Fibromyalgia and ME/CFS Overlap
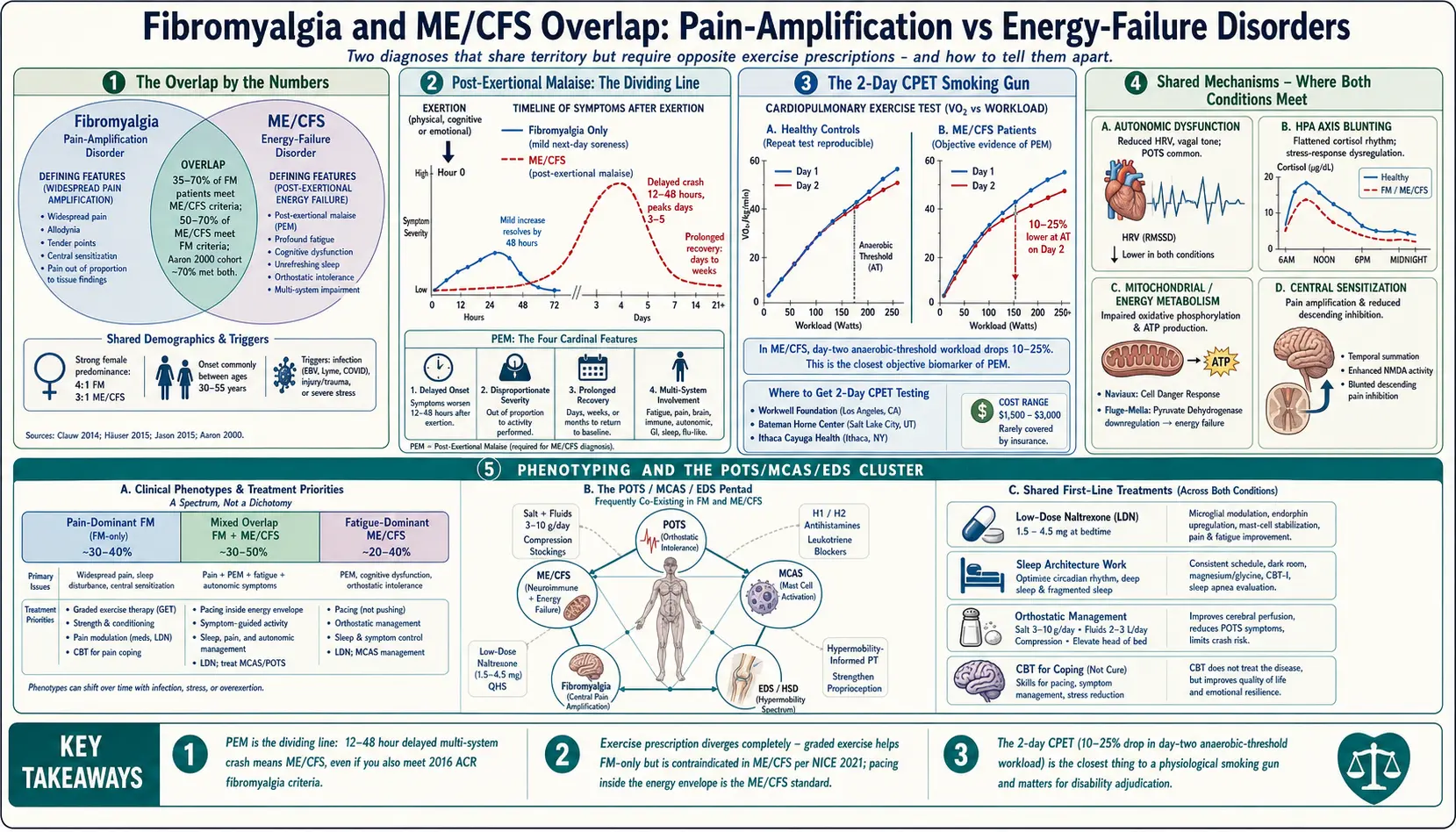
Table of Contents
- Why the Distinction Matters
- The Overlap by the Numbers
- Post-Exertional Malaise — The Dividing Line
- Three Criteria Sets Side by Side
- Shared Biological Mechanisms
- The 2-Day CPET — Objective PEM Proof
- Phenotyping: Pain-Dominant, Fatigue-Dominant, Mixed
- The POTS / MCAS / EDS Cluster
- Exercise: Where the Two Diverge Completely
- Treatments That Work for Both
- Which Diagnosis to Pursue — Disability & Insurance
- Practical Steps If You Suspect Both
- Key Research Papers
- Connections
- Featured Videos
Why the Distinction Matters
If you have been diagnosed with fibromyalgia and the standard exercise advice made you dramatically worse — not just sore for a day, but wiped out for a week — you may not have "just fibromyalgia." You may have myalgic encephalomyelitis / chronic fatigue syndrome (ME/CFS) layered on top, or instead. The two conditions share so much surface territory that primary-care doctors routinely lump them together, but the treatments that help one can actively harm the other.
