Exercise Pacing and Graded Movement for Fibromyalgia
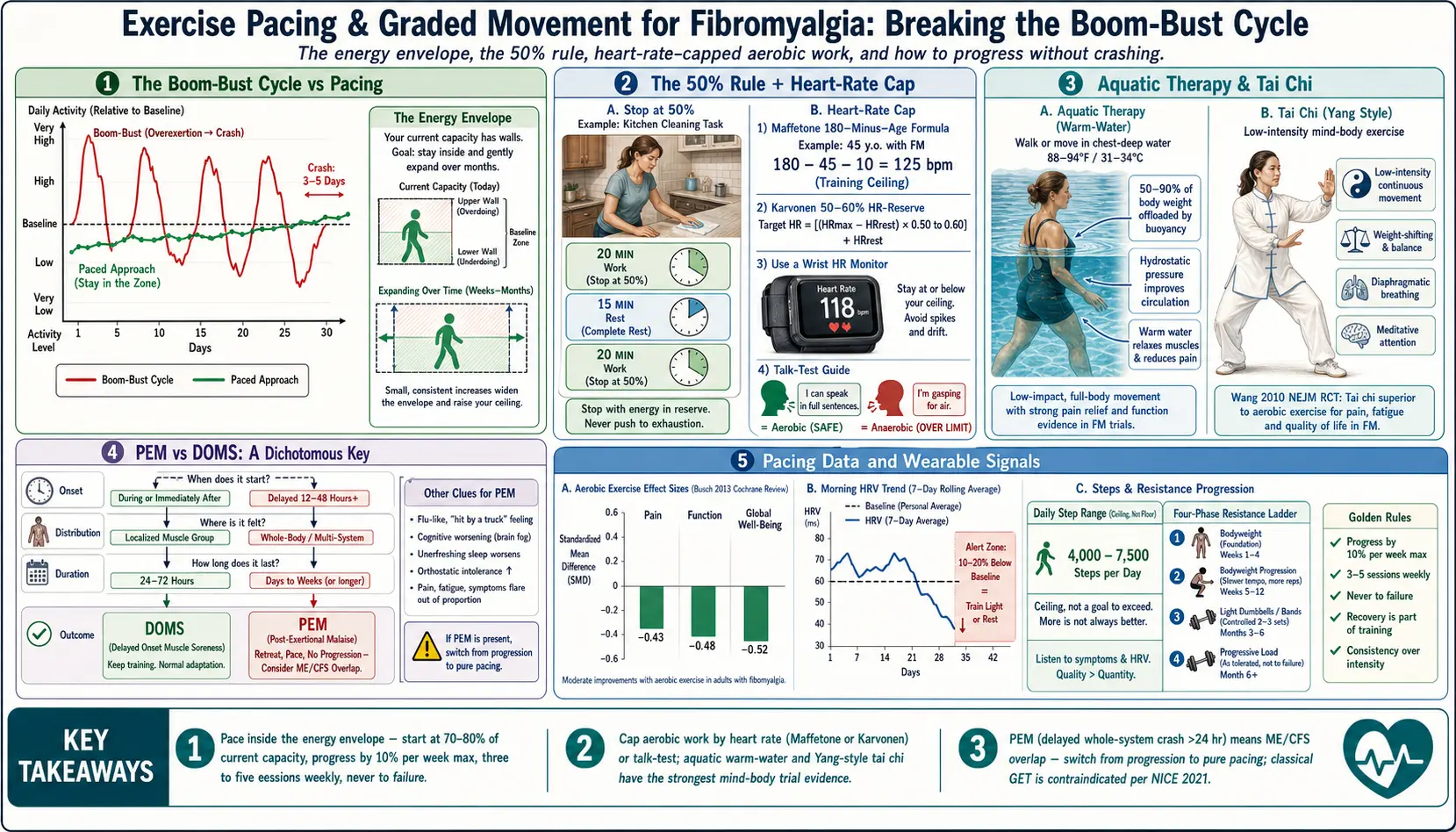
Table of Contents
- Why “Push Through the Pain” Backfires: The Boom-Bust Cycle
- The Pacing Envelope Concept
- Activity-Rest Balancing: The 50% Rule
- Graded Exercise Therapy (GET) Done Right
- How Fibromyalgia GET Differs from the Discredited PACE Protocol
- Heart-Rate-Capped Aerobic Work
- Aquatic Therapy: Warm Water Changes the Math
- Resistance Training: Starting Unloaded
- Tai Chi, Yoga, and Qigong
- Distinguishing Post-Exertional Malaise from Normal Soreness
- Using a Wearable to Track Load
- Practical Weekly Templates
- Common Pitfalls
- Key Research Papers
- Connections
- Featured Videos
Why “Push Through the Pain” Backfires: The Boom-Bust Cycle
Almost everyone with fibromyalgia has lived this pattern: a good day arrives, you feel close to normal, and you burn through a week’s worth of delayed chores in six hours — laundry, yard work, a long walk with a friend, maybe dinner out. The next morning you cannot get out of bed. Pain is everywhere, the fog is thick, sleep didn’t restore anything, and the crash lasts two, three, sometimes five days. By the time you recover, you are deconditioned again, and the cycle repeats.
