Tendinitis
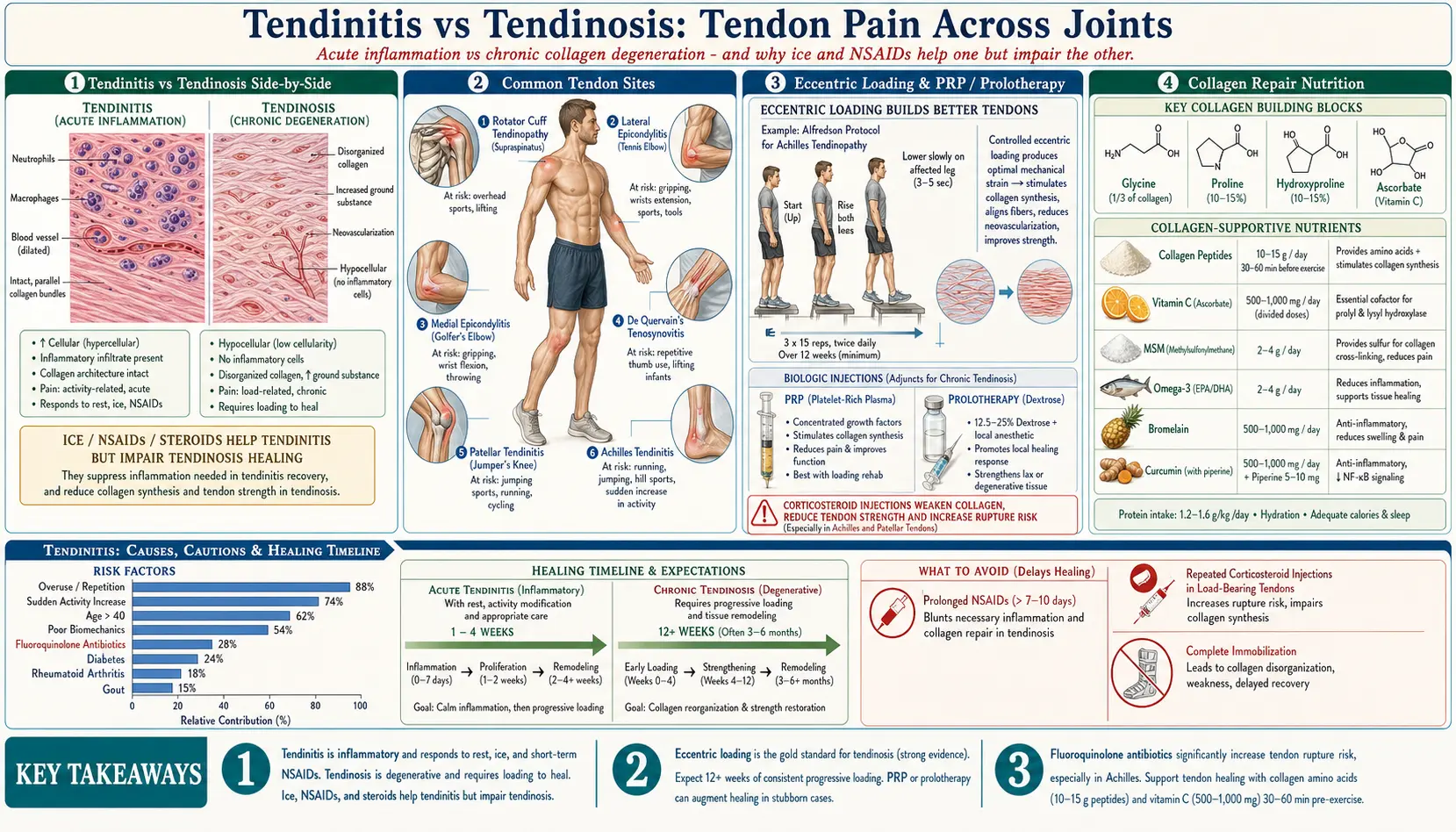
Table of Contents
- What Is Tendinitis?
- Tendinitis vs. Tendinosis
- Common Types of Tendinitis
- Causes and Mechanisms
- Symptoms and Diagnosis
- Conventional Treatment
- Natural and Naturopathic Approaches
- Prolotherapy and PRP
- Eccentric Exercises
- Ergonomic Modifications
- Tendon Nutrition and Blood Supply
- Important Cautions
- References & Research
- Featured Videos
What Is Tendinitis?
Tendinitis (also spelled tendonitis) is the acute inflammation or irritation of a tendon, the thick fibrous cord that attaches muscle to bone. Tendons transmit the force of muscle contraction to the skeleton, enabling movement. When a tendon becomes inflamed due to overuse, injury, or poor biomechanics, the result is pain, swelling, and impaired function at the affected joint.
