Nutrient Gaps: Magnesium, Vitamin D, B12, Iron in Fibromyalgia
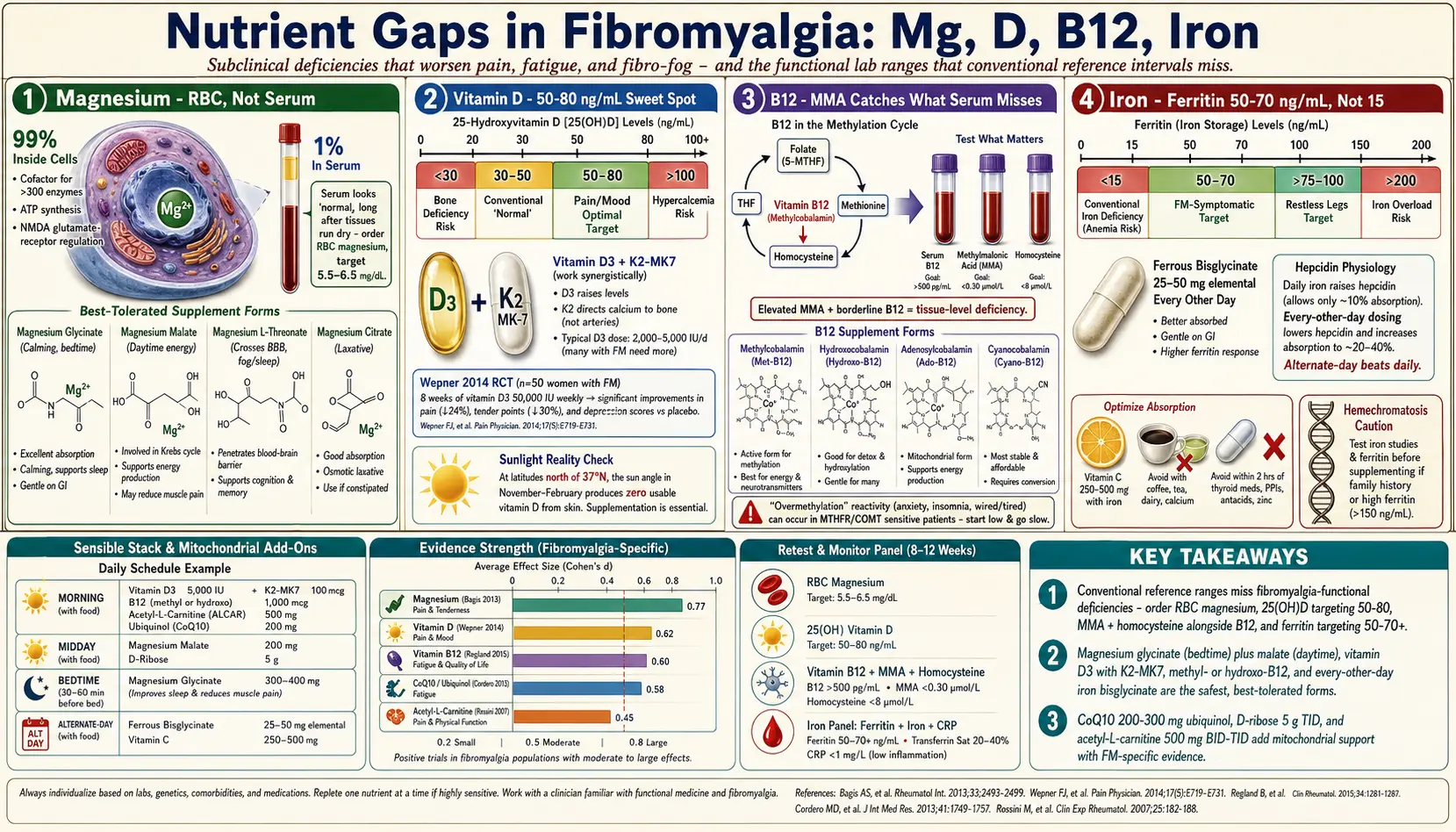
Table of Contents
- Why Nutrients Matter in Fibromyalgia
- Magnesium — The Most Commonly Missed Mineral
- Vitamin D — Pain, Mood, and the 50–80 Target
- Vitamin B12 — Why Serum Alone Misses Deficiency
- Iron and Ferritin — The >50–70 Sweet Spot
- CoQ10, Ribose, and Acetyl-L-Carnitine
- How to Stack a Sensible Protocol
- When to Be Extra Careful
- Key Research Papers
- Connections
- Featured Videos
Why Nutrients Matter in Fibromyalgia
If you have fibromyalgia, you have probably been told that "all your labs are normal." That phrase hides a lot. Standard lab panels catch frank deficiencies — anemia so severe your red cells are small and pale, vitamin D so low you are approaching osteomalacia, B12 so low your tongue is sore. They do not catch the subclinical gaps that quietly worsen fatigue, pain, and fibro fog in people whose cellular chemistry is already struggling.
