ACR 2016 Diagnostic Criteria for Fibromyalgia
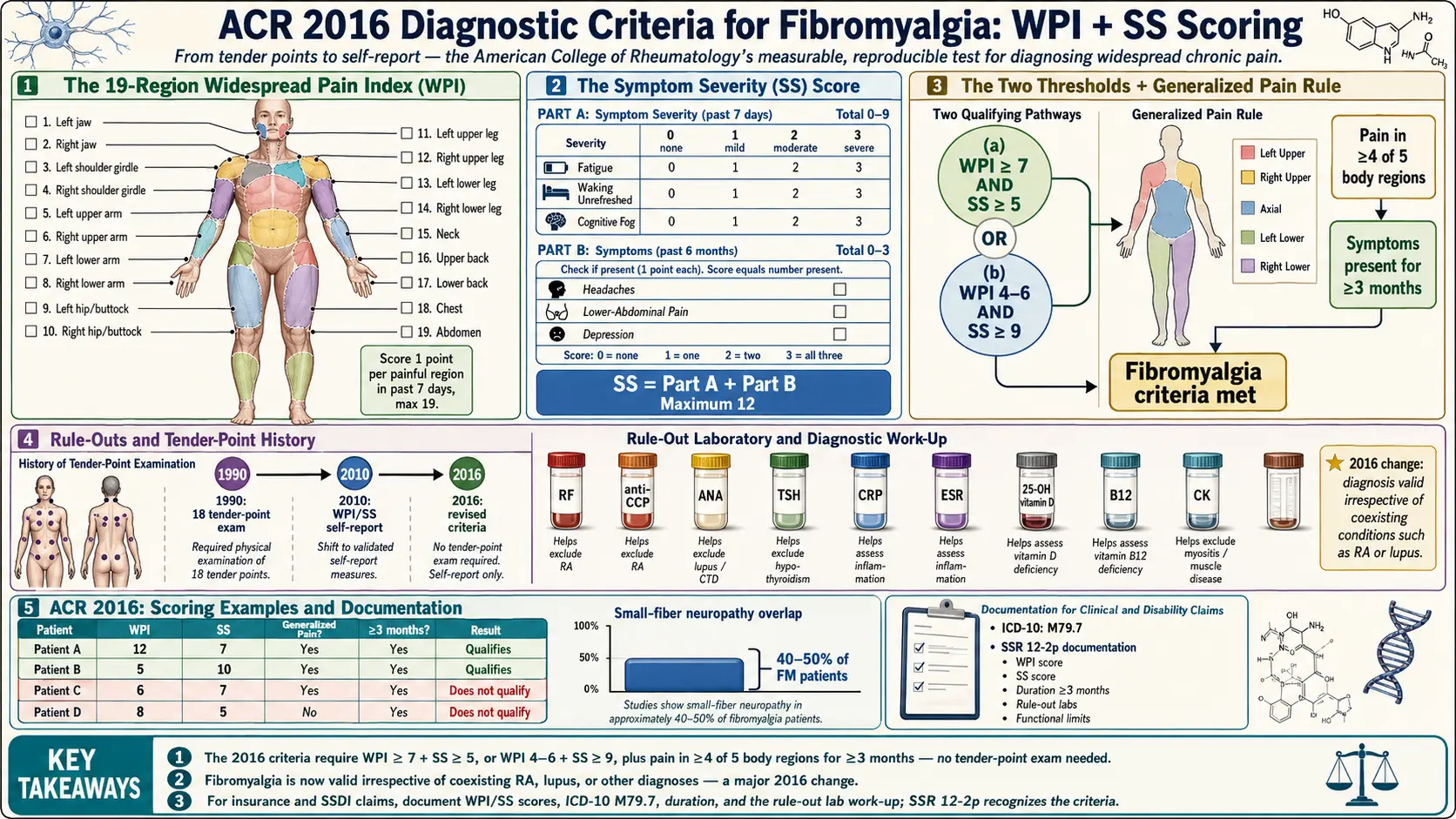
Table of Contents
- Why Diagnostic Criteria Matter
- A Short History: From Tender Points to Self-Report
- The Widespread Pain Index (WPI) — 19 Body Regions
- The Symptom Severity (SS) Score
- The Two Thresholds: How You Qualify
- The "Generalized Pain" Rule — 4 of 5 Regions
- Duration: Why It Must Be at Least 3 Months
- Rule-Outs: What Else Could It Be?
