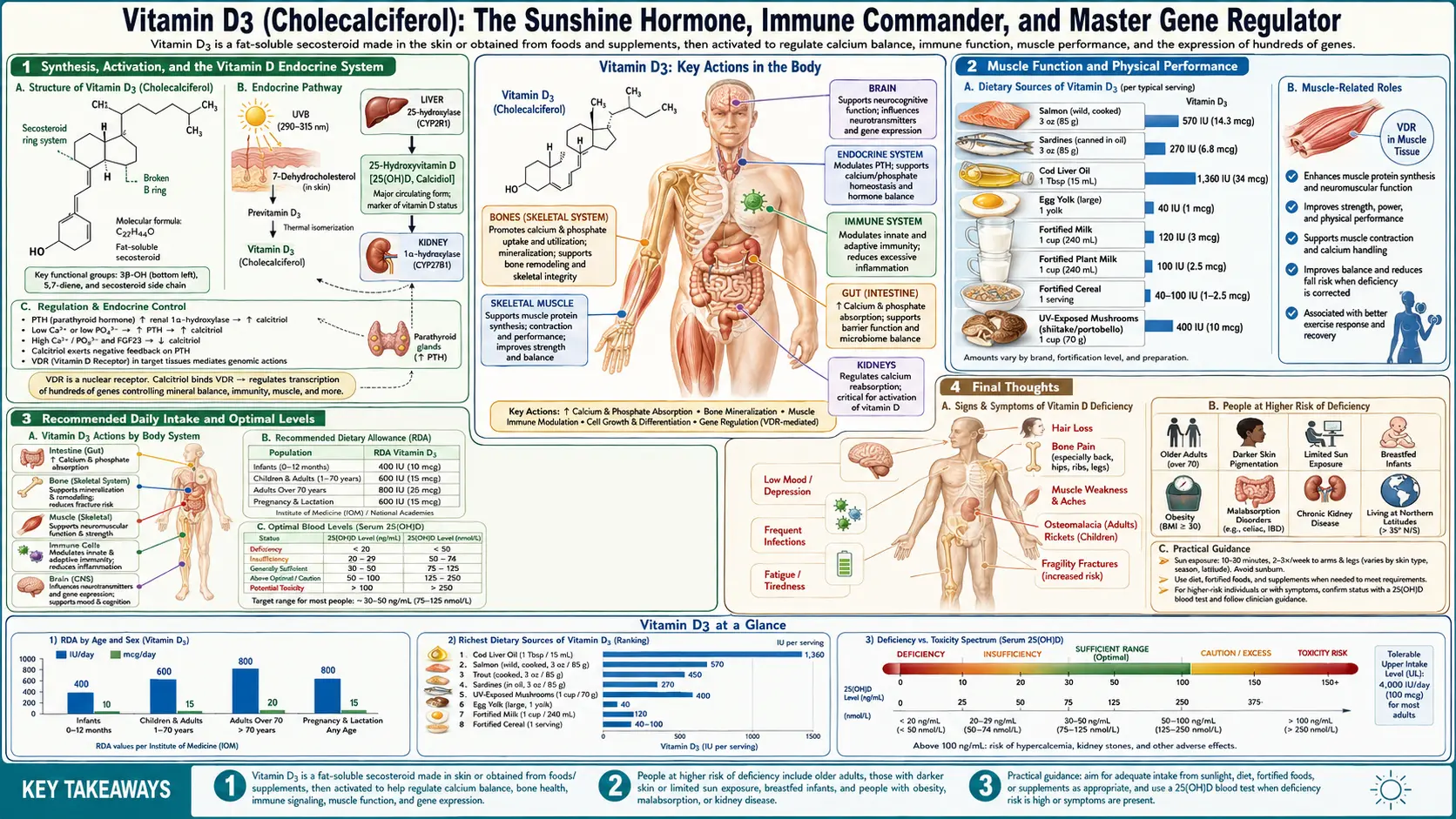
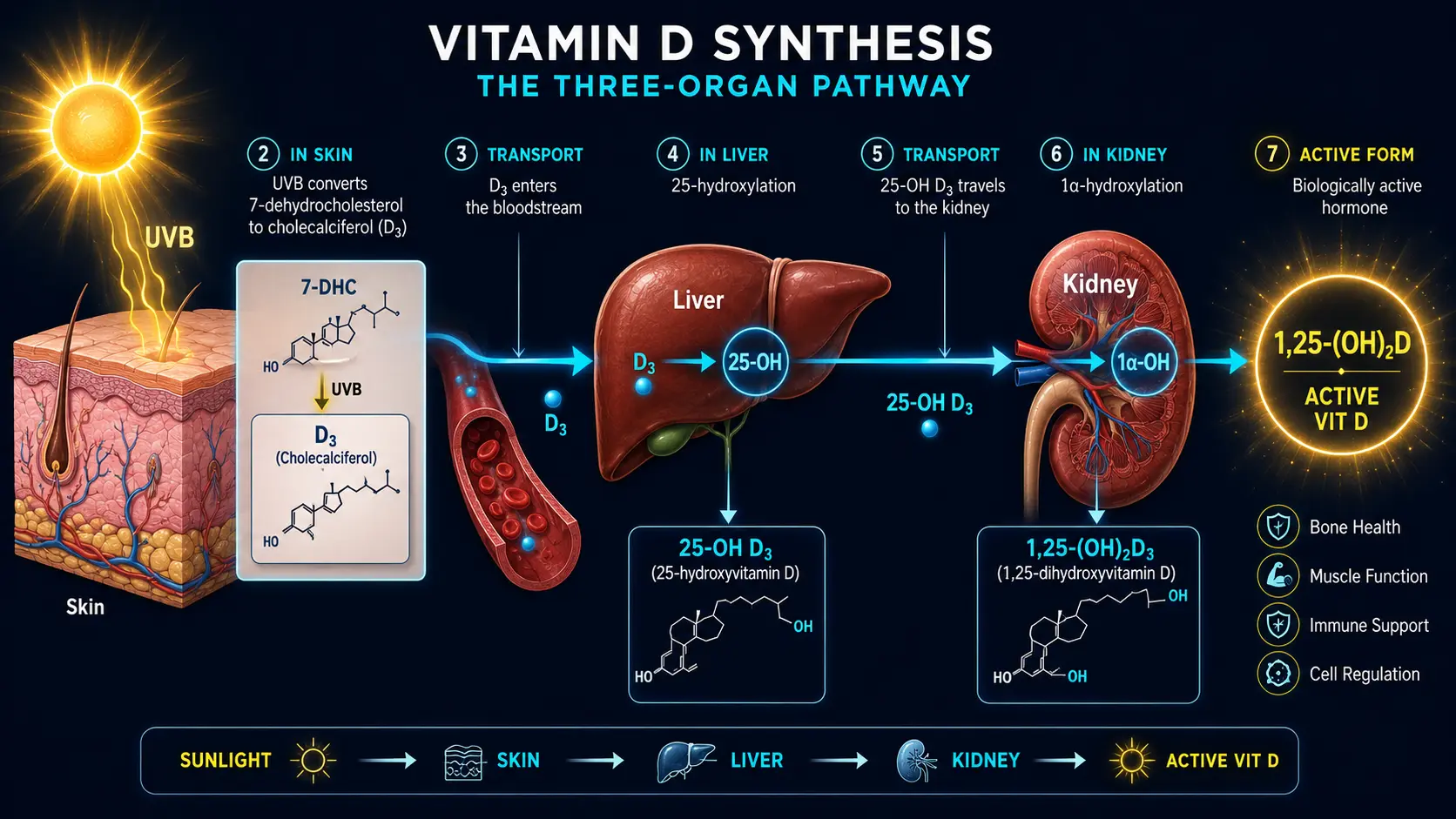
- Step 1 — Cutaneous Synthesis: When UVB radiation (wavelength 290–315 nm) strikes bare skin, it converts 7-dehydrocholesterol (a cholesterol derivative present in the epidermis) to previtamin D3, which rapidly isomerizes to cholecalciferol (Vitamin D3) through a heat-dependent reaction. This is the body's primary source of Vitamin D under natural conditions.