Four nutrients come up over and over in careful fibromyalgia workups: magnesium, vitamin D, vitamin B12, and iron. None of them is a cure. But if any one of them is low, your symptoms will be worse than they need to be, and no medication or exercise plan will fully compensate. Fixing the gaps is the cheapest, lowest-risk step in the whole treatment stack, and it is often the step that gets skipped because a green checkmark appeared next to a reference range that was never designed with chronic-pain patients in mind.
This article walks through each nutrient: why it matters, which lab actually answers the question, which foods help, which supplement forms are worth buying, and what doses look like in practice. It also covers three "energy-metabolism" add-ons — CoQ10, D-ribose, and acetyl-L-carnitine — where the evidence is smaller but interesting enough to consider.
Magnesium — The Most Commonly Missed Mineral
Why it matters. Magnesium is a cofactor for more than 300 enzymes, including every step that makes ATP (cellular energy), every reaction that moves calcium out of muscle cells after contraction, and the NMDA glutamate receptor, which sits at the center of central sensitization. Low magnesium leaves NMDA receptors "unplugged" and more excitable — exactly the state fibromyalgia patients are trying to calm down. It also drives up muscle tone, promotes tension headaches, worsens sleep, and amplifies anxiety.
Bagis and colleagues (2013) randomized fibromyalgia women to magnesium citrate, amitriptyline, or both. All three arms improved pain and tender-point counts, and the combination beat either alone — with magnesium alone providing meaningful relief without medication side effects.
The lab trap. Serum magnesium is unreliable. Only about 1% of your body's magnesium lives in the blood; the rest is locked inside cells and bone. The body guards serum magnesium tightly, pulling from bone if it has to, so serum looks "normal" long after tissues have run dry. If your doctor orders serum magnesium and it reads 2.0 mg/dL, that tells you almost nothing.
Ask for RBC magnesium (red blood cell magnesium). It measures what is actually inside a cell and tracks tissue status far better. Target the upper half of the reference range, roughly 5.5–6.5 mg/dL. If RBC magnesium is unavailable, a 24-hour urinary magnesium or a magnesium-loading test is a distant second. Serum is a last resort — and even then, readings in the lower third of the range should be treated as presumptively insufficient.
Food sources. Pumpkin seeds, almonds, cashews, spinach, Swiss chard, black beans, edamame, dark chocolate (70%+), avocado, and mackerel. A handful of pumpkin seeds is roughly 150 mg; a cup of cooked spinach is about 160 mg. Most American diets deliver 200–250 mg per day; the RDA is 310–420 mg, and many fibro patients feel best closer to 500–600 mg total intake (food plus supplement).
Supplement forms — this matters a lot.
- Magnesium glycinate (bisglycinate). Bound to the amino acid glycine. Best all-around form: highly absorbed, calming (glycine itself is a mild inhibitory neurotransmitter), gentle on the gut. First choice for most fibromyalgia patients. Typical dose: 200–400 mg elemental magnesium at bedtime.
- Magnesium malate. Bound to malic acid, a Krebs-cycle intermediate. Preferred by many fibro patients for daytime energy and muscle pain. Dose: 200–400 mg elemental, often split morning and midday.
- Magnesium L-threonate. The only form that crosses the blood-brain barrier well. Small trials suggest cognitive and sleep benefit. Expensive. Reasonable if fibro fog and brain-based symptoms dominate. Dose: 1,500–2,000 mg of the threonate compound (about 140–200 mg elemental) at night.
