Cannabis, CBD & Medical Marijuana for Fibromyalgia
If you have fibromyalgia, you have almost certainly wondered whether cannabis — CBD oil, medical marijuana, a THC gummy your cousin swears by — could actually help. The short answer is: probably, for some symptoms, in some people, at the right dose. The longer answer is what this article is for. We will walk through the endocannabinoid deficiency hypothesis that underlies the rationale, the real (and limited) evidence base, how THC and CBD differ, which ratios and forms make sense, how to dose without spending three days on the couch, and the drug interactions, legal issues, and long-term risks that rarely get mentioned in dispensary brochures.
Cannabis does not cure fibromyalgia. Nothing does. But used carefully, it can complement a treatment plan that already includes low-dose naltrexone, SNRIs such as duloxetine, serious sleep repair, and graded movement.
Table of Contents
- The Endocannabinoid Deficiency Hypothesis
- What the Evidence Actually Says
- THC vs CBD — Two Very Different Drugs
- Ratios: 1:1, High-CBD, and Microdosing
- Forms and Kinetics: Tinctures, Flower, Edibles
- Dosing Strategy: Low and Slow
- The Entourage Effect: Full-Spectrum vs Isolate
- Drug Interactions and Side Effects
- Legality, Driving, Work, and Pharmaceuticals
- CBD Purity and the Certificate of Analysis
- If You Are on Opioids, SSRIs, or Warfarin
- Key Research Papers
- PubMed Topic Searches
- Connections
- Featured Videos
The Endocannabinoid Deficiency Hypothesis
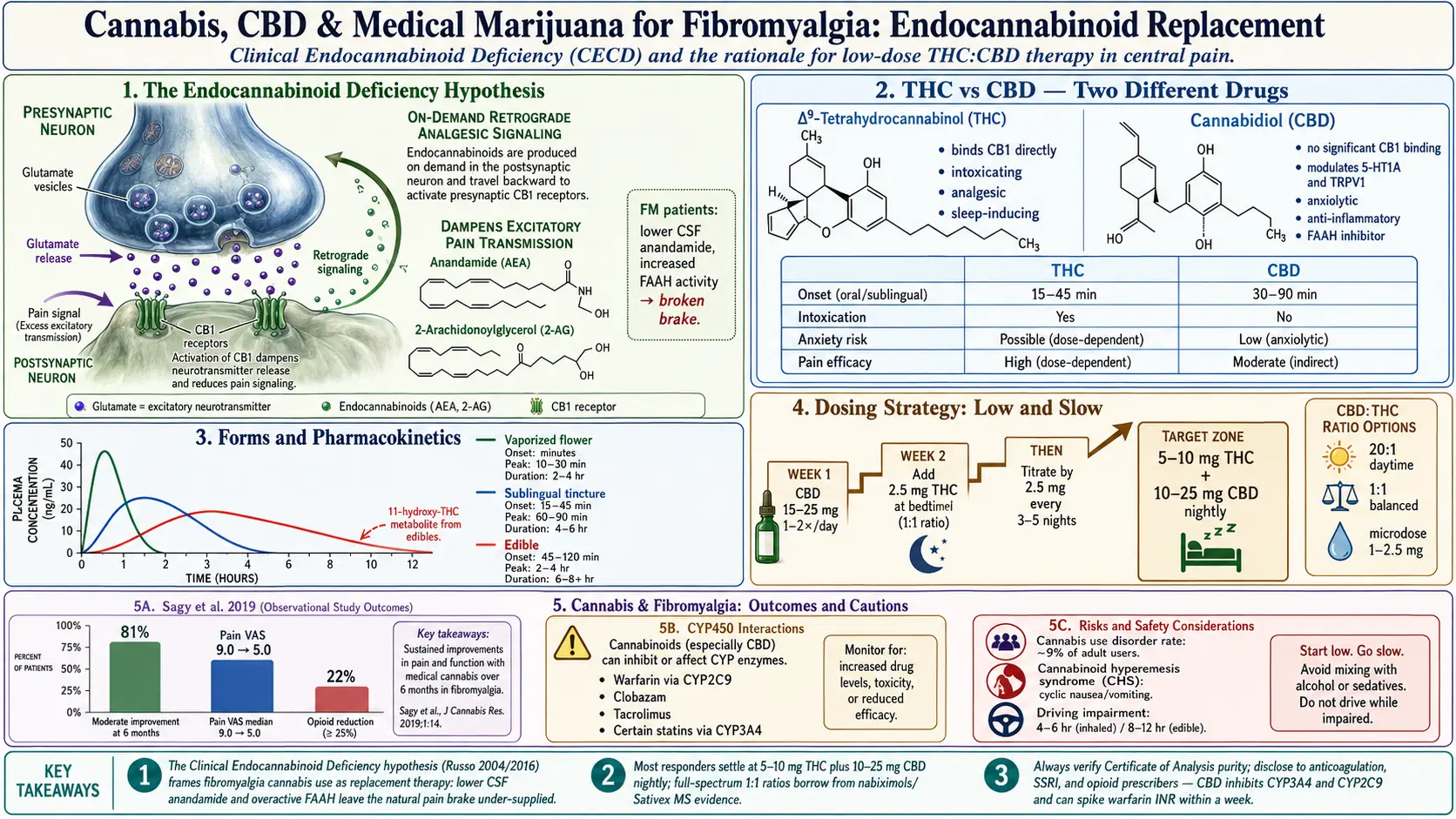
In 2004, cannabinoid researcher Ethan Russo proposed that fibromyalgia, migraine, and irritable bowel syndrome share an underlying feature he called Clinical Endocannabinoid Deficiency (CECD). He updated the theory in 2016 with a decade of supporting evidence. The idea: your body makes its own cannabis-like molecules — anandamide and 2-AG — that act on CB1 and CB2 receptors to dampen pain signalling, regulate sleep, and calm inflammation. In people with fibromyalgia, this system appears to run on empty. Cerebrospinal-fluid anandamide is lower. Enzymes that break down endocannabinoids may be more active. The net effect is an amplified pain system with one of its natural brakes missing.