- Step 2 — Hepatic Hydroxylation: Cholecalciferol is transported to the liver bound to Vitamin D-binding protein (DBP), where the enzyme 25-hydroxylase (CYP2R1) converts it to 25-hydroxyvitamin D [25(OH)D] — calcidiol. This is the primary circulating form of Vitamin D and the metabolite measured in blood tests to assess Vitamin D status.
- Step 3 — Renal Activation: In the kidneys, the enzyme 1-alpha-hydroxylase (CYP27B1) converts 25(OH)D to 1,25-dihydroxyvitamin D3 [1,25(OH)₂D] — calcitriol. Calcitriol is the fully active hormonal form of Vitamin D — the form that binds to the Vitamin D Receptor (VDR) and regulates gene expression.
- Extrarenal Activation: Critically, the 1-alpha-hydroxylase enzyme is also expressed in many tissues beyond the kidneys — including immune cells, breast tissue, prostate, colon, brain, pancreas, and placenta. This means that local, tissue-level activation of Vitamin D occurs throughout the body, enabling autocrine and paracrine (local) signaling independent of renal calcitriol production. This extrarenal activation is central to Vitamin D's roles in immune defense, cancer prevention, and cellular regulation.
- The Vitamin D Receptor (VDR): Calcitriol exerts its biological effects by binding to the Vitamin D Receptor (VDR), a nuclear receptor that functions as a transcription factor. The VDR-calcitriol complex binds to Vitamin D Response Elements (VDREs) in the promoter regions of target genes, modulating their expression. VDRs are expressed in virtually every tissue and cell type in the body — confirming that Vitamin D's influence extends far beyond calcium and bone metabolism.
- Self-Regulation: The system is elegantly self-regulating. Excess sun exposure cannot produce toxic levels of Vitamin D3 because previtamin D3 and Vitamin D3 are photodegraded by continued UV exposure into inert metabolites. The kidneys tightly regulate calcitriol production based on calcium, phosphorus, and parathyroid hormone (PTH) levels. However, supplemental Vitamin D3 lacks this photodegradation safeguard, which is why toxicity — though rare — is possible with very high-dose supplementation.
2. Bone Health and Calcium-Phosphorus Homeostasis
The classical and best-established role of Vitamin D is the regulation of calcium and phosphorus metabolism — the mineral foundation of the skeletal system.
- Intestinal Calcium Absorption: Calcitriol induces the expression of calbindin, TRPV6, and other calcium transport proteins in the intestinal epithelium, increasing the active absorption of dietary calcium from the gut. Without adequate Vitamin D, only 10–15% of dietary calcium is absorbed; with sufficient Vitamin D, absorption increases to 30–40% or more.
- Phosphorus Absorption: Vitamin D similarly enhances the intestinal absorption of phosphorus — the other critical mineral component of hydroxyapatite, the crystalline mineral that gives bone its hardness and compressive strength.
- Bone Mineralization: By ensuring adequate blood levels of calcium and phosphorus, Vitamin D enables the proper mineralization of the collagen matrix laid down by osteoblasts. Without Vitamin D, even abundant calcium intake cannot be deposited into bone effectively.
- Rickets: In children, severe Vitamin D deficiency causes rickets — a devastating failure of bone mineralization that results in soft, deformed bones, bowed legs, widened wrists, prominent frontal bossing, delayed closure of fontanelles, poor growth, dental defects, and increased fracture risk. Rickets was historically epidemic in industrial cities and is now resurging in some populations.
- Osteomalacia: The adult equivalent of rickets, osteomalacia involves the softening and weakening of mature bone due to inadequate mineralization. It presents as bone pain (often mistaken for fibromyalgia), muscle weakness, difficulty walking, and increased fracture risk.
- Osteoporosis: While osteoporosis is primarily a disease of bone mass loss (reduced osteoblast activity relative to osteoclast activity), Vitamin D deficiency profoundly exacerbates osteoporotic fracture risk by impairing calcium absorption, causing secondary hyperparathyroidism (PTH rises to mobilize calcium from bone), and reducing bone mineralization quality.
- Parathyroid Hormone (PTH) Regulation: Vitamin D suppresses PTH secretion from the parathyroid glands. When Vitamin D is deficient, PTH rises (secondary hyperparathyroidism), mobilizing calcium from bone to maintain blood calcium levels — at the direct expense of bone density.
- Fracture Prevention: Meta-analyses demonstrate that Vitamin D supplementation (particularly at doses achieving 25(OH)D levels above 30 ng/mL), especially when combined with calcium, significantly reduces the risk of hip fractures and non-vertebral fractures in older adults.
- Fall Prevention: Vitamin D supports neuromuscular function and reduces the risk of falls in the elderly — an effect that contributes to fracture prevention beyond its skeletal benefits. This muscle-strengthening effect is mediated through VDR-dependent regulation of muscle protein synthesis and calcium handling in muscle fibers.
3. Immune System — The Master Immune Modulator
Vitamin D's role in immune regulation is arguably as important as its role in bone health — and it is the function most emphasized in natural medicine.
- Innate Immune Activation: When immune cells (macrophages, monocytes, dendritic cells) encounter a pathogen, they upregulate both the VDR and the 1-alpha-hydroxylase enzyme, locally converting circulating 25(OH)D to active calcitriol. This locally produced calcitriol induces the expression of cathelicidin (LL-37) and defensins — antimicrobial peptides that directly kill bacteria, viruses, and fungi. This is one of the most elegant examples of the immune system using a nutrient as a weapon.