- Magnesium citrate. Well-absorbed, cheap, but laxative at higher doses. Useful if constipation is also a problem.
- Magnesium oxide. The form in most drugstore multivitamins. Poorly absorbed (roughly 4%) and mostly acts as a laxative. Avoid if your goal is tissue repletion.
- Topical magnesium chloride (Epsom salt baths, magnesium oil). Absorption is modest but real, and a warm Epsom bath is genuinely helpful for flares even if the mineral uptake is small.
Dosing and cautions. Start at 200 mg elemental at bedtime and build up. If stools loosen, back off or switch from citrate to glycinate/malate. The upper tolerable limit from supplements is 350 mg/day per the U.S. Institute of Medicine — but that limit is based on laxative effect, not toxicity, and well-tolerated doses of 400–600 mg are routine in fibromyalgia practice. Do not exceed 250 mg/day without medical supervision if you have chronic kidney disease (eGFR <45), because failing kidneys cannot clear magnesium and toxicity becomes possible. Interactions: magnesium reduces absorption of some antibiotics (fluoroquinolones, tetracyclines) and thyroid medication — separate doses by 4 hours.
Vitamin D — Pain, Mood, and the 50–80 Target
Why it matters. Vitamin D is not really a vitamin; it is a steroid hormone with receptors on nearly every immune cell, muscle cell, and many pain-processing neurons. Low vitamin D is associated with diffuse musculoskeletal pain, low mood, poor sleep, and cytokine shifts that overlap with the fibromyalgia profile. Wepner and colleagues (2014) published a double-blind randomized trial of vitamin D supplementation in fibromyalgia patients with baseline 25(OH)D below 32 ng/mL; the treatment arm (titrated to 32–48 ng/mL) showed significantly reduced pain on a visual analog scale compared with placebo.
The lab. Ask for 25-hydroxyvitamin D [25(OH)D], not 1,25-dihydroxyvitamin D. 25(OH)D is the storage form and reflects your total supply; 1,25-D is an active hormone tightly controlled by the kidney and tells you little about status.
Conventional labs flag deficiency only below 20 or 30 ng/mL. That is a bone-health threshold. For pain and mood, most integrative clinicians target 50–80 ng/mL (125–200 nmol/L). Many fibromyalgia patients feel best near the middle of that range. Staying under 100 ng/mL keeps you comfortably away from hypercalcemia risk.
Food and sunlight. Food alone rarely gets you there. Wild salmon, sardines, mackerel, egg yolks, and cod liver oil are the usable sources; fortified milk and cereals provide trivial amounts. Sunlight on bare skin (arms and legs, midday, no sunscreen, 10–20 minutes for fair skin, longer for darker skin) drives endogenous production from April to October in the continental U.S. Latitude above roughly 37°N (San Francisco, Richmond, Denver) produces no usable vitamin D from November through February regardless of how sunny the sky looks.
Supplement form. Vitamin D3 (cholecalciferol), not D2 (ergocalciferol). D3 raises 25(OH)D more reliably. Pair with vitamin K2 (MK-7, 90–180 mcg/day): K2 directs calcium to bones and teeth and away from arteries and soft tissue, an important partner when D is pushed above 50 ng/mL. Take both with fat (a meal with oil, butter, or avocado) — they are fat-soluble and absorption collapses on an empty stomach.
Dosing. A practical ramp for an adult with baseline 25(OH)D of 20–30 ng/mL: 5,000 IU of D3 plus 100 mcg K2-MK7 daily with the largest meal, retest at 8–12 weeks, then adjust. If baseline is under 20 ng/mL, some clinicians load with 10,000 IU/day for 8 weeks before dropping to maintenance. Once you hit the 50–80 range, maintenance is usually 2,000–5,000 IU/day depending on body size, latitude, skin color, and sun habits.
Cautions. Hypercalcemia is the real risk at sustained high doses. Recheck 25(OH)D and a serum calcium (or ionized calcium) after dose changes. Be cautious and consult a physician before high-dose D if you have sarcoidosis, granulomatous disease, lymphoma, primary hyperparathyroidism, or a history of kidney stones — these conditions can convert 25-D to active 1,25-D unchecked. Thiazide diuretics also raise calcium retention; coordinate with your prescriber.