- How to Use a Self-Score Sheet Before Your Appointment
- Why the Criteria Still Miss Some Patients
- Insurance and Disability Documentation Tips
- Key Research Papers
- Connections
- Featured Videos
Why Diagnostic Criteria Matter
If you have spent years bouncing between doctors who tell you your labs are normal, your scans are clean, and maybe you should see a psychiatrist, then a formal diagnosis of fibromyalgia is not just a label. It is a passport. It gets you access to medications that are actually indicated (pregabalin, duloxetine, milnacipran, low-dose naltrexone off-label), to physical therapy approved for central pain, to disability accommodations when you need them, and — just as importantly — to the end of being told your pain is imaginary.
The American College of Rheumatology (ACR) 2016 diagnostic criteria are the tool most rheumatologists, pain specialists, and primary care physicians in the U.S. now use to make that call. They are not perfect. They still miss people with unusual presentations, and they do not replace clinical judgment. But they are measurable, reproducible, and based on how fibromyalgia actually feels from the inside — which is a huge step forward from the hands-on ritual of poking eighteen spots on your body that dominated the field for a quarter century.
This article walks through the 2016 criteria the way you would actually use them: what the history is, what the two scores mean, how to fill out the sheet yourself, where the criteria fall short, and how to turn a positive result into documentation that works with insurance and disability.
A Short History: From Tender Points to Self-Report
1990 — the tender-point era. The original ACR criteria, published by Wolfe and colleagues, required two things: widespread pain for at least three months, and tenderness on digital palpation at at least 11 of 18 specific anatomic points (occiput, low cervical, trapezius, supraspinatus, second rib, lateral epicondyle, gluteal, greater trochanter, and medial knee, each side). The examiner pressed with about 4 kg of force — roughly the pressure that blanches a fingernail. This worked as a research tool but was a disaster in the clinic. Most primary care doctors never learned the exam, pressed too hard or too soft, and by the 2000s the average rheumatologist had quietly stopped counting tender points.
2010 — the first redesign. Wolfe's group threw out tender points and introduced two numeric scores: the Widespread Pain Index (WPI), which counts painful body regions, and the Symptom Severity (SS) Score, which rates fatigue, unrefreshing sleep, cognitive problems, and a long somatic symptom checklist. A patient met criteria if WPI was at least 7 and SS at least 5, or if WPI was 3–6 and SS at least 9. The criteria still required a physician's interview.
2011 — the self-report modification. Researchers realized patients could answer the questions themselves on paper, with results that matched physician interviews closely. This made the tool usable in surveys and epidemiology — and made it possible for you, the patient, to fill out a draft before your appointment and hand it to the doctor.
2016 — the current revision. Wolfe and colleagues tightened the 2010/2011 criteria to reduce misclassification. Three changes mattered most:
- A new "generalized pain" requirement: pain in at least 4 of 5 body regions (not just any 7 of 19 spots), so that people with only regional pain (e.g., just the neck and shoulders) no longer qualify.
- The somatic symptom checklist was simplified to a count of three specific symptoms (headaches, lower abdominal pain or cramps, depression) instead of the long open-ended list.
- The criteria explicitly say a fibromyalgia diagnosis is valid irrespective of other diagnoses — a major change. Before 2016, rheumatologists often refused to diagnose fibromyalgia if the patient also had rheumatoid arthritis or lupus, on the theory that the "real" disease explained everything. The 2016 revision acknowledges what patients have known for years: you can have both, and fibromyalgia on top of another inflammatory disease needs its own treatment.
The Widespread Pain Index (WPI) — 19 Body Regions
The WPI is just a count. You check off every region where you have had pain in the past week. Each region scores 1 point if painful, 0 if not. The maximum score is 19.