Fibromyalgia is, at its core, a pain amplification disorder. The central nervous system turns the volume up on every sensory signal, producing widespread pain, tenderness, and a constellation of cognitive and sleep symptoms. ME/CFS, by contrast, is a post-exertional energy disorder. Its defining feature is that any exertion — physical, cognitive, or emotional — triggers a delayed, prolonged crash that can last days, weeks, or permanently worsen the baseline.
This article walks through where the two diagnoses overlap, where they split, and why getting the label right — or recognizing that both apply — changes everything about exercise prescription, pacing strategy, disability paperwork, and your long-term trajectory.
The Overlap by the Numbers
The diagnostic overlap is enormous. Depending on which study you read:
- 50–70% of ME/CFS patients also meet criteria for fibromyalgia.
- 35–70% of fibromyalgia patients also meet criteria for ME/CFS.
- In the landmark 2000 Aaron study of 127 patients, roughly 70% met criteria for both conditions simultaneously.
- Both conditions show a strong female predominance (roughly 4:1 in fibromyalgia, 3:1 in ME/CFS).
- Both typically appear between ages 30 and 55, often following an infection, injury, or severe stressor.
That level of overlap is not coincidence. It suggests the two labels are carving out partly the same underlying biology from different angles — pain specialists see "fibromyalgia," fatigue specialists see "ME/CFS," and the patient in the middle ends up with whichever label their first specialist happened to use.
Post-Exertional Malaise — The Dividing Line
If there is one symptom that separates ME/CFS from fibromyalgia cleanly, it is post-exertional malaise, or PEM. PEM is not ordinary post-workout fatigue. It has four defining features:
- Delayed onset. The crash usually hits 12–48 hours after the exertion, not during it. You can feel fine at the gym and collapse two days later.
- Disproportionate severity. A grocery trip or a long phone call can produce the same flattening that a marathon would produce in a healthy person.
- Prolonged recovery. Days to weeks, sometimes months. Severe episodes can drop a patient's baseline permanently.
- Multi-system symptoms. PEM is not just fatigue. It includes cognitive "brain fog," flu-like malaise, sore throat, tender lymph nodes, orthostatic symptoms, and widespread pain — a whole-body crash, not just tiredness.
Fibromyalgia patients get sore after overdoing it. ME/CFS patients get sick, for a long time, and the sickness does not respond to rest in the ordinary way. A fibromyalgia patient who pushes through a bad workout might need a heating pad and an extra nap. An ME/CFS patient who pushes through the same workout might lose the next three weeks of their life.
If PEM is present, treatment strategy changes fundamentally. Graded exercise therapy (GET), which has modest evidence in fibromyalgia, is contraindicated in ME/CFS. The 2021 NICE guidelines in the UK formally withdrew GET as a recommended treatment for ME/CFS after two decades of patient reports of harm and a re-analysis of the underlying trial data. The replacement strategy is pacing — staying inside an "energy envelope" rather than trying to expand it through progressive overload.
Three Criteria Sets Side by Side
Three major criteria sets govern these diagnoses. Knowing which one your doctor is using tells you a great deal about what they will look for and miss.