Vitamin B12 — Why Serum Alone Misses Deficiency
Why it matters. B12 is essential for myelin repair, red-cell production, and the methylation reactions that recycle homocysteine and keep neurotransmitters (serotonin, dopamine, norepinephrine) flowing. Regland and colleagues have repeatedly documented elevated cerebrospinal-fluid homocysteine in fibromyalgia and ME/CFS patients — a functional signature of B12 and folate undersupply even when serum B12 looks normal. In a 2015 open-label study, Regland's team treated fibromyalgia/CFS patients with weekly hydroxocobalamin injections plus oral folic acid; response correlated with how aggressively the protocol was pushed.
The lab trap. Serum B12 is a poor screen. The U.S. reference range (typically 200–900 pg/mL) was set against frank megaloblastic anemia, not neurological or fatigue symptoms. Japan and most European countries flag anything under 500 pg/mL as deficient, and functional medicine clinicians often target >550–600 pg/mL. Worse, serum B12 can look high while tissue B12 is low — circulating analog B12, liver disease, and certain supplements can all inflate the number.
To catch functional deficiency, add methylmalonic acid (MMA) and homocysteine. MMA accumulates when B12 is truly low in the cell. Homocysteine rises when either B12 or folate is insufficient. An elevated MMA with a borderline-low B12 means tissue-level deficiency regardless of what the serum says — and it is common in fibromyalgia.
Food sources. B12 is found only in animal foods: clams, liver, sardines, salmon, beef, eggs, dairy. Vegans must supplement; long-term vegans without supplementation almost always develop deficiency eventually. Older adults lose stomach acid and intrinsic factor with age, so absorption drops even on a meat-heavy diet — the NIH estimates up to 20% of adults over 60 have some degree of B12 malabsorption. Long-term use of proton-pump inhibitors (omeprazole, esomeprazole), H2 blockers, and metformin also depletes B12 and warrants monitoring.
Supplement forms.
- Methylcobalamin (methyl-B12). The active coenzyme form. Absorbed well sublingually. Preferred by many clinicians, especially for neurological symptoms.
- Hydroxocobalamin. The form used in European and some U.S. clinical practice. Long-lasting in tissue; easier on sensitive people who react poorly to methylated B-vitamins. Often given as an intramuscular injection (1 mg weekly or monthly).
- Adenosylcobalamin. The mitochondrial form; sometimes paired with methyl-B12 for energy-forward protocols.
- Cyanocobalamin. The cheapest form and the one in most multivitamins. Your body must strip the cyanide group and convert it. Works fine for most people but is a poor choice for anyone with MTHFR, COMT, or detox concerns.
The methylation caveat. A subset of patients — often carriers of COMT or MTHFR variants — feel anxious, wired, or irritable on high-dose methyl-B12 or methyl-folate. This is sometimes called "overmethylation." If that happens, switch to hydroxocobalamin, start much lower (250–500 mcg rather than 1,000–5,000), and add a small amount of folate as folinic acid rather than L-methylfolate. This is not a reason to avoid B12 — it is a reason to match the form to your biochemistry.
Dosing. For oral repletion in fibromyalgia with borderline labs: 1,000–5,000 mcg methyl-B12 or hydroxo-B12 sublingually daily for 8–12 weeks, retest MMA and homocysteine, then taper to a maintenance dose (500–1,000 mcg daily or several times per week). If MMA stays elevated on oral therapy, intramuscular hydroxocobalamin (1 mg weekly for 8 weeks, then monthly) is more reliable.
Iron and Ferritin — The >50–70 Sweet Spot
Why it matters. Iron is the core of hemoglobin (oxygen transport), myoglobin (oxygen storage in muscle), and several enzymes that make dopamine and serotonin. Low iron — even without anemia — causes fatigue, restless legs, cold extremities, brain fog, thinning hair, and exercise intolerance. Women of reproductive age, heavy menstruators, frequent blood donors, and anyone with gut bleeding or celiac disease are at high risk, and fibromyalgia patients cluster in those categories.
The lab trap. Hemoglobin can still be "normal" long after iron stores are exhausted. The key test is ferritin, which measures stored iron. The U.S. reference range runs from roughly 15 to 200 ng/mL, and most labs flag "normal" above 15. That is a starvation threshold.