This is the boom-bust cycle, and it is the single most destructive pattern in fibromyalgia self-management. Every crash costs more than it gained. The total work completed over a month is lower than it would be if you paced evenly, because you spend so many days below baseline recovering from the peaks. Worse, repeated crashes sensitize the central nervous system further — meaning pain, fatigue, and fog all get more reactive over time (see central sensitization explained).
The fix is not to do less. It is to do the same or slightly more, spread evenly, every day. The jargon word for this is pacing, and it is the foundation everything else in this article sits on.
The Pacing Envelope Concept
Imagine your daily capacity as a rectangle with walls you can feel but not see. Activity inside the rectangle — the “energy envelope” — costs nothing extra. Activity outside it triggers a crash 24–72 hours later. The goal of pacing is to find where your walls are and stay comfortably inside them while you slowly, deliberately push them outward over months.
To find your envelope, track two numbers for two weeks:
- Morning energy rating on a 0–10 scale (0 = can’t get out of bed, 10 = best day of your life).
- Activity completed — steps walked, minutes of exercise, hours of household work, hours of focused mental work.
After two weeks, look for the daily activity level at which your next-morning rating stays stable or rises. That is the top of your envelope. Start every training plan at 70–80% of that number. Not 100%. Training at the absolute edge is fragile — any poor night of sleep, minor illness, or life stress pushes you over.
Activity-Rest Balancing: The 50% Rule
A practical rule used by occupational therapists who treat fibromyalgia and ME/CFS: stop at 50% of what you think you can do, then rest. Then do the next 50% block. Then rest.
Example: you want to clean the kitchen. You estimate it would take 40 minutes of continuous work. Under the 50% rule, you work for 20 minutes, sit down for 15, then finish the remaining 20 minutes. Total clock time is 55 minutes instead of 40, but the cost to the nervous system is half. You also finish with capacity to spare, which is the whole point.
The rest intervals don’t have to be lying down. They are deliberate low-demand intervals — sitting with tea, listening to music, legs up against a wall, slow breathing. Scrolling a phone does not count as rest for fibromyalgia because it keeps cognitive load high.
Graded Exercise Therapy (GET) Done Right
Graded Exercise Therapy is the gradual, measured increase of activity over weeks and months. For fibromyalgia specifically, done correctly, it has the strongest evidence base of any non-drug intervention. The 2013 Cochrane review led by Busch and colleagues (DOI 10.1002/14651858.CD003786.pub2) pooled 34 studies of aerobic exercise in fibromyalgia and concluded that moderate-intensity aerobic training improves pain, function, and global well-being, with effect sizes small to moderate but consistent.
The recipe that works in the trials:
- Start absurdly low. If you can currently walk five minutes before a symptom flare, start at two minutes. Not five. Not ten. Two.
- Increase by 10% per week maximum. Two minutes becomes 2:12 next week, 2:25 the week after. If the next morning’s symptom rating drops, hold the current level an extra week before progressing.
- Three to five sessions per week, not daily. Recovery days matter as much as training days.
- Cap intensity at a level where you can still hold a full-sentence conversation. If you have to take a breath mid-sentence, you are above threshold and will pay for it tomorrow.
- Expect a flare in the first two to six weeks. Then the body adapts, and the same workload starts feeling easier. If it doesn’t adapt by week six, the starting dose was too high — drop back 50% and restart.
How Fibromyalgia GET Differs from the Discredited PACE Protocol
If you have read anything about ME/CFS in the last decade, you have seen the backlash against Graded Exercise Therapy. The UK’s 2011 PACE trial was the most influential study to promote GET and Cognitive Behavioral Therapy for ME/CFS. After a decade of patient advocacy and reanalysis, the trial’s protocol changes, outcome-measure switching, and modest effect sizes led the UK’s National Institute for Health and Care Excellence (NICE) to remove GET as a recommended treatment for ME/CFS in 2021.