If CECD is real, supplying outside cannabinoids is not recreational — it is replacement therapy, conceptually similar to giving thyroid hormone to a hypothyroid patient. The analogy is imperfect (we cannot measure an "endocannabinoid level" at a commercial lab), but it reframes the conversation away from "drug use" and toward physiology.
What the Evidence Actually Says
The evidence base for cannabis in fibromyalgia is suggestive, not definitive. A quick tour:
- Fiz et al. 2011 (PLoS ONE). A Spanish cross-sectional study of 56 fibromyalgia patients: 28 cannabis users and 28 non-users. Users reported significantly lower scores on pain, stiffness, and the Fibromyalgia Impact Questionnaire (FIQ), plus better sleep and mental-health scores, two hours after use.
- Sagy et al. 2019 (Journal of Clinical Medicine). A prospective six-month Israeli cohort of 367 fibromyalgia patients using medical cannabis. At six months, 81% reported at least moderate improvement, pain intensity dropped from a median 9.0 to 5.0 on a 10-point scale, and 22% stopped or reduced opioids. Adverse events were mostly mild: dizziness, dry mouth, fatigue.
- Ste-Marie et al. 2012 (Arthritis Care & Research). Showed that 13% of a Canadian fibromyalgia cohort were using cannabis, often with opioids, and that users had higher rates of unstable mental illness and unemployment — a warning that self-medication patterns can signal unmet need, not success.
- Earlier MS-era trials of nabiximols (Sativex) — a 1:1 THC:CBD oromucosal spray — established that THC/CBD combinations reduce central neuropathic pain and spasticity in multiple sclerosis. Those data are the single strongest mechanistic bridge to fibromyalgia, because both conditions involve central sensitization.
- What is missing: large, placebo-controlled, double-blind randomized trials in fibromyalgia specifically. Most published work is observational, short, or uses heterogeneous products. Publication bias favors positive results.
Honest summary: cannabis probably helps a majority of fibromyalgia patients who try it, but the effect size is modest, responders are hard to predict in advance, and rigorous evidence is thinner than the cultural enthusiasm suggests.
THC vs CBD — Two Very Different Drugs
"Cannabis" is shorthand for a plant that produces more than a hundred cannabinoids. Two dominate the conversation.