- Cathelicidin (LL-37): Calcitriol is the most potent known inducer of cathelicidin expression. LL-37 disrupts microbial cell membranes, neutralizes bacterial endotoxins (LPS), exhibits antiviral activity, and modulates the inflammatory response. Vitamin D deficiency directly impairs the body's ability to produce this critical antimicrobial peptide.
- Tuberculosis — The Historical Connection: Before the discovery of antibiotics, tuberculosis was treated with sunlight exposure (heliotherapy) and cod liver oil — both of which we now understand to be Vitamin D interventions. The antimycobacterial effect of cathelicidin, induced by Vitamin D, explains why these treatments were effective and why Vitamin D deficiency increases susceptibility to tuberculosis.
- Respiratory Infections: A landmark individual patient data meta-analysis (Martineau et al., BMJ, 2017) of 25 randomized controlled trials involving over 11,000 participants demonstrated that Vitamin D supplementation reduced the risk of acute respiratory tract infections by approximately 12% overall, with the greatest protection (70% reduction) seen in individuals with the lowest baseline Vitamin D levels receiving daily or weekly supplementation.
- Influenza and Seasonal Respiratory Illness: Observational studies have consistently associated low Vitamin D status with increased susceptibility to influenza and other seasonal respiratory infections. The mechanistic rationale and observational data strongly support optimizing Vitamin D status as a component of respiratory immune defense, particularly during the winter months when endogenous synthesis is minimal at higher latitudes.
- Adaptive Immune Regulation: Calcitriol modulates the adaptive immune system by suppressing excessive Th1 and Th17 pro-inflammatory responses while promoting regulatory T-cell (Treg) development and anti-inflammatory Th2 responses. This immunomodulatory balance is critical for preventing autoimmune attack against the body's own tissues.
- Autoimmune Disease: Vitamin D deficiency is strongly associated with increased risk and severity of multiple autoimmune diseases, including multiple sclerosis, type 1 diabetes, rheumatoid arthritis, systemic lupus erythematosus, inflammatory bowel disease, psoriasis, Hashimoto's thyroiditis, and Graves' disease. The VITAL study extension demonstrated that Vitamin D supplementation (2,000 IU/day) reduced the incidence of autoimmune diseases by 22% over 5 years — a landmark finding.
- The Latitude Gradient: The incidence of autoimmune diseases, many cancers, and cardiovascular disease increases with distance from the equator — mirroring the decline in UVB exposure and Vitamin D synthesis. This geographical pattern provides some of the most compelling epidemiological evidence for Vitamin D's protective role in these conditions.
4. Cancer Prevention and Anticancer Mechanisms
The relationship between Vitamin D and cancer is one of the most extensively studied areas in nutritional epidemiology and molecular oncology.
- Gene Regulation: Calcitriol regulates the expression of genes involved in cell proliferation, differentiation, apoptosis (programmed cell death), and angiogenesis (blood vessel formation) — all of which are dysregulated in cancer. Through VDR-mediated gene expression, Vitamin D promotes the differentiation of cancer cells toward more normal phenotypes, inhibits uncontrolled proliferation, triggers apoptosis in malignant cells, and suppresses the formation of new blood vessels that feed tumor growth.
- Colorectal Cancer: The most robustly demonstrated cancer-Vitamin D relationship. Higher 25(OH)D levels are consistently associated with significantly reduced risk of colorectal cancer in observational studies. Individuals with levels above 40 ng/mL have approximately 50–65% lower colorectal cancer risk compared to those below 20 ng/mL.
- Breast Cancer: Numerous observational studies associate higher Vitamin D status with reduced breast cancer risk, particularly for ER-positive breast cancers. Meta-analyses suggest a 15–45% risk reduction at optimal Vitamin D levels.
- Prostate Cancer: The evidence is mixed but evolving. Some studies suggest that both very low and very high Vitamin D levels may be associated with increased prostate cancer risk, suggesting an optimal range rather than a simple linear relationship.
- Other Cancers: Epidemiological evidence supports protective associations between Vitamin D and cancers of the lung, pancreas, ovary, bladder, kidney, and non-Hodgkin lymphoma, though the strength of evidence varies.
- Cancer Mortality: A meta-analysis of randomized controlled trials demonstrated that Vitamin D3 supplementation reduced overall cancer mortality by approximately 13%. This finding suggests that while Vitamin D may have modest effects on cancer incidence, its impact on survival after cancer diagnosis may be more substantial.
- Wnt/β-Catenin Pathway: Calcitriol inhibits the Wnt/β-catenin signaling pathway — one of the most commonly aberrantly activated pathways in colorectal and other cancers. This is a key molecular mechanism by which Vitamin D suppresses intestinal carcinogenesis.
- Immune Surveillance: By enhancing NK cell activity and promoting anti-tumor immune responses, Vitamin D supports the immune system's ability to detect and eliminate emerging cancer cells before they establish tumors.
5. Mental Health — Depression, Seasonal Affective Disorder, and Cognitive Function
- VDR in the Brain: Vitamin D receptors and the 1-alpha-hydroxylase enzyme are expressed throughout the brain — in the hippocampus, hypothalamus, prefrontal cortex, cerebellum, and substantia nigra — confirming Vitamin D's direct neurological relevance.
- Depression: Low Vitamin D status is one of the most consistently observed nutritional associations with major depressive disorder. Meta-analyses of clinical trials demonstrate that Vitamin D supplementation produces statistically significant improvements in depression scores, with the greatest effects seen in individuals with clinically significant depression and low baseline Vitamin D levels.
- Seasonal Affective Disorder (SAD): The seasonal pattern of depression — with symptoms peaking in winter months when UVB exposure is minimal — closely mirrors the seasonal decline in Vitamin D synthesis. Vitamin D supplementation is used by many natural practitioners as a component of SAD management alongside light therapy.
- Neurotransmitter Regulation: Calcitriol regulates the expression of the genes encoding tryptophan hydroxylase 2 (TPH2) — the rate-limiting enzyme for serotonin synthesis in the brain — and tyrosine hydroxylase, the rate-limiting enzyme for dopamine synthesis. Vitamin D deficiency may therefore directly impair the production of both serotonin and dopamine.
- Neuroinflammation: Vitamin D suppresses microglial activation and reduces neuroinflammatory cytokines (IL-6, TNF-α, IL-1β) in the brain — processes implicated in the pathophysiology of depression, anxiety, and neurodegeneration.
- Cognitive Decline and Dementia: Low Vitamin D status is associated with accelerated cognitive decline, reduced hippocampal volume, and increased risk of Alzheimer's disease and all-cause dementia. The Vitamin D-VDR system supports neuronal calcium regulation, amyloid-beta clearance, neuroprotection, and synaptic plasticity.
- Schizophrenia: Neonatal Vitamin D deficiency is associated with increased risk of schizophrenia in adulthood, suggesting a developmental programming effect. This is consistent with Vitamin D's role in brain development during fetal and neonatal life.