This matters because some fibromyalgia patients — particularly those with heavy post-exertional malaise — have an ME/CFS-dominant phenotype in which any prescribed activity escalation makes them worse permanently. For those patients, classical GET is harmful.
The key differences between fibromyalgia GET and the discredited ME/CFS PACE approach:
- Fibromyalgia GET is patient-led and symptom-contingent. You do not progress on a fixed schedule if symptoms worsen — you hold or retreat. PACE progressed participants on a pre-set calendar regardless of crashes.
- Fibromyalgia GET caps intensity by heart rate or talk-test, not by time-at-effort.
- For patients with clear PEM (post-exertional malaise), the protocol becomes pacing without progression. The goal shifts from improvement to stability.
If you crash for more than 24 hours after any gentle activity session — not soreness, full-system crash — read the fibromyalgia and ME/CFS overlap article before designing a training plan.
Heart-Rate-Capped Aerobic Work
The cleanest way to keep exercise below the danger zone is to cap your heart rate. The goal is to stay aerobic — meaning your mitochondria have enough oxygen to make energy cleanly — and avoid crossing into anaerobic metabolism, which dumps lactate, spikes sympathetic drive, and is the dose most likely to trigger next-day flares.
Two useful formulas:
- Maffetone 180-minus-age (conservative). Take 180 and subtract your age. If you have a chronic illness or have been sedentary, subtract another 5–10. For a 45-year-old with fibromyalgia: 180 − 45 − 10 = 125 bpm ceiling. Stay at or below this during steady-state cardio.
- Karvonen heart-rate-reserve method, 50–60% zone. Target HR = resting HR + (0.50 to 0.60) × (220 − age − resting HR). For a 45-year-old with resting HR 70: target = 70 + 0.55 × (220 − 45 − 70) = 70 + 58 = 128 bpm.
Both formulas land in roughly the same window. Pick one, strap a heart-rate monitor to your wrist or chest, and when the number exceeds your cap, slow down. It really is that simple. Most people are shocked at how easy the pace must be at first — a stroll, not a brisk walk. That is correct. The adaptation happens with consistency, not intensity.
The talk test is a backup when you don’t have a monitor: you should be able to speak a full sentence without gasping. If you can only manage short phrases, you are too high.
Aquatic Therapy: Warm Water Changes the Math
For many people with fibromyalgia, water-based exercise is the only form that works without triggering flares. The reasons are mechanical and neurological:
- Buoyancy offloads 50–90% of body weight depending on water depth. Joint-loading pain drops to near-zero.
- Hydrostatic pressure improves circulation and reduces the orthostatic component that many fibromyalgia patients also carry.
- Warm water (88–94°F / 31–34°C) reduces muscle guarding and central pain sensitization by competing for the same sensory pathways that transmit pain.
- Resistance is proportional to effort — the faster you move, the more resistance. You cannot accidentally overload at a slow pace.
The 2017 Cochrane review on aquatic exercise for fibromyalgia led by Bidonde and colleagues concluded that aquatic training produces small-to-moderate improvements in pain, stiffness, and multidimensional function, with evidence quality ranging from low to moderate. The effect size is similar to land-based aerobic training, but drop-out rates are lower because tolerability is higher.
Practical notes: look for a pool kept at 88°F or warmer — standard lap pools at 78–82°F are too cold and will tighten muscles. Community YMCAs, hospital rehab pools, and arthritis-foundation aquatic programs often run warm-water sessions. Start with 20-minute sessions twice a week, alternating walking in chest-deep water with gentle arm sweeps. Do not use a kickboard for leg-only work at first — the floating horizontal position can spike neck and shoulder tension.
Resistance Training: Starting Unloaded
Muscle mass matters for fibromyalgia outcomes. Stronger muscles are less reactive to the same load, sleep quality tends to improve, and metabolic health — glucose regulation, bone density, mitochondrial function — all respond to resistance training in ways aerobic work alone cannot match. But the standard gym prescription (“start with the bar, add weight each session”) is too aggressive.
A fibromyalgia-appropriate progression:
- Phase 1 — Bodyweight or less, weeks 1–4. Wall push-ups, sit-to-stand from a chair, supine hip bridges, standing heel raises. Five to eight reps per set. One set per exercise. Twice per week. Yes, that’s all.