2016 ACR Fibromyalgia Criteria
The American College of Rheumatology's 2016 revision replaced the old tender-point exam with two questionnaires: the Widespread Pain Index (WPI), which counts painful body regions (0–19), and the Symptom Severity Scale (SSS), which scores fatigue, unrefreshing sleep, cognitive symptoms, and somatic complaints (0–12). Diagnosis requires either WPI ≥ 7 + SSS ≥ 5, or WPI 4–6 + SSS ≥ 9, with symptoms present at similar levels for at least three months. Crucially, fibromyalgia can now coexist with other diagnoses — the old "diagnosis of exclusion" requirement was dropped.
IOM / NAM 2015 SEID Criteria
In 2015, the Institute of Medicine (now the National Academy of Medicine) proposed renaming ME/CFS to Systemic Exertion Intolerance Disease (SEID) and simplified the diagnostic criteria to four core features, all required:
- Substantial reduction in pre-illness activity level for at least six months, accompanied by profound fatigue that is not relieved by rest.
- Post-exertional malaise.
- Unrefreshing sleep.
- At least one of: cognitive impairment, or orthostatic intolerance.
The SEID name never fully caught on, but the criteria themselves are the most clinician-friendly and are widely used in primary care and disability evaluations. They explicitly center PEM, which is the whole point.
Canadian Consensus Criteria (CCC, 2003) and ICC (2011)
The older Canadian Consensus Criteria and the stricter International Consensus Criteria (ICC) are still preferred by specialist clinics and research cohorts. They require PEM plus multiple symptoms from neurological, immune, autonomic, and energy-production categories. They identify a more severely affected subgroup than the IOM criteria and are the default for rigorous research. If you are pursuing specialty care at a center like Bateman Horne or Stanford's ME/CFS Clinic, expect the CCC or ICC to be used.
How the Criteria Interact
A patient can meet all three. Many do. Meeting the 2016 ACR fibromyalgia criteria does not exclude ME/CFS, and meeting IOM SEID criteria does not exclude fibromyalgia. In practice, if you have widespread pain plus PEM plus unrefreshing sleep plus cognitive symptoms, you likely qualify for both labels, and the correct diagnostic statement is "fibromyalgia and ME/CFS" rather than one or the other.
Shared Biological Mechanisms
Three biological systems keep turning up in both conditions, which is probably why the overlap is so large.
Autonomic Dysfunction
Both groups show abnormal heart-rate variability, reduced vagal tone, and a tendency toward orthostatic intolerance — symptoms on standing, including lightheadedness, palpitations, and fatigue. A sizable minority of patients in both groups meet criteria for postural orthostatic tachycardia syndrome (POTS). Tilt-table testing often reveals findings that explain the fainting, the "gravity is heavy" feeling, and the inability to stand in line at the grocery store. See the POTS page and the POTS/MCAS/EDS triad deep-dive.
HPA Axis Blunting
The hypothalamic-pituitary-adrenal axis — the body's main stress-response system — is measurably flattened in both fibromyalgia and ME/CFS cohorts. Morning cortisol tends to be low, the normal diurnal rhythm is blunted, and the reactivity to stress is reduced. This is not the same as Addison's disease (cortisol is not pathologically low, just suboptimal), but it helps explain why patients struggle with morning stiffness, post-stress crashes, and poor recovery from ordinary challenges.
Mitochondrial and Energy Metabolism Dysfunction
Research over the last decade has found reproducible abnormalities in cellular energy production in ME/CFS — impaired oxidative phosphorylation, altered pyruvate dehydrogenase activity, and a shift toward anaerobic metabolism at low workloads. Fibromyalgia patients show a milder version of the same signature. Naviaux's "cell danger response" framework and Fluge and Mella's pyruvate dehydrogenase work both describe a state in which cells behave as though they are still fighting a threat and cannot fully return to normal energy production. This is a plausible explanation for why the two conditions share fatigability, exercise intolerance, and the characteristic "wired but tired" sleep pattern.