- Anxiety: Emerging evidence links low Vitamin D to increased anxiety, and supplementation trials have shown modest anxiolytic effects.
6. Cardiovascular Health
- VDR in Cardiovascular Tissue: VDRs are expressed in cardiomyocytes (heart muscle cells), vascular smooth muscle cells, and endothelial cells, confirming direct cardiovascular relevance.
- Blood Pressure: Vitamin D suppresses the renin-angiotensin-aldosterone system (RAAS) by downregulating renin gene expression. Vitamin D deficiency leads to inappropriate RAAS activation — a major driver of hypertension. Observational studies consistently show inverse associations between Vitamin D levels and blood pressure, though supplementation trials have yielded mixed results on blood pressure reduction.
- Endothelial Function: Calcitriol supports endothelial nitric oxide production, reduces oxidative stress in the vascular wall, and inhibits endothelial cell inflammation — all of which promote healthy vascular function.
- Atherosclerosis: Vitamin D deficiency promotes vascular calcification (paradoxically, by disrupting calcium homeostasis), endothelial dysfunction, inflammation, and smooth muscle cell proliferation in arterial walls — all components of atherosclerotic progression.
- Heart Failure: Low Vitamin D is highly prevalent among heart failure patients and is associated with worse functional class, higher mortality, and increased risk of adverse cardiac events. Vitamin D supports cardiac contractility through its role in myocardial calcium handling.
- Cardiovascular Mortality: Multiple large observational studies demonstrate a U-shaped or inverse relationship between Vitamin D status and cardiovascular mortality, with the lowest risk at 25(OH)D levels of approximately 30–50 ng/mL.
- Arterial Stiffness: Vitamin D deficiency is associated with increased arterial stiffness and pulse wave velocity — independent risk factors for cardiovascular events. Supplementation has shown modest improvements in some studies.
7. Blood Sugar Regulation and Diabetes
- Pancreatic Beta Cell Function: VDRs are expressed on pancreatic beta cells, and calcitriol enhances insulin synthesis and secretion. Vitamin D deficiency impairs beta cell function and reduces insulin release in response to glucose.
- Insulin Sensitivity: Vitamin D modulates insulin sensitivity in target tissues (muscle, fat, liver) through VDR-mediated gene expression and by reducing systemic inflammation that drives insulin resistance.
- Type 2 Diabetes Prevention: The landmark D2d (Vitamin D and Type 2 Diabetes) randomized controlled trial demonstrated that Vitamin D supplementation (4,000 IU/day) reduced the risk of progression from prediabetes to type 2 diabetes by approximately 15% overall, and by up to 62% in individuals who achieved 25(OH)D levels above 40 ng/mL and were not obese.
- Type 1 Diabetes: Vitamin D's immunomodulatory effects — suppressing autoreactive Th1/Th17 cells and promoting regulatory T-cells — are directly relevant to the autoimmune destruction of beta cells in type 1 diabetes. Observational studies associate Vitamin D supplementation in infancy with a 30–80% reduced risk of developing type 1 diabetes.
- Gestational Diabetes: Low Vitamin D status during pregnancy is associated with increased risk of gestational diabetes. Supplementation may help reduce this risk, though optimal doses and timing are still being refined.
- Metabolic Syndrome: Vitamin D deficiency is independently associated with metabolic syndrome — the cluster of insulin resistance, central obesity, hypertension, dyslipidemia, and elevated blood sugar that drives cardiovascular disease and type 2 diabetes.
- HbA1c: Some studies demonstrate that Vitamin D supplementation in diabetic individuals with deficiency reduces HbA1c, though the magnitude of effect varies across populations and study designs.
8. Muscle Function and Physical Performance
- VDR in Skeletal Muscle: VDRs are expressed in skeletal muscle tissue, and calcitriol directly regulates muscle protein synthesis, calcium handling, and contractile function. VDR expression in muscle declines with age, paralleling the decline in Vitamin D status and muscle function.
- Muscle Strength: Vitamin D deficiency causes proximal muscle weakness — difficulty rising from a chair, climbing stairs, or lifting objects. This weakness is often subtle and attributed to aging rather than recognized as a reversible nutritional deficiency.
- Sarcopenia Prevention: Age-related loss of muscle mass and function (sarcopenia) is accelerated by Vitamin D deficiency. Supplementation in deficient elderly individuals improves muscle strength, balance, and functional performance.
- Fall Prevention: As noted in the bone health section, Vitamin D supplementation reduces fall risk in the elderly by approximately 20% — an effect largely attributable to improved neuromuscular function and balance.
- Athletic Performance: Emerging evidence suggests that Vitamin D sufficiency supports optimal muscle power, reaction time, and aerobic capacity in athletes. Many athletic performance facilities now routinely assess and optimize Vitamin D status.
- Muscle Pain and Fibromyalgia: Diffuse musculoskeletal pain and weakness are common in Vitamin D deficiency and are frequently misdiagnosed as fibromyalgia, chronic fatigue syndrome, or "growing pains" in children. Screening for Vitamin D deficiency should be routine in any patient presenting with unexplained muscle pain.
9. Pregnancy and Fetal Development
- Placental Function: The placenta expresses VDR and 1-alpha-hydroxylase, locally producing calcitriol to support immune tolerance of the fetus, implantation, placental development, and angiogenesis.
- Preeclampsia: Vitamin D deficiency in early pregnancy is associated with a 2–5 fold increased risk of preeclampsia. Calcitriol's suppression of the RAAS, its anti-inflammatory effects, and its support of endothelial function are all relevant to preeclampsia prevention.
- Gestational Diabetes: As discussed above, low Vitamin D increases gestational diabetes risk.
- Preterm Birth: Low Vitamin D status is associated with increased risk of preterm delivery, though the evidence is still evolving.
- Fetal Bone Development: Maternal Vitamin D status directly influences fetal calcium accretion and bone mineralization. Severe maternal deficiency can cause neonatal rickets and congenital craniotabes (soft skull bones).
- Immune Programming: Maternal Vitamin D status influences fetal immune system development, with deficiency associated with increased risk of asthma, allergies, and autoimmune diseases in the child.
- Brain Development: Vitamin D regulates neuronal differentiation, neurotrophic factor expression, and brain development during fetal life. Maternal deficiency is associated with altered neurocognitive outcomes in offspring.
- Recommended Supplementation: Many natural practitioners and researchers recommend 4,000–6,000 IU/day during pregnancy — significantly higher than the current official recommendation of 600 IU/day. The Hollis et al. RCT demonstrated that 4,000 IU/day was safe and effective at achieving sufficient Vitamin D levels in pregnant women and their newborns.
10. Respiratory Health
- Respiratory Infection Prevention: As detailed in the immune section, Vitamin D supplementation reduces the risk of acute respiratory tract infections, with the greatest benefit in deficient individuals.