- Phase 2 — Full bodyweight, weeks 5–10. Push-ups on knees, bodyweight squats to a chair, glute bridges with a pause, assisted lunges holding a counter. Two sets. Still twice per week.
- Phase 3 — Light external load, month 3 onward. Dumbbells in the 2–8 lb range, resistance bands, suspension trainers. Two to three sets of 8–12 reps.
- Phase 4 — Progressive loading, month 6+. Only if the prior phases have been symptom-stable for at least four weeks.
Two rules override everything else. First, stop any set two reps before failure. Training to failure spikes post-exertional symptoms out of proportion to the benefit. Second, never add load and volume in the same week. If you increase weight on squats, don’t also add a set. Pick one variable to change, let the body adapt for two weeks, then change the next.
Tai Chi, Yoga, and Qigong
The strongest single trial of non-aerobic movement for fibromyalgia was Wang and colleagues’ 2010 randomized controlled trial in the New England Journal of Medicine (DOI 10.1056/NEJMoa0912611). Sixty-six patients were randomized to twice-weekly Yang-style tai chi for 12 weeks versus a wellness-and-stretching control. The tai chi group improved significantly on the Fibromyalgia Impact Questionnaire, sleep, and depression scores, with benefits sustained at 24 weeks. A 2018 follow-up trial by the same group (BMJ 2018, DOI 10.1136/bmj.k851) replicated the finding and showed tai chi was at least as effective as aerobic exercise.
Tai chi works for fibromyalgia because it combines several active ingredients that are individually helpful and synergistic:
- Low-intensity continuous movement (aerobic exposure below any flare threshold).
- Weight-shifting balance training (proprioceptive recalibration for a sensitized nervous system).
- Diaphragmatic breathing (parasympathetic activation, vagal tone improvement).
- Meditative attention (reduces catastrophizing, a known amplifier of central pain).
- Social and teacher-led structure (improves adherence, a bigger driver of benefit than the movement itself in many trials).
Yoga — particularly gentle, restorative, or Iyengar styles with heavy prop use — has a smaller but positive evidence base. Avoid hot yoga (the heat plus the intensity push many fibromyalgia patients into crash territory). Avoid vinyasa-style flows if your sleep is already non-restorative. Qigong is essentially tai chi stripped of the martial forms and focused on breath-led movement; the trial data is smaller but directionally similar.
Distinguishing Post-Exertional Malaise from Normal Soreness
This is the most important diagnostic skill a person with fibromyalgia can develop. The two phenomena look similar at first — both involve “feeling bad after exercise” — but they respond to opposite strategies.
Normal post-exercise soreness (DOMS):
- Localized to the muscles you worked.
- Peaks 24–48 hours after the session and resolves by 72 hours.
- Feels mechanical — tender-to-press, sore on stretch, better with gentle movement.
- Mental clarity, sleep, and appetite are unchanged.
- Prescription: keep training, stay hydrated, maybe a lighter session.
Post-exertional malaise (PEM):
- Whole-system crash — muscle, joint, cognitive fog, orthostatic intolerance, sleep disruption, sometimes sore throat or swollen lymph nodes.
- Typically delayed 12–48 hours, lasts 2–7 days or longer.
- Disproportionate to the trigger (“I only walked to the mailbox”).
- Rest does not quickly resolve it the way it resolves soreness.
- Prescription: retreat from the activity level that triggered it, pace more conservatively for weeks, do not progress until fully stable.
If you consistently get PEM after sessions your protocol considers “gentle,” you likely have an ME/CFS-dominant phenotype. Classical GET is contraindicated. Pure pacing without progression — plus treating any co-occurring orthostatic intolerance, dysautonomia, or sleep disorder — is the correct first step. See the ME/CFS overlap article.
Using a Wearable to Track Load
Consumer wearables have quietly become one of the most useful tools in fibromyalgia self-management. The key metrics:
- Heart-rate variability (HRV). A morning HRV reading that is 10–20% below your personal baseline is the single best objective signal that you are under-recovered. Train lighter that day or rest. The Garmin “Body Battery,” Oura Ring “Readiness Score,” Apple Watch “HRV,” and Whoop “Recovery” all derive from the same underlying autonomic signal.
- Resting heart rate trend. A resting HR 7–10 bpm above your personal baseline for two days in a row is a reliable flare-warning signal. Pull back.
- Sleep staging. Consumer estimates of deep and REM sleep are approximate, but trends over weeks are useful. Non-restorative sleep is a fibromyalgia hallmark — see the sleep article.