THC (delta-9-tetrahydrocannabinol) is the intoxicating compound. It binds CB1 receptors in the brain directly, producing the "high," sedation, appetite, and — relevant here — genuine analgesia and improved sleep onset. Downsides for fibromyalgia patients: next-day cognitive fog (already a fibro problem), anxiety or panic at higher doses, tachycardia, and in susceptible people, worsening of pre-existing anxiety or depression. THC tolerance develops quickly.
CBD (cannabidiol) is non-intoxicating. It does not meaningfully activate CB1. It modulates anxiety circuits (serotonin 5-HT1A, TRPV1), damps down pro-inflammatory cytokines, and may slow the breakdown of anandamide by inhibiting FAAH. Used alone, CBD is a mild-to-moderate anxiolytic and sleep aid, with modest direct pain effects. Most rigorous CBD-alone trials in chronic pain have been underwhelming — it helps, but less than marketing suggests.
For fibromyalgia, the practical implication is that CBD alone is safer but weaker, while THC adds real pain and sleep benefit at the cost of intoxication, next-day function, and anxiety risk. Most successful fibromyalgia regimens use some THC, usually a small amount, usually at night.
Ratios: 1:1, High-CBD, and Microdosing
Dispensaries label products by the CBD:THC ratio. A few common patterns:
- 1:1 balanced (e.g., 5 mg CBD : 5 mg THC). The ratio used in nabiximols/Sativex and the MS trials. CBD blunts THC's anxiety and cognitive side effects while preserving most of the pain benefit. A reasonable starting architecture for fibromyalgia patients who want meaningful relief and are comfortable with mild intoxication.
- High-CBD (e.g., 20:1 or 10:1). Daytime option. Most of the calming and anti-inflammatory effect, very little high. Good for anxiety and daytime pain without cognitive trade-off.
- THC-dominant (e.g., 1:2 or THC-only). Better for severe nighttime pain or insomnia, but high anxiety and tolerance risk. Reserve for bedtime.
- Microdosing. Using very small THC doses — 1 to 2.5 mg — often with CBD. Many fibromyalgia patients find this is the sweet spot: measurable pain and sleep benefit without feeling stoned the next morning.
A sensible first-month plan looks like: high-CBD product by day (20 to 40 mg CBD once or twice), plus a 1:1 or low-THC product at bedtime (start at 2.5 mg THC, titrate). Adjust based on what actually changes.
Forms and Kinetics: Tinctures, Flower, Edibles
The form matters as much as the dose because absorption kinetics differ enormously.
- Sublingual tinctures (oil under the tongue). Onset 15 to 45 minutes, peak at 60 to 90 minutes, duration 4 to 6 hours. Easy to dose precisely by the drop or milliliter. Best general-purpose starting form.
- Vaporized flower or concentrate. Onset within minutes, peak at 10 to 30 minutes, duration 2 to 4 hours. Fast relief for flare pain; less total THC exposure than combustion; easier to titrate in real time. Smoking (combustion) adds tar and respiratory irritation — vaporize instead.
- Edibles (gummies, capsules, baked goods). Onset 45 to 120 minutes, peak at 2 to 4 hours, duration 6 to 8 hours and occasionally longer. The hepatic first pass converts some delta-9 THC to 11-hydroxy-THC, a more potent metabolite — which is why edibles feel stronger than their mg number suggests and why overshooting is easy. Best for nighttime sleep coverage if you can dose conservatively.
- Topicals. CBD and THC creams can help localized joint or muscle pain without systemic absorption. A reasonable adjunct; unlikely to treat diffuse fibromyalgia pain on their own.
Dosing Strategy: Low and Slow
The single most common reason fibromyalgia patients give up on cannabis is that they took too much, too fast, and had a bad experience. A conservative protocol:
- Start with CBD alone for a week. 15 to 25 mg once or twice daily. Establish tolerance and watch for side effects.
- Introduce THC at night, 2.5 mg. Use a 1:1 tincture or low-dose edible. Take it 60 to 90 minutes before bedtime on a night you do not need to drive or work early the next morning.
- Hold the dose for 3 to 5 nights. Judge by sleep quality, morning pain, and next-day clarity — not just the first night.