- Asthma: Vitamin D deficiency is associated with increased asthma severity, more frequent exacerbations, reduced response to corticosteroids, and impaired lung function. Supplementation may reduce the risk of severe asthma attacks requiring emergency treatment or hospitalization.
- COPD: Low Vitamin D is common in chronic obstructive pulmonary disease and is associated with accelerated lung function decline, increased exacerbation frequency, and higher mortality.
- Lung Development: Vitamin D influences fetal and childhood lung development. Maternal deficiency is associated with reduced lung function and increased wheeze and asthma risk in offspring.
- Pneumonia: Low Vitamin D status is associated with increased pneumonia incidence and severity, consistent with its role in innate immune defense and cathelicidin production in the respiratory epithelium.
11. Thyroid Health
- Hashimoto's Thyroiditis: Vitamin D deficiency is highly prevalent among individuals with Hashimoto's — the most common cause of hypothyroidism. Low Vitamin D is associated with higher thyroid antibody levels (anti-TPO, anti-Tg), and supplementation has been shown to reduce antibody titers in some studies.
- Graves' Disease: Low Vitamin D is also associated with increased risk and severity of Graves' disease (autoimmune hyperthyroidism).
- Thyroid Cancer: Some epidemiological evidence links Vitamin D deficiency with increased thyroid cancer risk and more aggressive disease behavior.
- Immunomodulatory Mechanism: Vitamin D's promotion of regulatory T-cells and suppression of autoreactive immune responses is the primary mechanism by which it protects against autoimmune thyroid disease.
12. Gut Health
- Intestinal Barrier Function: Calcitriol enhances the expression of tight junction proteins (claudins, occludin, ZO-1) in intestinal epithelial cells, strengthening the gut barrier and reducing intestinal permeability ("leaky gut").
- Inflammatory Bowel Disease (IBD): Vitamin D deficiency is extremely common in Crohn's disease and ulcerative colitis. Supplementation reduces intestinal inflammation, supports mucosal healing, and may reduce relapse frequency. The latitude gradient of IBD incidence (higher in northern regions) is consistent with Vitamin D's protective role.
- Microbiome Modulation: Emerging research demonstrates that Vitamin D status influences the composition and diversity of the gut microbiome, promoting beneficial bacteria and suppressing pathogenic species.
- Celiac Disease: Individuals with celiac disease are at increased risk of Vitamin D deficiency due to malabsorption, and this deficiency contributes to the osteopenia and osteoporosis commonly seen in celiac patients.
- Colorectal Protection: Vitamin D's support of intestinal barrier integrity, immune regulation, and anti-inflammatory effects in the gut contributes to its well-documented protective role against colorectal cancer.
13. Skin Health
- Keratinocyte Differentiation: Calcitriol regulates the proliferation and differentiation of keratinocytes — the primary cells of the epidermis. This function is the basis for the use of Vitamin D analogues (calcipotriol/calcitriene) as topical treatments for psoriasis.
- Psoriasis: Topical Vitamin D analogues are among the first-line treatments for plaque psoriasis, reducing keratinocyte hyperproliferation, modulating local immune responses, and promoting normal skin differentiation. Systemic Vitamin D optimization further supports psoriasis management from within.
- Atopic Dermatitis (Eczema): Vitamin D deficiency is associated with increased eczema severity. Supplementation may improve skin barrier function and reduce the antimicrobial peptide deficiency that predisposes atopic skin to infection.
- Vitiligo: Vitamin D's immunomodulatory effects and its role in melanocyte function make it relevant to vitiligo management, often used alongside UV phototherapy.
- Wound Healing: Vitamin D supports wound healing through its effects on cathelicidin production (antimicrobial defense), immune regulation, and keratinocyte proliferation.
- Skin Aging: Adequate Vitamin D supports skin health and may modulate photoaging processes, though direct sun exposure for Vitamin D synthesis must be balanced against UV-induced photodamage — a nuanced consideration in natural medicine.
14. Fertility and Reproductive Health
- Female Fertility: VDRs are expressed in the ovaries, uterus, and placenta. Vitamin D deficiency is associated with reduced fertility, impaired ovarian reserve, lower IVF success rates, and conditions such as polycystic ovary syndrome (PCOS) and endometriosis.
- PCOS: Vitamin D deficiency is highly prevalent among women with PCOS and is associated with worse metabolic profiles, insulin resistance, and anovulation. Supplementation has shown improvements in insulin sensitivity, menstrual regularity, and hormonal balance in some studies.
- Male Fertility: VDRs are expressed in testicular tissue, and Vitamin D influences spermatogenesis, sperm motility, capacitation, and acrosome reaction. Deficiency is associated with reduced sperm quality and fertility.
- IVF Outcomes: Women with sufficient Vitamin D levels have significantly higher clinical pregnancy rates during IVF compared to deficient women.
- Pregnancy Outcomes: As detailed in Section 9, optimizing Vitamin D is essential for placental function, preeclampsia prevention, fetal development, and neonatal health.
15. Sources of Vitamin D3
Sunlight — The Primary Natural Source
- Optimal Conditions: Exposing large areas of bare skin (arms, legs, back) to midday sun (10 AM–3 PM) when the UV index is 3 or above for approximately 10–30 minutes (depending on skin tone, latitude, and season) can produce 10,000–25,000 IU of Vitamin D3 — far more than any food source can provide.
- Skin Tone: Melanin in darker skin absorbs UV radiation, reducing Vitamin D synthesis. Individuals with darker skin tones require 3–6 times longer sun exposure to produce equivalent amounts of Vitamin D — making them significantly more prone to deficiency, particularly at higher latitudes.
- Latitude: Above approximately 35° latitude (north of Atlanta in the US, north of Crete in Europe), UVB intensity is insufficient for cutaneous Vitamin D synthesis during winter months (November–February in the northern hemisphere), creating a "Vitamin D winter."
- Sunscreen: SPF 30 sunscreen blocks approximately 97% of UVB radiation, virtually eliminating Vitamin D synthesis. Natural practitioners often recommend brief, unprotected sun exposure followed by sun protection, rather than complete avoidance of direct sunlight.
- Age: The concentration of 7-dehydrocholesterol in the skin decreases with age. A 70-year-old produces approximately 25% of the Vitamin D3 that a 20-year-old produces from the same sun exposure.
- Glass: UVB radiation does not pass through glass. Indoor sun exposure through windows does not produce Vitamin D.
Dietary Sources
Vitamin D3 is found in very few natural foods — a reflection of the fact that sunlight, not diet, was the evolutionary source of this nutrient.
- Cod Liver Oil: The traditional powerhouse — a single tablespoon provides approximately 1,360 IU of Vitamin D3 along with Vitamin A and omega-3 fatty acids
- Wild-Caught Fatty Fish: Salmon (600–1,000 IU per 3.5 oz), mackerel, sardines, herring, and trout are the richest food sources. Wild-caught fish contain 3–4 times more Vitamin D than farmed fish.