The 19 regions are:
- Upper body, left side: shoulder girdle, upper arm, lower arm, jaw
- Upper body, right side: shoulder girdle, upper arm, lower arm, jaw
- Lower body, left side: hip (buttock, trochanter), upper leg, lower leg
- Lower body, right side: hip (buttock, trochanter), upper leg, lower leg
- Axial: neck, upper back, lower back, chest, abdomen
Count each jaw separately (left and right). Count each hip separately. "Pain" means any pain, ache, soreness, tenderness, or burning — not just sharp pain. If the region hurt at any point in the past seven days, mark it.
The Symptom Severity (SS) Score
The SS score has two parts. The total is 0–12.
Part A — three core symptoms, each scored 0 to 3 for the past week:
- Fatigue — 0 = no problem, 1 = slight or mild, 2 = moderate, 3 = severe, pervasive, continuous, life-disturbing.
- Waking unrefreshed — same 0 to 3 scale. You sleep eight hours and wake up feeling as if you did not sleep at all.
- Cognitive symptoms ("fibro fog") — trouble thinking, remembering words, concentrating. Same 0 to 3 scale.
Part A ranges from 0 to 9.
Part B — three somatic symptoms, scored as a simple presence count (0 = none, 1 = any one, 2 = any two, 3 = all three) in the past six months:
- Headaches
- Pain or cramps in the lower abdomen
- Depression
Part B ranges from 0 to 3.
Total SS = Part A + Part B, maximum 12. Write both subtotals down separately — some older intake forms still list the 2010 version, which used a longer symptom list. If your doctor hands you the longer form, that is fine, but confirm they are scoring it by 2016 rules.
The Two Thresholds: How You Qualify
A patient satisfies the 2016 criteria when all three of the following are true:
- Either WPI ≥ 7 AND SS ≥ 5, or WPI between 4 and 6 AND SS ≥ 9.
- Generalized pain: pain in at least 4 of the 5 body regions (see next section).
- Symptoms present at similar level for at least 3 months.
That is the whole test. Two numbers, a geographic check, and a duration. No lab test, no imaging, no tender-point exam.
Examples:
- WPI 9, SS 6 — qualifies (first threshold).
- WPI 5, SS 10 — qualifies (second threshold).
- WPI 6, SS 7 — does not qualify. You need SS 9 or higher at this WPI range.
- WPI 12, SS 4 — does not qualify. You need SS at least 5.
Patients who fall just below the cutoffs on one visit frequently qualify on another — fibromyalgia fluctuates. If you are close, it is worth rescoring in a few weeks.
The "Generalized Pain" Rule — 4 of 5 Regions
The 2016 revision added a geographic filter. The 19 WPI spots collapse into 5 large regions:
- Left upper region — left jaw, left shoulder girdle, left upper arm, left lower arm
- Right upper region — right jaw, right shoulder girdle, right upper arm, right lower arm
- Left lower region — left hip/buttock, left upper leg, left lower leg
- Right lower region — right hip/buttock, right upper leg, right lower leg
- Axial region — neck, upper back, lower back, chest, abdomen
You must have pain in at least four of these five regions. This rule excludes people whose pain is truly localized — for example, chronic low-back and neck pain only (one region: axial), or bilateral knee pain only (two regions: left lower, right lower). Those patients may have real chronic pain, but the 2016 criteria reserve the fibromyalgia label for pain that is distributed across the whole body.
Duration: Why It Must Be at Least 3 Months
Pain and fatigue lasting less than three months are often explained by an active infection, a medication side effect, an injury, a depressive episode, or a flare of an underlying inflammatory disease that will eventually declare itself. Three months is long enough to filter out most of those confounders while still being short enough that patients do not have to wait years to be diagnosed.
"Similar level for three months" does not mean your pain score is identical every day. Fibromyalgia flares. What the criteria ask is that the overall symptom picture — WPI roughly in range, SS roughly in range — has been present continuously, not just for a single bad week.
Rule-Outs: What Else Could It Be?
Although the 2016 criteria allow fibromyalgia to coexist with other diagnoses, a responsible clinician still rules out conditions that mimic it, because some of those require specific treatment. Standard first-pass labs and assessments:
- Rheumatoid arthritis (RA) — RF, anti-CCP antibodies, CRP, ESR. RA typically causes swollen joints with morning stiffness more than an hour; fibromyalgia causes pain without visible swelling.