- Titrate by 2.5 mg increments. Most fibromyalgia responders settle between 5 and 10 mg THC at night, often paired with 10 to 25 mg CBD.
- Revisit every 4 to 6 weeks. Tolerance can creep in. If you notice you need more for the same effect, take a 48-hour break before increasing.
If a dose makes you anxious, paranoid, or tachycardic: take more CBD (50 to 200 mg orally), hydrate, sit somewhere safe, and ride it out. CBD genuinely antagonizes acute THC anxiety. The experience is unpleasant but not dangerous in an otherwise healthy adult.
The Entourage Effect: Full-Spectrum vs Isolate
The entourage effect is the hypothesis that cannabis works better when its minor cannabinoids (CBG, CBN, CBC, THCV) and terpenes (myrcene, linalool, beta-caryophyllene) are present alongside the major ones. Full-spectrum products contain the full plant profile including trace THC; broad-spectrum removes THC but keeps the rest; isolate is purified CBD (or THC) alone.
Evidence for the entourage effect is mostly preclinical and anecdotal, but consistent enough that full-spectrum products are the default recommendation when legal. Isolate is a reasonable choice only if you are subject to THC drug testing or are unusually sensitive to THC.
Drug Interactions and Side Effects
Cannabinoids — particularly CBD at higher doses — inhibit several cytochrome P450 liver enzymes, notably CYP3A4 and CYP2C9. This raises blood levels of many drugs:
- Warfarin (CYP2C9). CBD can push INR dangerously high. If you take warfarin and start CBD, tell your anticoagulation clinic and expect more frequent INR checks for the first month.
- SSRIs and SNRIs. Combined sedation, mild serotonergic effects, possible increased SSRI levels. Usually manageable, but disclose the cannabis.
- Benzodiazepines, opioids, z-drugs (zolpidem), gabapentinoids. Additive sedation and respiratory depression. Be careful. Many fibromyalgia patients end up stacking several of these; cannabis on top is where falls and next-morning hangovers appear.
- Clobazam, tacrolimus, certain statins, amiodarone. Significant interactions; do not combine without physician input.
- Alcohol. Multiplies intoxication unpredictably. Keep doses separate or skip one.
Common side effects include dry mouth, dizziness, orthostatic drops in blood pressure (especially at first), appetite changes, fatigue, and mild cognitive slowing. Long-term risks: tolerance, cannabis use disorder in roughly 9% of adult users (higher with daily use), worsened anxiety or depression in a minority, and — rarely — cannabinoid hyperemesis syndrome, a paradoxical cyclic vomiting illness that only resolves with complete cessation. If you develop unexplained cyclic nausea and hot-shower-seeking behavior, stop cannabis and see a clinician.
Legality, Driving, Work, and Pharmaceuticals
Legal status in the United States remains a patchwork. As of 2026, hemp-derived CBD (under 0.3% THC) is federally legal, though FDA enforcement against unapproved health claims continues. THC-containing cannabis is legal for medical use in most states and adult use in a growing majority, but it remains a federal Schedule I/III controlled substance depending on rescheduling status. Consequences that matter in daily life:
- Driving. THC impairs reaction time and judgement. Per se THC limits vary by state; any detectable THC can be grounds for DUI in zero-tolerance states. Never drive within 4 to 6 hours of inhaled THC or 8 to 12 hours of edibles.
- Work. Safety-sensitive jobs (commercial driving, aviation, healthcare, federal employment) commonly test for THC, and THC metabolites linger in urine for days to weeks. CBD isolate is technically safer but contamination is common — see the purity section.
- Firearms. Federal ATF forms still ask about "unlawful use of marijuana" regardless of state legality. Honest answers can affect firearm purchases.
- International travel. Do not carry any cannabis across borders, even to another legal state via air.
- Prescription alternatives. Nabilone (Cesamet) is a synthetic THC-analog pill, FDA-approved for chemotherapy nausea but prescribed off-label for fibromyalgia pain and sleep in some clinics; small trials show benefit. Nabiximols (Sativex) is approved in the UK, Canada, and elsewhere for MS spasticity and is used off-label for chronic pain; not FDA-approved in the US. Epidiolex is purified pharmaceutical CBD, approved only for specific seizure disorders. These pharmaceutical options come with consistent dosing and insurance coverage (sometimes), but at a higher cost than dispensary products.