For fibromyalgia symptoms, most functional and sleep-medicine clinicians target ferritin above 50–70 ng/mL; for restless legs, the neurological target is often >75–100 ng/mL. Patients at 20 ng/mL are technically "normal" but functionally iron-depleted and often exhausted.
Order a full iron panel: ferritin, serum iron, TIBC (total iron binding capacity), transferrin saturation, and CRP. Ferritin rises with inflammation, so a "normal" ferritin in someone with an elevated CRP can mask real deficiency — the transferrin saturation (should be >20%) helps sort this out.
Food sources. Heme iron (red meat, liver, shellfish, sardines) absorbs roughly 15–35%. Non-heme iron (lentils, beans, spinach, pumpkin seeds, dark chocolate) absorbs only 2–20% and drops further in the presence of tea, coffee, calcium, or whole grains. Pairing non-heme sources with vitamin C (peppers, citrus, kiwi) two- to three-folds absorption.
Supplement forms.
- Ferrous bisglycinate (iron chelate). Best-tolerated form. Gentle on the gut, minimal constipation, good absorption. First choice. Typical dose: 25–50 mg elemental iron every other day.
- Ferrous sulfate. Cheap and effective but notorious for nausea, constipation, and black stools. Works, but many patients abandon it.
- Ferrous fumarate and ferrous gluconate. Middle-ground tolerability.
- Heme iron polypeptide. Derived from animal hemoglobin; highly absorbed, expensive.
- IV iron (iron sucrose, ferric carboxymaltose). For patients who cannot tolerate oral iron, have malabsorption, or need rapid repletion. Requires a prescriber and infusion setup.
Dosing. Current evidence favors every-other-day dosing of 50–100 mg elemental iron rather than daily. A dose of iron temporarily spikes a hormone called hepcidin that blocks the next day's absorption, so daily dosing is less efficient than alternate-day. Take with vitamin C, on an empty stomach if tolerated, away from coffee, tea, dairy, calcium supplements, and thyroid medication. Recheck ferritin at 8–12 weeks.
Cautions. Do not supplement iron without a lab showing you need it. Iron overload (hemochromatosis) is common — roughly 1 in 200 people of Northern European descent carry two HFE mutations — and pushing iron into someone who already has plenty damages the liver, pancreas, and heart. Men and postmenopausal women in particular should confirm low ferritin before supplementing.
CoQ10, Ribose, and Acetyl-L-Carnitine
Beyond the big four, three mitochondrial-support nutrients have fibromyalgia-specific evidence worth knowing about.
Coenzyme Q10 (ubiquinone / ubiquinol). CoQ10 shuttles electrons through the mitochondrial electron transport chain. Cordero and colleagues have published a series of small randomized trials showing that fibromyalgia patients have lower CoQ10 levels in blood mononuclear cells and improve on supplementation. Typical dose: 200–300 mg/day of ubiquinol (the reduced, better-absorbed form) with a fatty meal. Especially worth considering if you also take a statin, which depletes CoQ10.
D-Ribose. A five-carbon sugar that is the backbone of ATP itself. Teitelbaum's open-label studies in fibromyalgia and ME/CFS reported roughly 30% reductions in fatigue and pain at 5 g three times daily. Evidence quality is modest (no large placebo-controlled trials), but the intervention is cheap and low-risk. Caveat: it is a sugar and can temporarily lower blood glucose — diabetics should monitor, and it should be taken with food if hypoglycemia is a concern.
Acetyl-L-Carnitine (ALCAR). Shuttles fatty acids into mitochondria for beta-oxidation. A 2007 randomized controlled trial by Rossini and colleagues in fibromyalgia patients (1,500 mg/day orally plus intramuscular injections) reported significant reduction in pain, tender-point count, and depression compared with placebo. Typical oral dose: 500 mg two to three times daily. Avoid taking late in the evening — some people find it stimulating.
How to Stack a Sensible Protocol
A reasonable starting protocol for a fibromyalgia patient with documented gaps might look like this:
- Morning, with breakfast: Vitamin D3 5,000 IU + K2-MK7 100 mcg, methyl- or hydroxo-B12 1,000 mcg sublingual, acetyl-L-carnitine 500 mg, CoQ10 (ubiquinol) 200 mg.