Central Sensitization
On the pain side, both groups show central sensitization — an amplified, over-reactive pain-processing system. Temporal summation, the phenomenon where repeated mild stimuli build into severe pain, is exaggerated. Descending pain inhibition (the brain's ability to turn down incoming pain signals) is weaker. This is better studied in fibromyalgia but is clearly present in ME/CFS as well. See the central sensitization article for the full mechanism.
The 2-Day CPET — Objective PEM Proof
One of the few objective tests that can document PEM is the two-day cardiopulmonary exercise test (CPET), developed and validated by Staci Stevens, Chris Snell, and Mark Van Ness at the Workwell Foundation, with seminal results published by Davenport and colleagues in 2010.
The protocol is simple in concept. The patient performs a maximal CPET on day one, measuring VO2 at peak and at the anaerobic threshold. They rest overnight. The next day, they repeat the identical test. Healthy people, sedentary people, people with heart failure, people with fibromyalgia without ME/CFS — all reproduce their day-one numbers within a few percentage points on day two. ME/CFS patients, uniquely, show a 10–25% drop in workload and VO2 at the anaerobic threshold on the second test. Their bodies cannot reproduce the effort, because the first test triggered PEM.
Why this matters:
- It is the closest thing to a physiological smoking gun for ME/CFS.
- Disability insurers and the Social Security Administration recognize CPET data far more readily than symptom questionnaires alone.
- It can objectively distinguish "fibromyalgia with fatigue" from "fibromyalgia plus ME/CFS," which changes treatment.
Caveats: the test is expensive (around $1,500–$3,000, rarely covered), it is offered at only a handful of U.S. centers (Workwell Foundation in California, Ithaca Cayuga Medical, Bateman Horne Center in Utah, and a few university labs), and the second-day test itself can worsen a severe patient for weeks. It is not something to do casually. But for patients fighting a disability denial, it can be decisive. See the ME/CFS page for more on testing strategy.
Phenotyping: Pain-Dominant, Fatigue-Dominant, Mixed
A useful clinical framework, whether or not your doctor uses this language explicitly, is to ask where your symptoms cluster:
Pain-Dominant Fibromyalgia
Widespread pain is the headline. Fatigue is present but manageable — you are tired, but you can push through a day of moderate activity and recover with a night's sleep. Exercise, done gently and progressively, tends to help. This phenotype responds reasonably well to duloxetine, milnacipran, low-dose naltrexone, and graded movement programs. Disability is driven by pain, not energy failure.
Fatigue-Dominant ME/CFS
Fatigue and PEM are the headline. Pain is present but not the main story — it may come and go with crashes rather than sitting at a steady level. Any exercise increment beyond your current envelope triggers a crash. Pacing, aggressive rest, orthostatic management, and avoiding GET are the pillars of treatment. Disability is driven by energy failure, not pain.
Mixed Phenotype
The largest group. Both the pain and the PEM are severe. These patients are often the most disabled and the hardest to treat, because every intervention has to account for both the pain-amplification side and the post-exertional-crash side. Gentle movement that respects PEM can still help, but the ceiling is lower and the margin for error is narrow.
Honest self-phenotyping is worth doing. Keep a two-week symptom log scoring pain (0–10) and fatigue/PEM (0–10) separately each day. The ratio of the two tells you which playbook to prioritize.
The POTS / MCAS / EDS Cluster
A large minority of fibromyalgia and ME/CFS patients — especially women in their 20s through 40s — cluster with three other diagnoses that travel together:
- POTS (postural orthostatic tachycardia syndrome) — heart rate rises more than 30 beats per minute on standing, with symptoms.
- MCAS (mast cell activation syndrome) — flushing, hives, food intolerances, GI symptoms, and reactions to medications and temperature changes.
- Hypermobile EDS or generalized joint hypermobility — stretchy skin, bendy joints, velvet-soft skin, frequent subluxations.