CBD Purity and the Certificate of Analysis
The CBD market is loosely regulated. Independent testing has repeatedly found products that contain less CBD than labelled, more THC than labelled, or contaminants — pesticides, heavy metals, residual solvents, and occasionally synthetic cannabinoids. The protection is the Certificate of Analysis (COA), a third-party lab report for the specific batch you are buying.
What to look for on a COA:
- Batch number matches the product in your hand.
- Potency panel confirms the CBD and THC milligrams per bottle match the label.
- Contaminant panels pass: pesticides, heavy metals (lead, cadmium, mercury, arsenic), microbials, mycotoxins, residual solvents.
- Lab name and date are visible, and the lab is ISO 17025 accredited.
Any vendor that cannot produce a current COA for the batch you are buying should be skipped. This is especially important if you are subject to drug testing — "THC-free" CBD isolates have failed plenty of workplace drug screens because the actual product contained traces of THC.
If You Are on Opioids, SSRIs, or Warfarin
This section is a warning, not a prohibition. Many fibromyalgia patients on opioids find that cannabis lets them reduce opioid dose over months, and large observational series support this. But opioid-cannabis combinations increase sedation and fall risk, and tapering opioids without your prescriber's knowledge is unsafe and can cost you your prescription. Bring cannabis into the conversation openly. Most pain clinics in legal states now have policies that accommodate medical cannabis use; some still do not, and you need to know which camp your prescriber is in before you start.
On SSRIs or SNRIs, disclose cannabis to your prescriber — not because the combination is usually dangerous, but because side-effect attribution becomes impossible otherwise. On warfarin, do not start any cannabinoid product without telling your anticoagulation clinic; INR can jump within a week. On clobazam or tacrolimus, do not start CBD without a pharmacist-led interaction review.
Cannabis complements — it does not replace — the core fibromyalgia toolkit: LDN, SNRIs where tolerated, serious sleep repair, graded movement, and correction of nutrient gaps. A realistic goal is a 20 to 40% reduction in pain and meaningful improvement in sleep — not a cure.
Key Research Papers
- Sagy I, et al. Safety and Efficacy of Medical Cannabis in Fibromyalgia. J Clin Med. 2019;8(6):807.
- Fiz J, et al. Cannabis Use in Patients with Fibromyalgia: Effect on Symptoms Relief and Health-Related Quality of Life. PLoS ONE. 2011;6(4):e18440.
- Russo EB. Clinical Endocannabinoid Deficiency Reconsidered: Current Research Supports the Theory in Migraine, Fibromyalgia, Irritable Bowel, and Other Treatment-Resistant Syndromes. Cannabis Cannabinoid Res. 2016;1(1):154–165.
- Ste-Marie PA, et al. Association of Herbal Cannabis Use With Negative Psychosocial Parameters in Patients With Fibromyalgia. Arthritis Care Res. 2012;64(8):1202–1208.
- Search PubMed
- Ware MA, et al. The effects of nabilone on sleep in fibromyalgia: results of a randomized controlled trial. Anesth Analg. 2010;110(2):604–610.
PubMed Topic Searches
For current peer-reviewed work, the following searches return live PubMed results:
- Cannabis and fibromyalgia
- CBD and fibromyalgia
- Clinical endocannabinoid deficiency
- Nabilone and fibromyalgia
- Nabiximols (Sativex) and chronic pain
- THC:CBD ratio in chronic pain
- Cannabidiol drug interactions and CYP enzymes
- Cannabinoid hyperemesis syndrome
- Medical cannabis and opioid reduction
- Cannabis and central sensitization
Connections
- Fibromyalgia Overview
- Nutrient Gaps in Fibromyalgia
- Low-Dose Naltrexone for Fibromyalgia
- Sleep and Non-Restorative Sleep
- Exercise Pacing and Graded Movement
- Chronic Pain
- Insomnia
- Fibromyalgia and ME/CFS Overlap
- ACR 2016 Diagnostic Criteria
- Central Sensitization Explained
- Small-Fiber Neuropathy Overlap
- Anxiety
- Depression
- Fatigue
- Low-Dose Naltrexone
- Arthritis