Low-Dose Naltrexone (LDN): The Off-Label Immunomodulator Redefining Chronic Illness Care
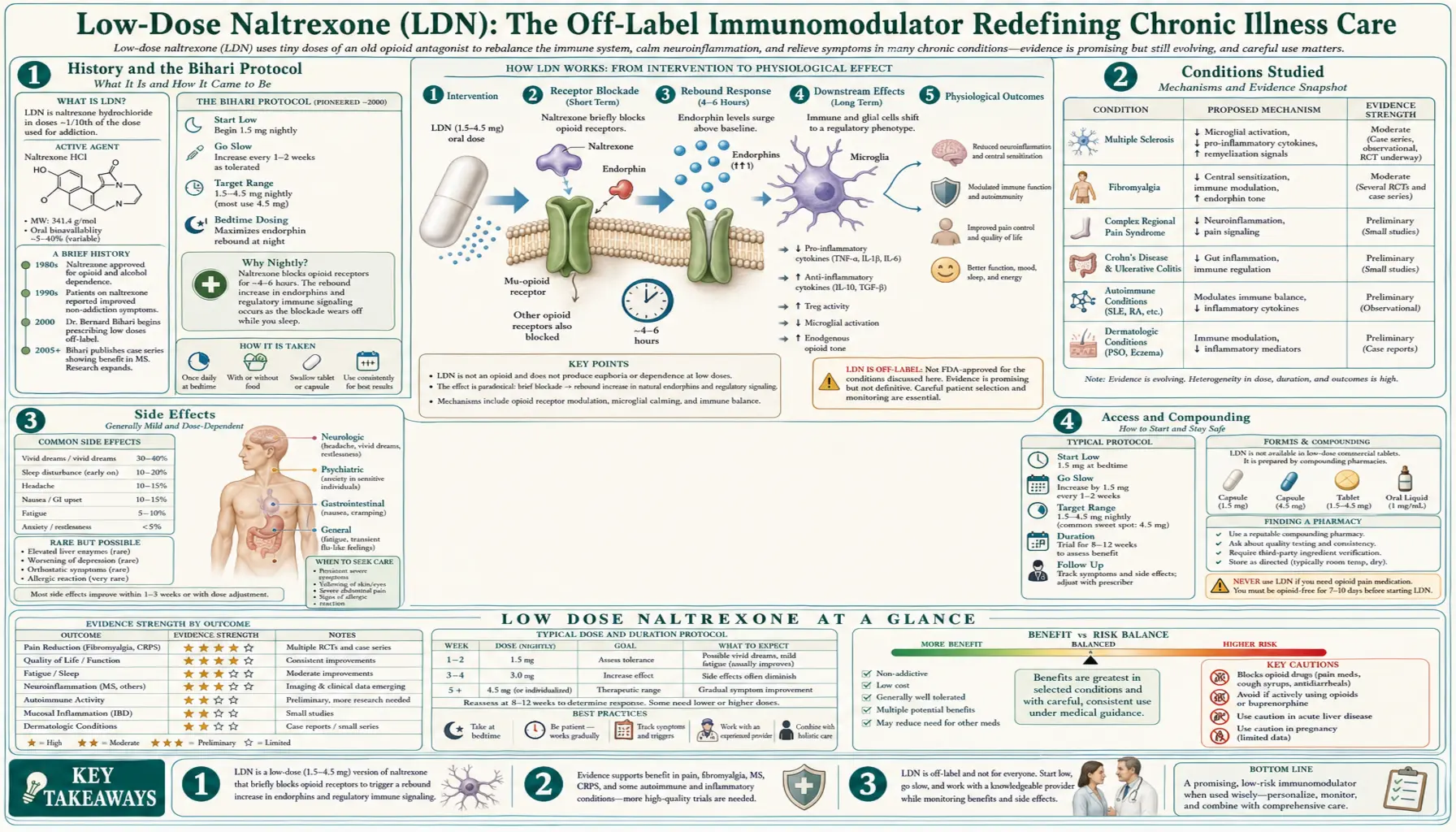
Naltrexone is a pure opioid-receptor antagonist first approved in 1984 at a daily oral dose of 50 mg for alcohol use disorder and opioid use disorder. In 1985, physician Bernard Bihari observed that at roughly one-tenth that dose — now called low-dose naltrexone (LDN) — the drug produced entirely different effects: modulation of the immune system, reduction of inflammatory cytokines, and in some patients, substantial improvement in autoimmune disease and chronic pain. The mechanism differs from standard-dose naltrexone and centers on brief nightly opioid-receptor blockade, rebound endorphin release, and direct effects on glial cells in the central nervous system.