- Egg Yolks (pasture-raised): Provide approximately 40–100 IU per yolk. Eggs from hens raised outdoors in sunlight contain significantly more Vitamin D than conventional eggs.
- Beef Liver: Provides modest amounts of Vitamin D3 (approximately 42 IU per 3 oz)
- UV-Exposed Mushrooms: Mushrooms exposed to UV light (sunlight or UV lamps) produce Vitamin D2 (ergocalciferol), not D3. While Vitamin D2 can raise 25(OH)D levels, it is less effective and shorter-lasting than D3 in humans.
- Lichen-Sourced Vitamin D3: The only vegan source of true Vitamin D3, derived from lichen — a symbiotic organism that produces cholecalciferol. Available as supplements.
- Fortified Foods: Milk, orange juice, cereals, and some plant milks are fortified with Vitamin D (usually D3 in the US, sometimes D2). Fortification doses are typically 100–150 IU per serving — insufficient for achieving optimal levels in deficient individuals.
16. Recommended Daily Intake and Optimal Levels
Official Recommendations (IU/day)
- Infants (0–12 months): 400 IU
- Children and Adults (1–70 years): 600 IU
- Adults over 70: 800 IU
- Pregnant and Breastfeeding Women: 600 IU
Natural Medicine Perspective
Most natural medicine practitioners, integrative physicians, and many endocrinologists consider the official RDA of 600 IU grossly inadequate for achieving and maintaining optimal Vitamin D status. Common therapeutic recommendations include:
- Maintenance (adults): 2,000–5,000 IU/day of Vitamin D3
- Deficiency Repletion: 5,000–10,000 IU/day for 8–12 weeks, then maintenance dosing
- Pregnancy: 4,000–6,000 IU/day (supported by the Hollis et al. RCT)
- Autoimmune Conditions: Some practitioners use 5,000–10,000 IU/day under monitoring, targeting higher 25(OH)D levels (50–80 ng/mL)
- Obese Individuals: Require 2–3 times higher doses due to sequestration of Vitamin D in adipose tissue
Optimal Blood Levels — 25(OH)D
- Deficient: Below 20 ng/mL (50 nmol/L) — associated with rickets, osteomalacia, and severe health consequences
- Insufficient: 20–29 ng/mL (50–72 nmol/L) — suboptimal for most health outcomes
- Sufficient (conventional): 30–50 ng/mL (75–125 nmol/L)
- Optimal (natural medicine): 40–70 ng/mL (100–175 nmol/L) — the range associated with the lowest disease risk across most studied conditions
- Potentially Excessive: Above 100 ng/mL (250 nmol/L) — risk of hypercalcemia increases
- Toxic: Above 150 ng/mL (375 nmol/L) — hypercalcemia and associated complications are likely
17. Supplemental Forms
- Vitamin D3 (Cholecalciferol): The preferred form in natural medicine. Identical to the form produced in the skin from sunlight. More effective than D2 at raising and maintaining 25(OH)D levels. Available from animal sources (lanolin from sheep's wool) and vegan sources (lichen).
- Vitamin D2 (Ergocalciferol): Derived from UV-irradiated yeast or fungi. Less effective than D3 at raising 25(OH)D levels, has a shorter half-life, and may be less potent at immune and extraskeletal effects. Still commonly prescribed in some medical contexts but generally not preferred in natural medicine.
- Calcidiol (25-Hydroxyvitamin D3 / Calcifediol): The pre-hydroxylated form that is the actual circulating metabolite measured in blood tests. It is more rapidly absorbed, more potent per microgram, and raises 25(OH)D levels more predictably than cholecalciferol — particularly in individuals with liver dysfunction, obesity, or malabsorption. Available as a prescription (Rayaldee®) and increasingly as a supplement.
- Oil-Based Softgels vs. Dry Tablets: Vitamin D3 is fat-soluble and is best absorbed when taken with dietary fat. Oil-based softgels and liquid drops (in MCT oil or olive oil) provide built-in fat for absorption. Dry tablets should be taken with a fat-containing meal.
- Liquid Drops: Available in concentrations of 400–4,000+ IU per drop, allowing precise dose titration. Ideal for infants, children, and individuals who prefer liquid supplementation.
- High-Dose Boluses: Weekly (50,000 IU), monthly, or quarterly high-dose protocols exist but are generally less preferred in natural medicine, as daily or weekly dosing more closely mimics physiological patterns and produces more stable 25(OH)D levels.
18. Synergistic Nutrients — The Critical Partners
Vitamin D does not work in isolation — its safety and efficacy depend critically on the presence of several synergistic nutrients.
- Vitamin K2 (Menaquinone): The single most important synergistic partner for Vitamin D. Vitamin D increases intestinal calcium absorption, while Vitamin K2 directs that calcium into bones and teeth and away from soft tissues and arteries. Without adequate K2, Vitamin D-enhanced calcium absorption can paradoxically contribute to arterial calcification, kidney stones, and soft tissue calcification. K2 activates osteocalcin (which deposits calcium into bone) and matrix Gla protein (MGP) (which prevents calcium deposition in arteries). Natural practitioners consider D3 and K2 a mandatory pairing.
- Magnesium: Magnesium is required as a cofactor for virtually every enzymatic step of Vitamin D metabolism — including its synthesis in the skin, its hydroxylation in the liver and kidneys, and its binding to transport proteins. Magnesium deficiency impairs Vitamin D activation and can cause Vitamin D supplementation to be ineffective. Conversely, Vitamin D supplementation in magnesium-depleted individuals can worsen magnesium deficiency by increasing its utilization. Many practitioners estimate that 50–80% of the population is simultaneously deficient in both Vitamin D and magnesium — making co-supplementation essential.
- Vitamin A (Retinol): Vitamins A and D share nuclear receptor partners (they both heterodimerize with RXR) and regulate overlapping sets of genes. They work synergistically in immune function, and the balance between A and D is important — excessive Vitamin D without adequate A (or vice versa) can lead to imbalances in gene expression. Cod liver oil has traditionally provided both vitamins in natural proportion.
- Calcium: Vitamin D's primary classical function is to enhance calcium absorption and maintain calcium homeostasis. Adequate calcium intake (from food, ideally) ensures that Vitamin D's bone-building effects can be realized. However, calcium supplementation without adequate D and K2 can be counterproductive.
- Zinc: Zinc is required for VDR function and for the expression of Vitamin D-dependent genes. Deficiency impairs the cellular response to Vitamin D even when circulating levels are adequate.
- Boron: This trace mineral influences Vitamin D metabolism and may enhance its effects on bone health and calcium utilization.
- Omega-3 Fatty Acids: Omega-3s and Vitamin D have synergistic anti-inflammatory, immunomodulatory, and neuroprotective effects. Fatty fish provides both naturally.