Tendinitis can occur in virtually any tendon in the body but most commonly affects the shoulders, elbows, wrists, knees, and heels. While often considered a minor condition, untreated tendinitis can progress to chronic tendon degeneration, significantly limiting mobility and quality of life.
Tendinitis vs. Tendinosis
Understanding the distinction between tendinitis and tendinosis is critical for proper treatment:
- Tendinitis: Acute inflammation of the tendon, typically occurring in the early stages of injury. Inflammatory cells are present, and the condition usually responds to anti-inflammatory interventions. Duration is typically days to a few weeks.
- Tendinosis: Chronic degeneration of the tendon's collagen fibers without significant inflammation. The tendon shows disorganized collagen, increased ground substance, and neovascularization (new, abnormal blood vessel growth). This condition develops over weeks to months of continued stress.
Most cases that patients describe as "tendinitis" are actually tendinosis by the time they seek treatment. This distinction matters because anti-inflammatory treatments (ice, NSAIDs, corticosteroid injections) may help true tendinitis but can actually impair healing in tendinosis, where the goal is to stimulate collagen repair rather than suppress inflammation.
Common Types of Tendinitis
Lateral Epicondylitis (Tennis Elbow)
Affects the tendons on the outside of the elbow, specifically the extensor carpi radialis brevis. Despite the name, it is far more common in non-athletes, particularly people who perform repetitive gripping, typing, or manual labor. Pain radiates from the outer elbow into the forearm and wrist.
Medial Epicondylitis (Golfer's Elbow)
Involves the tendons on the inside of the elbow (flexor-pronator mass). Common in golfers, throwing athletes, and workers who perform repetitive wrist flexion or forearm pronation. Pain is localized to the inner elbow and may radiate down the forearm.
Achilles Tendinitis
Inflammation of the Achilles tendon, the largest and strongest tendon in the body, connecting the calf muscles to the heel bone. Common in runners, particularly those who suddenly increase training intensity. Can occur at the mid-portion of the tendon or at its insertion point on the calcaneus.
Rotator Cuff Tendinitis
Affects one or more of the four rotator cuff tendons (supraspinatus, infraspinatus, teres minor, subscapularis), most commonly the supraspinatus. Often caused by repetitive overhead movements in swimming, throwing, or overhead work. Pain occurs with arm elevation and can disturb sleep when lying on the affected side.
Patellar Tendinitis (Jumper's Knee)
Inflammation of the patellar tendon connecting the kneecap to the shinbone. Prevalent in athletes who perform frequent jumping (basketball, volleyball) or running. Pain is localized just below the kneecap and worsens with squatting, jumping, or climbing stairs.
De Quervain's Tenosynovitis
Affects the tendons of the thumb (abductor pollicis longus and extensor pollicis brevis) as they pass through a narrow tunnel at the wrist. Common in new parents from repeatedly lifting infants, and increasingly seen with heavy smartphone use. Pain occurs at the thumb side of the wrist and may radiate into the thumb or forearm.
Causes and Mechanisms
- Overuse and repetitive strain: The most common cause. Repetitive motions create microtears in the tendon faster than the body can repair them. This is particularly problematic in tendons with limited blood supply.
- Sudden increase in activity: Rapidly increasing exercise intensity, duration, or frequency without adequate adaptation time (the "too much, too soon" phenomenon).
- Poor biomechanics: Faulty movement patterns, muscle imbalances, or poor posture place abnormal stress on tendons. Examples include running with excessive pronation or poor shoulder mechanics during overhead activities.
- Aging: Tendons become less elastic, less hydrated, and more susceptible to injury with age. Collagen turnover slows, and blood supply diminishes. Tendinitis becomes increasingly common after age 40.
- Inadequate warm-up: Exercising with cold, unstretched muscles and tendons increases strain on tendon fibers.
- Equipment and ergonomics: Improper workstation setup, ill-fitting shoes, worn-out athletic footwear, or incorrect tool grip sizes can all contribute.
- Medications: Fluoroquinolone antibiotics (ciprofloxacin, levofloxacin) are associated with increased risk of tendinitis and tendon rupture, particularly of the Achilles tendon. Statins may also impair tendon health in some individuals.
- Systemic conditions: Diabetes, rheumatoid arthritis, thyroid disorders, and gout increase tendinitis risk through metabolic and inflammatory mechanisms.
Symptoms and Diagnosis
Common symptoms of tendinitis include:
- Pain: Localized to the tendon, typically described as a dull ache that sharpens with movement or activity. Pain often worsens with use and improves with rest in early stages.
- Tenderness: The tendon is painful when pressed or palpated.
- Swelling: Mild to moderate swelling around the affected tendon, sometimes with warmth.
- Stiffness: The affected joint feels stiff, particularly in the morning or after periods of inactivity.
- Crepitus: A crackling or grating sensation when the tendon moves through its sheath.