Today LDN is used off-label for a long list of chronic-inflammatory and autoimmune conditions. This article explains the mechanism, the evidence base, common dosing, side effects, and where LDN fits in an evidence-informed chronic-illness protocol.
Table of Contents
- History and the Bihari Protocol
- Mechanism — Three Pathways
- Conditions Studied
- Dosing and Titration
- Side Effects
- Important Considerations and Contraindications
- Access and Compounding
- Connections
- Featured Videos
History and the Bihari Protocol
Low-dose naltrexone traces to Dr. Bernard Bihari (1931–2010), a Harvard-trained New York addiction physician who first observed its apparent immune effects in HIV/AIDS patients in 1985–1986 and later extended it to autoimmune disease and cancer. Because naltrexone’s patent had long expired, no sponsor has carried LDN through large-scale FDA trials, so the evidence remains a patchwork of small studies and clinical experience — the fuller story is told in the dedicated History article.
Mechanism — Three Pathways
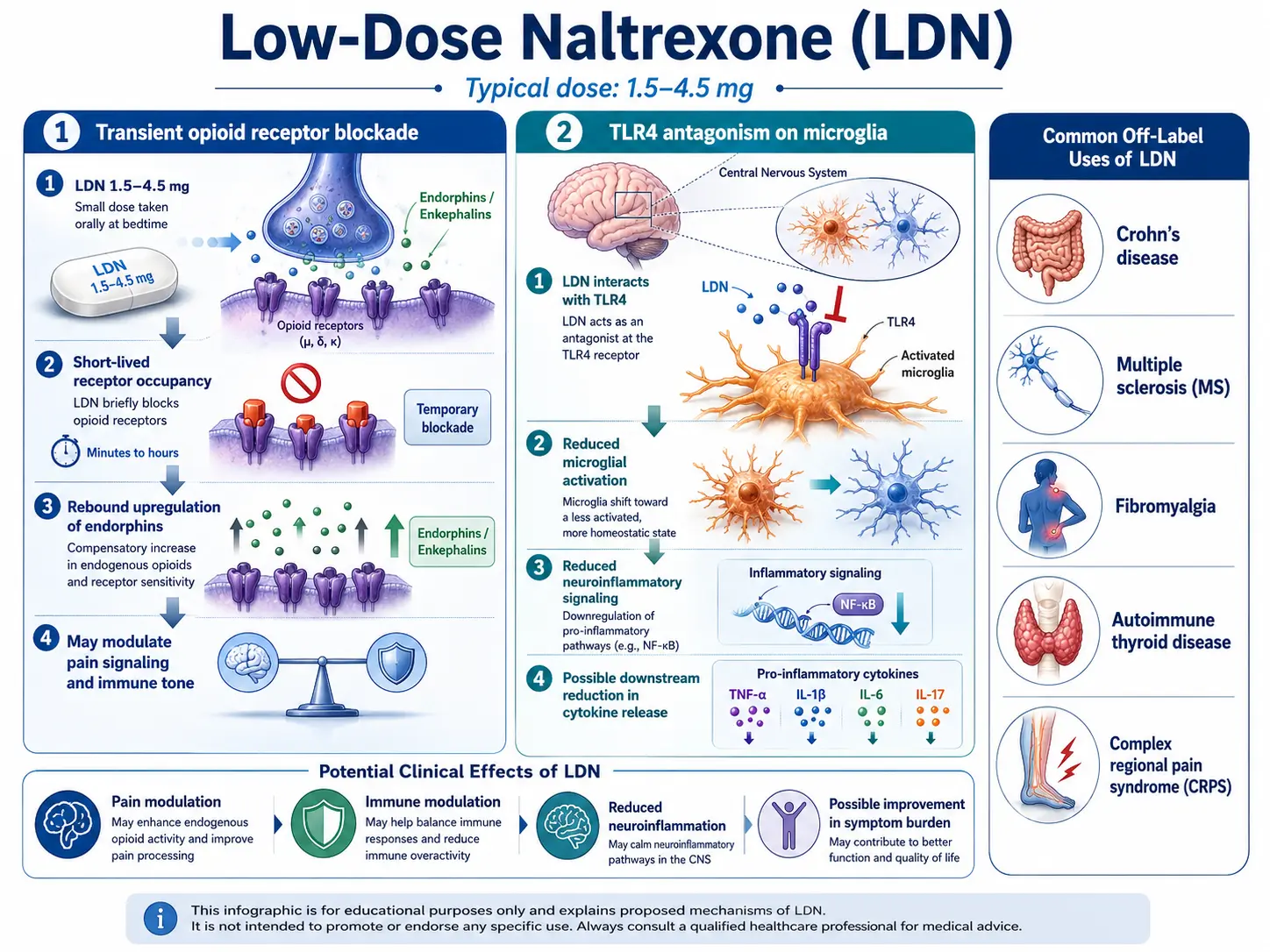
- Transient opioid-receptor blockade with endorphin rebound. Taking a low dose at bedtime produces a brief (4–6 hour) blockade of mu-opioid receptors. The body responds by increasing production of endogenous opioids and enkephalins, which then act on immune cells bearing opioid receptors, modulating cytokine balance toward a less inflammatory profile.