19. Populations at Higher Risk of Deficiency
- Individuals Living at High Latitudes: Above 35°N or below 35°S, UVB intensity is insufficient for adequate cutaneous Vitamin D synthesis during winter months.
- Individuals with Dark Skin: Higher melanin content reduces Vitamin D synthesis by 3–6 fold, making dark-skinned individuals at higher latitudes among the most deficient populations worldwide.
- Elderly Individuals: Reduced skin 7-dehydrocholesterol, decreased sun exposure, impaired renal hydroxylation, and lower dietary intake create a "perfect storm" of deficiency risk in the aged.
- Obese Individuals: Vitamin D is sequestered in adipose tissue, reducing its bioavailability. Obese individuals require 2–3 times higher doses to achieve equivalent 25(OH)D levels.
- Indoor Workers: Office workers, shift workers, and individuals who spend most of their time indoors receive minimal UVB exposure regardless of latitude.
- Individuals Who Cover Their Skin: For cultural, religious, or sun-protection reasons, covered skin cannot synthesize Vitamin D.
- Breastfed Infants: Human breast milk contains very little Vitamin D (typically 20–80 IU/L), making exclusively breastfed infants at high risk of deficiency unless supplemented (400 IU/day is recommended for all breastfed infants).
- Individuals with Malabsorptive Conditions: Celiac disease, Crohn's disease, cystic fibrosis, and other fat malabsorption conditions impair Vitamin D absorption from the gut.
- Post-Bariatric Surgery Patients: Gastric bypass in particular dramatically reduces Vitamin D absorption, requiring lifelong high-dose supplementation.
- Individuals with Liver or Kidney Disease: Impaired hepatic hydroxylation (liver disease) or renal hydroxylation (kidney disease) reduces the conversion of Vitamin D to its active forms.
- Individuals on Certain Medications: Anticonvulsants (phenytoin, phenobarbital), glucocorticoids, rifampin, cholestyramine, and antiretrovirals all accelerate Vitamin D catabolism or impair its metabolism.
- Vegans: Since almost all natural food sources of Vitamin D3 are animal-derived, vegans are at increased risk unless they supplement with lichen-sourced D3 or UV-exposed mushrooms (D2).
20. Signs of Deficiency
Vitamin D deficiency is often called the "silent epidemic" because it can persist for years without obvious symptoms before manifesting as serious disease. Warning signs span the musculoskeletal system (bone pain, proximal muscle weakness, fractures, rickets in children), the immune system (frequent respiratory infections, slow recovery, worsening autoimmunity), and the brain (depression, anxiety, cognitive fog, fatigue), along with slow wound healing and hair loss. For a full, patient-friendly guide to the symptoms, causes, and recovery, see Vitamin D Deficiency.
21. Toxicity and Safety
Vitamin D toxicity is rare but real. It does not come from sun exposure (the skin self-limits through photodegradation) — only from very high-dose supplementation sustained over time, which drives hypercalcemia (excess blood calcium) with nausea, excessive thirst and urination, confusion, kidney stones, and, in severe cases, kidney injury and heart-rhythm disturbances. Adequate vitamin K2 and magnesium lower the risk, while people with sarcoidosis or other granulomatous diseases are more susceptible. For a full, patient-friendly guide to the symptoms, causes, and risks, see Vitamin D Toxicity.
22. Special Therapeutic Applications
- General Optimization: 2,000–5,000 IU/day D3 with K2 (100–200 mcg MK-7) and magnesium for all adults, targeting 25(OH)D of 40–60 ng/mL.
- Deficiency Repletion: 5,000–10,000 IU/day for 8–12 weeks, followed by maintenance dosing with monitoring.
- Autoimmune Disease Support: 5,000–10,000 IU/day under monitoring, often combined with omega-3, curcumin, and a comprehensive anti-inflammatory protocol.
- Immune Resilience / Infection Prevention: 2,000–5,000 IU/day during cold and flu season, with short-term increases (10,000–20,000 IU/day for 3–5 days) at the onset of acute illness.
- Osteoporosis and Fracture Prevention: 2,000–5,000 IU/day D3 + K2 + calcium (from food) + magnesium + weight-bearing exercise.
- Pregnancy: 4,000–6,000 IU/day D3 with K2, beginning preconception and continuing throughout pregnancy and lactation.
- Depression and SAD: 2,000–5,000 IU/day as part of a comprehensive mood-support protocol including omega-3, B vitamins, and magnesium.
- Type 2 Diabetes Prevention: 4,000 IU/day (per the D2d trial) for individuals with prediabetes, targeting 25(OH)D above 40 ng/mL.
- PCOS: 2,000–5,000 IU/day as adjunctive support for insulin sensitivity, hormonal balance, and ovulatory function.
- Psoriasis: Topical calcipotriol plus systemic D3 optimization for comprehensive psoriasis management.
- Coimbra Protocol (Autoimmune): High-dose Vitamin D (40,000–200,000 IU/day) under strict medical supervision with calcium-restricted diet and monitoring — used by some practitioners for severe autoimmune diseases including MS, lupus, and psoriasis. This is a specialized protocol requiring expert guidance.
Historical Medical Use & the Dosing Story (1926–1972)
Vitamin D has one of the most dramatic dosing histories in all of medicine — a story that swings from a genuine miracle cure to a near-forgotten danger and back to a modern, evidence-based middle ground. Understanding that arc helps make sense of the wildly different numbers patients still encounter online today, from the official 600 IU to claims that “everyone needs 10,000 IU.”
The Rickets Cure (1920s–1930s)
- A real, well-earned triumph. In the 1920s, rickets — the bone-softening disease that left children with bowed legs, widened wrists, and deformed chests — was epidemic in the smoky, sun-starved industrial cities of Europe and the northern United States. The discovery that both cod liver oil and ultraviolet light could prevent and cure it was one of the great nutritional victories of the era. By the early 1930s, “the antirachitic factor” had been chemically identified as vitamin D, and the routine fortification of milk that followed essentially erased childhood rickets across the developed world. This is honest history: vitamin D really did cure rickets, and it remains the textbook example of a vitamin deficiency disease conquered by a single nutrient.
- Why it worked. Vitamin D enables the gut to absorb calcium and phosphorus and lets the bone-building cells lay down hard mineral. Without it, even a calcium-rich diet cannot mineralize growing bone — which is why sunlight, cod liver oil, and later fortified milk all worked through the same final pathway. (See the Bone Health section above.)
The 1972 Megadose Era
- What an older medical text described. Mid-century clinicians, impressed by vitamin D’s power over bone disease, experimented with very large doses for inflammatory and autoimmune conditions. An older (circa 1972) medical reference described using doses on the order of ~280,000 IU of vitamin D for certain autoimmune problems — a number that, taken out of context, has resurfaced in modern videos as evidence that “doctors used to give enormous doses.”