- Midday, with lunch: Magnesium malate 200 mg elemental, D-ribose 5 g (mixed into water or tea).
- Bedtime: Magnesium glycinate 300–400 mg elemental.
- Alternate days, away from coffee/dairy/thyroid meds: Ferrous bisglycinate 25–50 mg elemental + vitamin C 250–500 mg (only if ferritin is low).
Retest at 8–12 weeks: RBC magnesium, 25(OH)D, serum B12 plus MMA and homocysteine, ferritin plus iron panel plus CRP. Adjust doses based on results, not symptoms alone. Nutrient repletion is usually slow; expect real tissue-level changes over 3–6 months, not 3–6 days.
When to Be Extra Careful
- Chronic kidney disease. Magnesium, potassium, and high-dose D all require coordination with your nephrologist. Do not freelance.
- Hemochromatosis, HFE carriers, frequent transfusions. Do not supplement iron without a recent ferritin under 50 ng/mL.
- Sarcoidosis, granulomatous disease, lymphoma, primary hyperparathyroidism, history of kidney stones. High-dose vitamin D can provoke hypercalcemia.
- Pregnancy and breastfeeding. RDAs change. Coordinate with your obstetrician.
- Thyroid medication, fluoroquinolone or tetracycline antibiotics, bisphosphonates. Separate from magnesium, iron, and calcium by at least 4 hours.
- Proton-pump inhibitors, metformin, anticonvulsants. Long-term use depletes B12 and magnesium — test annually.
- Overmethylation reactivity. If methyl-B12 or L-methylfolate makes you anxious, jittery, or insomniac, switch to hydroxocobalamin and folinic acid at lower doses.
None of these cautions is a reason to skip nutrient work. They are reasons to test before treating, to start low, and to recheck after 8–12 weeks. Fibromyalgia is not cured by any single supplement, but patients who close these four gaps almost always feel the difference — fewer bad days, lighter fog, more usable energy, and a smaller gap between what they want to do and what their body will allow.
Key Research Papers
- Bagis S, et al. Is magnesium citrate treatment effective on pain, clinical parameters and functional status in patients with fibromyalgia? Rheumatol Int. 2013.
- Wepner F, et al. Effects of vitamin D on patients with fibromyalgia syndrome: a randomized placebo-controlled trial. Pain. 2014.
- Regland B, et al. Response to vitamin B12 and folic acid in myalgic encephalomyelitis and fibromyalgia. PLoS ONE. 2015.
- Cordero MD, et al. Coenzyme Q10 in fibromyalgia: oxidative stress and clinical improvement. Antioxid Redox Signal. 2013.
- Rossini M, et al. Acetyl-L-carnitine in fibromyalgic syndrome: a randomized, double-blind, placebo-controlled clinical trial. Clin Exp Rheumatol. 2007.
- Stoffel NU, et al. Iron absorption from oral iron supplements given on consecutive versus alternate days. Lancet Haematol. 2017 (alternate-day iron dosing).
Live PubMed Searches
For further reading, the following PubMed topic searches return current peer-reviewed work on nutrient status in fibromyalgia and related chronic-pain syndromes:
- Fibromyalgia and magnesium
- Fibromyalgia, vitamin D, and pain
- Fibromyalgia, B12, and homocysteine
- Fibromyalgia, ferritin, and iron status
- Fibromyalgia and coenzyme Q10
- Fibromyalgia and acetyl-L-carnitine
- Fibromyalgia, D-ribose, and chronic fatigue
- RBC magnesium and tissue status assessment
- Methylmalonic acid and functional B12 deficiency
- Alternate-day iron dosing and hepcidin
Connections
- Magnesium
- Fibromyalgia Overview
- Iron
- Vitamin B12
- Vitamin D3
- Fibromyalgia and ME/CFS Overlap
- Low-Dose Naltrexone for Fibromyalgia
- Sleep and Non-Restorative Sleep
- ACR 2016 Diagnostic Criteria
- Central Sensitization Explained
- Small-Fiber Neuropathy Overlap
- Exercise Pacing and Graded Movement
- Chronic Fatigue Syndrome
- Homocysteine
- Calcium
- Vitamin B12 Test
- Fatigue
- Magnesium Glycinate