- Systemic lupus erythematosus (SLE) — ANA, complement (C3/C4), urinalysis. Lupus often brings rash, mouth ulcers, cytopenias, and kidney findings.
- Hypothyroidism — TSH, free T4. Untreated hypothyroidism can reproduce fatigue, muscle pain, cognitive fog, and cold intolerance almost perfectly. See thyroid disorders and Hashimoto's thyroiditis.
- Polymyalgia rheumatica (PMR) — onset typically after age 50, bilateral shoulder and hip girdle pain with dramatic morning stiffness, markedly elevated ESR and CRP, and a near-miraculous response to low-dose prednisone. Fibromyalgia does not respond to steroids.
- Vitamin D deficiency — 25-hydroxy vitamin D. Low D produces diffuse musculoskeletal pain that improves with replacement.
- Vitamin B12 deficiency — B12, methylmalonic acid. Causes fatigue, neuropathy, cognitive changes.
- Sleep apnea — a sleep study if snoring, witnessed apneas, or daytime sleepiness suggest it. Untreated apnea can masquerade as fibromyalgia.
- Myositis — CK (creatine kinase). Inflammatory muscle diseases cause weakness more than pain.
None of these rule-outs are sufficient on their own. A normal TSH does not prove fibromyalgia; it only removes hypothyroidism from the list. The 2016 criteria are the positive diagnostic step; lab work is the negative one.
How to Use a Self-Score Sheet Before Your Appointment
The single most effective thing you can do before a rheumatology or pain appointment is to arrive with a completed 2016 self-score sheet. Most doctors have one in the drawer, but many have never used it. Here is how to build and use your own:
- Draw a simple body diagram with the 19 WPI regions labeled. Over seven days, mark every region that hurts at any point during the week. Do it each evening so you do not forget.
- Record the SS scores each evening too. Rate fatigue, waking unrefreshed, and cognitive problems on the 0–3 scale for that day. Average the week.
- Check the three somatic symptoms (headaches, lower abdominal pain, depression) for the past six months. Each present symptom adds 1 to SS.
- Total both scores. Check which threshold you meet, confirm the 4-of-5 regions rule, and note duration.
- Bring it to the appointment on paper. This short-circuits the "can you describe your pain?" interview that often goes nowhere, and it signals to the doctor that you know the criteria and expect them to apply them.
If your clinician refuses to use the ACR 2016 criteria and insists on a tender-point exam that has been obsolete since 2010, that is a legitimate reason to seek a second opinion.
Why the Criteria Still Miss Some Patients
The 2016 criteria are the best tool available and still imperfect. Three groups of patients are frequently missed:
Patients with small-fiber neuropathy overlap. Up to 40–50% of people diagnosed with fibromyalgia have measurable loss of small nerve fibers on skin biopsy or corneal confocal microscopy. Their pain has a more burning, electric, stocking-and-glove distribution that may not light up all 4 of 5 regions the way classical fibromyalgia does. These patients may fail the 2016 criteria yet have the same underlying pain amplification. The overlap is discussed in detail in the small-fiber neuropathy overlap article.
Patients with severe fatigue and mild pain. Some people with what most specialists would call fibromyalgia have towering fatigue, cognitive fog, and unrefreshing sleep with relatively modest pain. They may score SS 9 or higher but WPI only 3, which is just below the second threshold. These patients often sit at the boundary with myalgic encephalomyelitis / chronic fatigue syndrome. See the fibromyalgia and ME/CFS overlap article.
Patients in a flare-and-remission pattern. If you happen to be in a relatively good week when you fill out the form, you may not qualify that week even though you clearly qualify most weeks. The criteria are a snapshot, not a long-term assessment. Keep a symptom diary over several months if this describes you, and present the full range to your doctor.
A diagnosis that is clinically obvious to an experienced physician sometimes fails the criteria on paper. The criteria do not override clinical judgment; they support it.
Insurance and Disability Documentation Tips
A diagnosis that sits in your chart only as "fibromyalgia, unspecified" will not carry much weight with a disability insurer. Documentation that holds up requires specifics. When your clinician writes the note, ask for these elements:
- The ICD-10 code. Fibromyalgia is M79.7. Make sure it appears on the problem list and on every relevant visit note.