- Daily step count. A ceiling, not a floor. For many fibromyalgia patients, a sustainable daily range is 4,000–7,500 steps. Chasing 10,000 is a boom-bust trap.
Which device matters less than using it consistently for at least six weeks to establish your personal baselines. The absolute number on any given day is nearly useless — the deviation from your baseline is what you act on.
Practical Weekly Templates
Two example weeks for different starting points. Adjust durations downward freely if these still feel too much.
Template A — Mild-to-moderate fibromyalgia, can tolerate a 15-minute walk without next-day flare:
- Monday: 20 minutes walking, heart-rate capped. Five minutes of gentle stretching.
- Tuesday: Phase-appropriate resistance circuit, 20–25 minutes total including rests.
- Wednesday: Rest or 15 minutes of tai chi / restorative yoga.
- Thursday: 20–25 minutes warm-water walking or aquatic class.
- Friday: Resistance circuit repeat.
- Saturday: 25-minute walk OR tai chi class. Not both.
- Sunday: Full rest. Gentle stretching only.
Template B — Severe fibromyalgia or PEM-dominant phenotype:
- Monday: 5 minutes seated leg raises + ankle circles. 5 minutes diaphragmatic breathing.
- Tuesday: Rest.
- Wednesday: 10 minutes warm-water walking in chest-deep pool, slow pace, no arm work.
- Thursday: Rest.
- Friday: 5–7 minutes supine mobility work — hip bridges, knee-to-chest, cat-cow on hands and knees if tolerated.
- Saturday: Rest.
- Sunday: 10 minutes tai chi video, seated modifications.
Hold Template B for at least four weeks before considering any increase. Progress only when morning symptom ratings are stable or rising for 14 consecutive days.
Common Pitfalls
- Progressing by feel on good days. A good day is not a reason to jump two phases. Stick to the plan you made on an average day.
- Skipping rest weeks. Every four to six weeks, hold volume and intensity flat for seven days. Not an absolute rest — just no progression. This consolidates adaptation.
- Treating stretching as exercise. Stretching feels good, but passive stretching alone has not shown meaningful benefit in fibromyalgia trials. It is an adjunct, not a substitute for aerobic + resistance + mind-body work.
- Chasing morning workouts when sleep is broken. If your sleep is non-restorative, training in the first two hours after waking is often the worst window. Mid-morning or early afternoon tends to work better.
- Ignoring stress load. A hard week at work, a family conflict, or grief all draw from the same envelope as physical activity. Pull back the training plan during life stress — see the stress management article.
Key Research Papers
- Busch AJ, et al. Exercise therapy for fibromyalgia. Cochrane Database of Systematic Reviews. 2013.
- Wang C, et al. A randomized trial of tai chi for fibromyalgia. N Engl J Med. 2010;363:743–754.
- Bidonde J, et al. Aquatic exercise training for fibromyalgia. Cochrane Database of Systematic Reviews. 2014/2017.
- Wang C, et al. Effect of tai chi versus aerobic exercise for fibromyalgia: comparative effectiveness randomized controlled trial. BMJ. 2018;360:k851.
- Bidonde J, et al. Aerobic exercise training for adults with fibromyalgia. Cochrane Database of Systematic Reviews. 2017.
Live PubMed Searches
For further reading, the following PubMed topic searches return current peer-reviewed work on exercise, pacing, and movement therapies in fibromyalgia:
- Fibromyalgia and graded exercise therapy
- Fibromyalgia pacing and the energy envelope
- Fibromyalgia and aquatic exercise
- Fibromyalgia and resistance training
- Fibromyalgia and tai chi
- Fibromyalgia and yoga
- Post-exertional malaise in fibromyalgia
- Heart-rate variability in fibromyalgia
- The PACE trial and ME/CFS graded exercise controversy
Connections
- Fibromyalgia and ME/CFS Overlap
- Central Sensitization Explained
- Stress Management
- Sleep and Non-Restorative Sleep
- Fibromyalgia Overview
- Arthritis
- Low-Dose Naltrexone for Fibromyalgia
- Nutrient Gaps in Fibromyalgia
- ACR 2016 Diagnostic Criteria
- Small-Fiber Neuropathy Overlap
- POTS Compression and Exercise Program
- Chronic Pain
- Chronic Fatigue Syndrome
- Ankylosing Spondylitis
- POTS
- MCAS
- Low-Dose Naltrexone
- Exercise and PT Protocol