When three or four of these co-occur in the same patient, it is sometimes called the fibromyalgia-POTS-MCAS-EDS pentad. Treatment becomes a coordinated effort: H1/H2 blockers for MCAS, salt loading and compression for POTS, pacing for ME/CFS, LDN for pain, and physical therapy calibrated for hypermobility. See the POTS/MCAS/EDS triad deep-dive for the full protocol. Recognizing the cluster matters because treating one node in isolation often fails; the others keep pulling the patient backward.
Exercise: Where the Two Diverge Completely
This is the single most important practical difference, and it is the one most often mishandled.
For fibromyalgia without PEM, graded aerobic exercise has moderate evidence of benefit. Trials of walking, swimming, tai chi, and yoga show reduced pain, improved sleep, and better function at 12 weeks. The protocol is the usual one: start low, increase by no more than 10% per week, expect mild soreness, do not push through sharp pain. See the graded movement article.
For ME/CFS (or fibromyalgia with PEM), the same protocol is actively dangerous. The 2011 PACE trial, which originally endorsed graded exercise therapy, has been extensively re-analyzed and its positive findings largely reversed. Real-world patient surveys consistently report that GET worsens their condition, sometimes permanently. The 2021 NICE guidelines in the UK, the CDC, and the U.S. ME/CFS clinical coalition all now advise against GET and in favor of pacing.
Pacing means staying inside your energy envelope. The practical tools:
- A heart-rate monitor set to alert at your anaerobic threshold (commonly estimated at 55–60% of max HR for ME/CFS patients, or from CPET data if available). Stay below the alert.
- An activity diary tracking hours of upright activity, cognitive exertion, and social exertion against next-day symptoms.
- Planned rest before symptoms appear, not after.
- Reducing the envelope voluntarily during flares, viral illness, or emotional stress.
See the pacing and energy envelope article for the full protocol.
Treatments That Work for Both
Despite the divergence on exercise, a surprising amount of treatment overlaps. These interventions help both fibromyalgia and ME/CFS patients at reasonable rates:
- Low-dose naltrexone (LDN). At 1.5–4.5 mg nightly, LDN reduces central sensitization and microglial activation. It has randomized-controlled-trial evidence in fibromyalgia and observational evidence in ME/CFS. Inexpensive, well tolerated, worth trying for most patients in either group. See the LDN article.
- Sleep architecture work. Both conditions feature deep-sleep disruption. Low-dose doxepin, mirtazapine, or trazodone; consistent sleep/wake timing; light exposure in the morning; sleep-study evaluation for comorbid apnea or periodic limb movements. See the sleep architecture article.
- Orthostatic management. Increased salt (3–10 g/day) and fluid (2–3 L/day), compression garments (waist-high, 20–30 mmHg), and beta blockers or midodrine where appropriate.
- Cognitive behavioral therapy aimed at coping, not at "curing" the illness. CBT does not fix either condition, but it can reduce the secondary suffering of living with chronic illness.
- Nutritional basics. Vitamin D repletion, B12 if low, magnesium glycinate for sleep and muscle pain, and treating iron deficiency aggressively.
Treatments that help fibromyalgia but often fail or worsen ME/CFS include antidepressants at activating doses, progressive aerobic exercise, and — in some patients — stimulant-based therapies that can push the patient over their energy envelope and into a crash.
Which Diagnosis to Pursue — Disability & Insurance
If you are applying for Social Security Disability, long-term disability insurance, or workplace accommodations, the label on the paperwork matters more than you would hope it should.
Fibromyalgia is formally recognized by the SSA under SSR 12-2p. Claims succeed when there is a documented history from a rheumatologist, tender-point or WPI/SSS evidence, and functional limitations. Fibromyalgia is easier to get diagnosed and somewhat easier to get approved, but benefit awards for fibromyalgia alone tend to be more modest and more frequently reviewed.
ME/CFS is formally recognized by the SSA under SSR 14-1p, which explicitly accepts the diagnosis when made according to CDC criteria and supported by signs such as tender lymph nodes, non-exudative pharyngitis, or abnormal CPET findings. SSR 14-1p is often more favorable for severely disabled patients because it acknowledges that ME/CFS can produce complete work incapacity.