- The actual WPI and SS scores, written out. "Patient meets ACR 2016 criteria with WPI 11 and SS 8" carries far more weight than "patient has widespread pain."
- Duration. "Symptoms present continuously for [N] months/years."
- The rule-out work-up. List the labs that came back normal (TSH, ANA, RF, anti-CCP, CRP, 25-OH vitamin D, B12, CK). This demonstrates the diagnosis is not a cop-out.
- Functional limitations. Specific, measurable: cannot stand more than 20 minutes, cannot lift more than 10 pounds, cannot concentrate for more than 30 minutes without a break. Avoid vague words like "struggles" or "fatigued."
- Treatment history. Medications tried, physical therapy attempted, response to each. Disability claims require evidence that conservative treatment has failed.
Social Security Disability (SSDI). The Social Security Administration issued SSR 12-2p in 2012, which formally recognizes fibromyalgia as a medically determinable impairment when documented by the 1990 ACR criteria or the 2010 criteria. The 2016 revision is generally accepted as the updated version of the 2010 criteria, though some adjudicators are still catching up. If your SSDI claim is denied on the grounds that fibromyalgia is not established, reference SSR 12-2p in the appeal.
Private long-term disability. Many policies contain a 24-month limit on "self-reported symptoms" that explicitly includes fibromyalgia. This is not illegal, and there is no workaround for the clause itself. What you can do is strengthen the record with objective findings where possible: skin biopsy for small-fiber neuropathy, sleep study results, neurocognitive testing, and functional capacity evaluations. Those shift the claim from "self-reported" to "supported by objective testing."
None of this is a substitute for a disability attorney in a contested claim. But bringing a clean ACR 2016 score sheet, a documented rule-out work-up, and specific functional limitations to the table makes every subsequent step easier.
Key Research Papers
- Wolfe F, Clauw DJ, Fitzcharles MA, et al. 2016 Revisions to the 2010/2011 fibromyalgia diagnostic criteria. Semin Arthritis Rheum. 2016;46(3):319–329.
- Wolfe F, Clauw DJ, Fitzcharles MA, et al. The American College of Rheumatology preliminary diagnostic criteria for fibromyalgia and measurement of symptom severity. Arthritis Care Res. 2010;62(5):600–610.
- Wolfe F, Smythe HA, Yunus MB, et al. The American College of Rheumatology 1990 criteria for the classification of fibromyalgia. Arthritis Rheum. 1990;33(2):160–172.
- Wolfe F, Clauw DJ, Fitzcharles MA, et al. Fibromyalgia criteria and severity scales for clinical and epidemiological studies: a modification of the ACR preliminary diagnostic criteria. J Rheumatol. 2011;38(6):1113–1122.
- Clauw DJ. Fibromyalgia: a clinical review. JAMA. 2014;311(15):1547–1555.
Live PubMed Searches
For further reading, the following PubMed topic searches return current peer-reviewed work on the ACR criteria and fibromyalgia diagnosis:
- ACR 2016 fibromyalgia diagnostic criteria
- Widespread Pain Index and Symptom Severity score
- Fibromyalgia tender point exam — historical perspective
- Fibromyalgia and small-fiber neuropathy
- Fibromyalgia self-report questionnaire validation
- Fibromyalgia vs polymyalgia rheumatica differential diagnosis
- Fibromyalgia and hypothyroidism overlap
- Fibromyalgia disability adjudication and SSR 12-2p
Connections
- Fibromyalgia Overview
- Fibromyalgia and ME/CFS Overlap
- Central Sensitization Explained
- Hashimoto's Thyroiditis
- Thyroid Disorders
- Small-Fiber Neuropathy Overlap
- Arthritis
- Chronic Pain
- Chronic Fatigue Syndrome
- Low-Dose Naltrexone for Fibromyalgia
- Sleep and Non-Restorative Sleep
- Nutrient Gaps in Fibromyalgia
- Exercise Pacing and Graded Movement
- Fatigue
- Depression
- Low-Dose Naltrexone
- MCAS
- POTS