- Toll-like receptor 4 (TLR4) antagonism on microglia. LDN directly inhibits TLR4 on central-nervous-system glial cells, reducing the pro-inflammatory cascade implicated in chronic pain, fibromyalgia, and neuroinflammation.
- Direct effects on regulatory T cells and natural killer cells. LDN has been shown to normalize regulatory T-cell activity and enhance NK-cell function, relevant in both autoimmunity and cancer biology.
Conditions Studied
LDN has been studied or is commonly used off-label for:
- Multiple sclerosis. Randomized trials and observational data suggest reduced fatigue, spasticity, and quality-of-life benefit.
- Crohn’s disease. A placebo-controlled trial showed induction of remission in roughly 67% of patients versus 17% on placebo.
- Fibromyalgia. Small crossover trials have shown meaningful pain reduction.
- Hashimoto’s thyroiditis. Case series and clinical reports describe reduced TPO antibodies and improved symptoms.
- Chronic pain and complex regional pain syndrome. TLR4-mediated benefit.
- Psoriasis, lupus, and systemic sclerosis. Case series and small studies.
- Long-COVID fatigue and post-viral syndromes. Open-label reports.
Dosing and Titration
The standard LDN range is 1.5 mg to 4.5 mg taken at bedtime. Titration typically starts at 0.5 mg or 1.5 mg and advances every 1–2 weeks as tolerated. Some patients respond best to lower doses (<3 mg). A subset of patients with central-sensitization syndromes or sleep disruption on the standard regimen tolerate morning dosing or ultra-low doses better. Because standard naltrexone tablets are 50 mg, LDN requires compounded capsules, sublingual drops, or quartering tablets.
Side Effects
- Vivid dreams or sleep disruption in the first 1–2 weeks. Usually settles.
- Mild headaches, nausea, or GI upset.
- Transient increase in symptoms in some autoimmune patients during the first month.
Important Considerations and Contraindications
- Opioid medications. LDN blocks opioid-receptor effects. Anyone using prescription opioids for pain should not use LDN concurrently, and LDN should not be started within 7 days of opioid discontinuation.
- Pregnancy. Safety data are limited; use is typically avoided.
- Acute hepatitis. Standard-dose naltrexone has a black-box warning for hepatotoxicity at very high doses; LDN doses are orders of magnitude lower, but liver enzymes should be monitored.
- Immunosuppressive therapies. LDN’s immunomodulation may interact with biologics; coordinate with prescribing clinician.
Access and Compounding
Because LDN doses do not exist in manufactured form, a compounding pharmacy must prepare the capsules. Many compounding pharmacies worldwide now specialize in LDN and can fill prescriptions through telemedicine. Quality varies — patients typically do better with immediate-release capsules than with slow-release formulations, because the transient blockade is part of the mechanism.
Research Papers
Selected PubMed topic searches relevant to low-dose naltrexone mechanisms, autoimmune disease, chronic pain, and immunomodulation.
- PubMed: Low-dose naltrexone and autoimmune disease
- PubMed: Low-dose naltrexone and fibromyalgia
- PubMed: Low-dose naltrexone and multiple sclerosis
- PubMed: Low-dose naltrexone and Crohn's disease
- PubMed: Naltrexone and opioid growth factor (OGF)
- PubMed: LDN and complex regional pain syndrome
- PubMed: Naltrexone, TLR4, and microglia
- PubMed: LDN and Hashimoto's thyroiditis
- PubMed: Low-dose naltrexone and cancer
- PubMed: Low-dose naltrexone and post-viral syndromes
- PubMed: Naltrexone pharmacokinetics at low dose
- PubMed: Naltrexone and endogenous endorphin rebound
Connections
- Chronic Pain
- Fibromyalgia
- Lupus
- Crohn's Disease
- Multiple Sclerosis
- Hashimoto's Thyroiditis
- POTS
- Fatigue
- Gut Healing
- Stress Management
- Thyroid Panel
- Inflammatory Markers
- Anti Inflammatory Diet
- Complex Regional Pain Syndrome
- Psoriasis
- Chronic Fatigue Syndrome
- Central Sensitization Explained
- Sjogrens Syndrome