- The honest reframe — this is dangerous as a routine dose. Treat that figure as a historical artifact, not a recommendation. 280,000 IU taken as a routine or daily-type dose is hazardous. Sustained intake at anywhere near that level drives hypervitaminosis D, in which the body absorbs and mobilizes far too much calcium, producing hypercalcemia — nausea, excessive thirst and urination, confusion, kidney stones, kidney injury, soft-tissue and vascular calcification, and dangerous heart-rhythm disturbances. (The Toxicity and Safety section above details the mechanism.) Unlike sunlight, which the skin self-limits through photodegradation, swallowed vitamin D has no such safety brake.
- The pendulum swung back. Later editions of that same reference quietly dropped the megadose recommendations and aligned with the conventional figure of roughly 600 IU/day. Meanwhile, a parallel camp of integrative practitioners argued the opposite — that 600 IU is far too little and that most people need several thousand IU per day, with some claiming 6,000–10,000 IU/day. So patients today are caught between a discredited megadose, a deliberately conservative RDA, and louder-than-the-evidence claims for 10,000 IU.
The Evidence-Based Middle Ground (Today)
The way out of this confusion is the single most important point on this whole page: do not chase a dose — chase a blood level. Vitamin D status is measured by a simple blood test, 25-hydroxyvitamin D [25(OH)D], and the dose that gets one person to a healthy level can be too little or too much for another (body size, baseline level, skin tone, absorption, and obesity all change the math). The honest, defensible numbers are:
- RDA (the floor for healthy people): 600 IU/day for most children and adults, 800 IU/day after age 70. This is the amount set to prevent deficiency in the general population — not necessarily to reach the higher levels some studies associate with broader benefit.
- Tolerable Upper Intake Level (the safe ceiling for routine, unmonitored use): 4,000 IU/day for adults. Routinely exceeding this without testing is where avoidable trouble begins.
- The practical reality for many adults: 1,000–4,000 IU/day is frequently what it takes to move a low or insufficient 25(OH)D up into the sufficient range, especially for people who are darker-skinned, older, heavier, indoors, or living at northern latitudes. This range sits comfortably under the upper limit and reaches sufficiency for most people.
- On 10,000 IU/day: this is not an appropriate blanket recommendation. Short repletion courses or genuinely high needs are handled under clinical supervision with periodic 25(OH)D and serum-calcium monitoring — not adopted indefinitely by everyone because a video said so. (Higher physician-monitored protocols exist for specific conditions; see Special Therapeutic Applications above.)
Within that framework, the real benefits the deficiency story points to are genuine — but they come from reaching sufficiency, not from megadosing past it:
- Immunity: correcting deficiency modestly lowers the risk of respiratory infections, with the largest benefit in the most deficient people (see the Immune System section) — pushing an already-sufficient level higher does not add protection.
- Mood: the clearest mood improvements appear when a low baseline level is restored, not when a normal level is pushed into excess (see Mental Health).
- Musculoskeletal & back pain: the diffuse bone and muscle pain of deficiency (osteomalacia) and proximal muscle weakness improve as 25(OH)D normalizes — this is repletion correcting a deficiency, not a painkiller effect of high doses.
- Pregnancy, infant skeleton & teeth: adequate maternal vitamin D supports fetal bone mineralization and tooth development and prevents neonatal rickets; a controlled trial found 4,000 IU/day safe and effective in pregnancy for reaching sufficiency — again, achieving a target level, not megadosing (see Pregnancy and Fetal Development).
In short: the 1920s rickets cure was real, the 1972 megadose was a wrong turn, and the modern answer is to test your 25(OH)D, supplement within the 600–4,000 IU range to reach sufficiency, pair vitamin D with vitamin K2 and magnesium, and recheck rather than guessing with an arbitrary — and potentially dangerous — large number.
Key Research Papers — History & Dosing
- Holick MF. Vitamin D Is Not as Toxic as Was Once Thought: A Historical and an Up-to-Date Perspective. Mayo Clinic Proceedings. 2015;90(5):561–564.
- Holick MF. Vitamin D Deficiency. New England Journal of Medicine. 2007;357(3):266–281.
- Holick MF, Binkley NC, Bischoff-Ferrari HA, et al. Evaluation, Treatment, and Prevention of Vitamin D Deficiency: an Endocrine Society Clinical Practice Guideline. The Journal of Clinical Endocrinology & Metabolism. 2011;96(7):1911–1930.
- Hollis BW, Johnson D, Hulsey TC, Ebeling M, Wagner CL. Vitamin D supplementation during pregnancy: Double-blind, randomized clinical trial of safety and effectiveness. Journal of Bone and Mineral Research. 2011;26(10):2341–2357.
Live PubMed searches: vitamin D toxicity / hypercalcemia · 25(OH)D targets & sufficiency · vitamin D in pregnancy & rickets.
Final Thoughts
Vitamin D3 is not merely a vitamin — it is a hormone, a gene regulator, an immune commander, and a guardian of nearly every major organ system in the human body. Its influence spans from the mineralization of the fetal skeleton to the prevention of cancer in old age, from the first immune response against a respiratory pathogen to the last defense against autoimmune self-destruction. The modern epidemic of Vitamin D deficiency — born of indoor lifestyles, sunscreen culture, northern latitudes, and dark skin at high latitudes — represents one of the most significant and correctable public health challenges of our time. In natural medicine, optimizing Vitamin D3 — alongside its essential partners K2 and magnesium — is not an option but a foundational imperative for every patient, at every age, in every condition. The evidence is overwhelming, the intervention is safe and affordable, and the potential benefits are nothing less than transformative.
We evolved under the sun, and our bodies still carry its ancient wisdom in every cell that bears a Vitamin D receptor. Honor that evolutionary heritage — seek the light, nourish the hormone, and let the sunshine vitamin illuminate the path to health from the inside out.
Connections
- How Your Skin Makes Vitamin D — interactive animation
- Bone Remodeling & Calcium Balance — interactive animation
- Vitamin D Deficiency — symptoms, causes, and recovery
- Vitamin D Toxicity — hypervitaminosis D symptoms, causes, and risks
- Vitamin K2 (Menaquinone) — the partner vitamin that directs the calcium D3 absorbs
- Calcium
- Calcium and Muscle Function — excitation-contraction coupling, cramps, tetany, and the calcium-magnesium balance for cardiac and skeletal muscle.
- Cancer
- Depression
- Diabetes
- Phosphorus
- Osteoporosis
- Vitamin D and Surgical Recovery
- Vitamin D3 and Bone Health
- Vitamin D3 and Immune System
- Vitamin D3 and Cancer Prevention
- Magnesium
- Psoriasis
- Vitamin D Test
- PCOS
- Cardiovascular Disease
- Insulin Resistance
- Celiac Disease
- Vitamin A
- Omega-3 Fatty Acids