Practical strategy when both apply:
- List both diagnoses on every form. Do not pick one and drop the other.
- Ask your physician to document PEM explicitly with examples. Vague notes like "fatigue" carry far less weight than "patient reports 3–5 day functional collapse after 20 minutes of housework."
- If possible, obtain 2-day CPET data. It is the most powerful objective evidence either condition has.
- Keep a functional diary for several months before applying — hours of upright activity, hours of work capacity, crashes and their triggers.
- Consider a disability attorney experienced with ME/CFS specifically. It usually costs nothing upfront (contingency fee) and dramatically improves approval odds.
Practical Steps If You Suspect Both
- Score yourself. Take the 2016 ACR questionnaire (WPI + SSS) and the IOM SEID checklist. Write down your scores.
- Log symptoms for two weeks. Pain 0–10, fatigue 0–10, PEM episodes, triggers. Bring the log to your doctor.
- Test orthostatic vitals at home. Lie flat for 10 minutes, measure HR and BP. Stand. Measure again at 1, 3, 5, and 10 minutes. A heart-rate increase greater than 30 beats per minute (or 40 in teenagers) flags POTS.
- Ask for a rheumatology referral (for the fibromyalgia side) and an ME/CFS-literate clinician (for the PEM side). The Bateman Horne Center, ME/CFS Clinical Coalition, and Solve ME/CFS Initiative all maintain provider lists.
- Stop GET if it is making you worse. You are not imagining it. The protocol is wrong for your physiology.
- Start pacing conservatively while you sort out the full diagnostic picture. There is no downside to staying inside your envelope.
- Consider LDN early. Inexpensive, well-tolerated, and it helps both conditions.
Key Research Papers
- Institute of Medicine. Beyond Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: Redefining an Illness. National Academies Press, 2015. (IOM / SEID criteria)
- Aaron LA, Burke MM, Buchwald D. Overlapping conditions among patients with chronic fatigue syndrome, fibromyalgia, and temporomandibular disorder. Arch Intern Med. 2000;160(2):221–227.
- Davenport TE, Stevens SR, VanNess JM, Snell CR, Little T. Conceptual model for physical therapist management of chronic fatigue syndrome/myalgic encephalomyelitis. Phys Ther. 2010. (2-day CPET framework)
- Wolfe F, et al. 2016 Revisions to the 2010/2011 fibromyalgia diagnostic criteria. Semin Arthritis Rheum. 2016.
- Fluge Ø, Mella O, et al. Metabolic profiling indicates impaired pyruvate dehydrogenase function in myalgic encephalopathy/chronic fatigue syndrome. JCI Insight. 2016.
- Bateman L, et al. Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: Essentials of Diagnosis and Management. Mayo Clin Proc. 2021.
Live PubMed Searches
For further reading, the following PubMed topic searches return current peer-reviewed work on the fibromyalgia / ME/CFS overlap and its management:
- Fibromyalgia and chronic fatigue syndrome overlap
- Post-exertional malaise in ME/CFS
- Two-day CPET and chronic fatigue syndrome
- Graded exercise therapy and reported harm in ME/CFS
- Pacing and the energy envelope concept
- Autonomic dysfunction in fibromyalgia and ME/CFS
- HPA axis findings across both conditions
- Low-dose naltrexone in fibromyalgia and ME/CFS
- POTS, MCAS, and fibromyalgia cluster
- 2016 ACR fibromyalgia diagnostic criteria
Connections
- POTS
- Chronic Fatigue Syndrome
- POTS/MCAS/EDS Triad
- Low-Dose Naltrexone for Fibromyalgia
- Sleep and Non-Restorative Sleep
- Central Sensitization Explained
- Exercise Pacing and Graded Movement
- MCAS
- Fibromyalgia Overview
- ACR 2016 Diagnostic Criteria
- Low-Dose Naltrexone
- Chronic Pain
- Fatigue
- Nutrient Gaps in Fibromyalgia
- Small-Fiber Neuropathy Overlap
- Post-Viral Triggers in ME/CFS
- Magnesium
- Post Exertional Malaise Explained