- Weakness: Reduced strength in the affected muscle-tendon unit, either from pain inhibition or tendon damage.
Diagnosis is primarily clinical, based on history and physical examination. Imaging may include ultrasound (excellent for visualizing tendon structure, thickness, and tears) or MRI (gold standard for detailed tendon assessment). X-rays do not show tendons but can identify calcific tendinitis or bony abnormalities.
Conventional Treatment
RICE Protocol
The traditional first-line approach for acute tendinitis:
- Rest: Relative rest from the aggravating activity (not complete immobilization, which can impair healing).
- Ice: Applied for 15-20 minutes several times daily to reduce acute inflammation and pain.
- Compression: Elastic bandaging to reduce swelling.
- Elevation: Raising the affected limb above heart level when possible.
NSAIDs
Non-steroidal anti-inflammatory drugs (ibuprofen, naproxen) can reduce pain and inflammation in acute tendinitis. However, prolonged use may impair tendon healing by suppressing the inflammatory cascade needed for tissue repair. Short courses of 7-10 days are generally recommended.
Corticosteroid Injections
Provide rapid pain relief by powerfully suppressing inflammation. However, evidence shows that corticosteroids weaken tendon collagen, increase the risk of tendon rupture (particularly in the Achilles tendon), and are associated with worse long-term outcomes compared to physical therapy alone. Most clinicians now limit injections to 1-2 per tendon site and avoid them in load-bearing tendons.
Physical Therapy
The cornerstone of tendinitis treatment. A physical therapist can identify biomechanical contributors, provide manual therapy, prescribe progressive loading exercises, and use modalities such as ultrasound therapy and dry needling to promote healing.
Natural and Naturopathic Approaches
Naturopathic management of tendinitis focuses on providing the raw materials for tendon repair, reducing inflammation through natural pathways, and optimizing the healing environment:
Collagen Peptides
Hydrolyzed collagen supplementation (10-15 grams daily) provides the specific amino acids (glycine, proline, hydroxyproline) needed for tendon repair. Research shows that taking collagen peptides with vitamin C 30-60 minutes before exercise increases collagen synthesis in tendons and ligaments. Type I collagen is the predominant form in tendons.
Vitamin C
Essential for collagen synthesis through its role in the hydroxylation of proline and lysine residues. Vitamin C deficiency impairs tendon repair. Supplementation of 500-1000 mg daily supports collagen production and provides antioxidant protection against oxidative damage at the injury site.
MSM (Methylsulfonylmethane)
An organic sulfur compound that supports connective tissue integrity and has mild anti-inflammatory properties. Sulfur is a critical component of the structural proteins in tendons and cartilage. Typical dosing is 2-4 grams daily.
Omega-3 Fatty Acids
EPA and DHA (2-4 grams daily of combined fish oil) modulate the inflammatory response by promoting the production of resolvins and protectins, specialized pro-resolving mediators that help resolve inflammation without suppressing the healing process.
Bromelain
A proteolytic enzyme derived from pineapple stems with demonstrated anti-inflammatory and anti-edema effects. Bromelain reduces swelling and pain when taken on an empty stomach (500-1000 mg daily between meals). It works by modulating prostaglandin synthesis and reducing fibrin accumulation.
Turmeric and Curcumin
Curcumin, the active compound in turmeric, is a potent anti-inflammatory that inhibits NF-kB, COX-2, and multiple inflammatory cytokines. Use bioavailable forms (with piperine, phospholipid complex, or nano-formulated) at doses of 500-1000 mg curcuminoids daily.
Topical Arnica
Arnica montana gel or cream applied topically to the affected tendon can reduce pain and swelling. Clinical trials support its efficacy comparable to topical NSAIDs for musculoskeletal pain, with fewer side effects.
DMSO (Dimethyl Sulfoxide)
A naturally occurring solvent with potent anti-inflammatory and analgesic properties when applied topically. DMSO penetrates the skin rapidly and can reduce tendon pain and swelling. Typically applied as a 70% solution. It may cause a garlic-like taste and mild skin irritation. Use pharmaceutical-grade DMSO only.
Prolotherapy and PRP
Regenerative injection therapies represent an important treatment category for chronic tendinitis and tendinosis:
Prolotherapy
Involves injecting a dextrose (sugar water) solution into and around the damaged tendon. The controlled irritation triggers a localized inflammatory response that stimulates the body's natural healing cascade, including fibroblast proliferation and new collagen deposition. A series of 3-6 injections spaced 2-4 weeks apart is typical. Multiple studies support its efficacy for lateral epicondylitis, Achilles tendinopathy, and rotator cuff tendinitis.
Platelet-Rich Plasma (PRP)
The patient's own blood is drawn and centrifuged to concentrate platelets, which are rich in growth factors (PDGF, TGF-beta, VEGF, IGF-1). The concentrated platelet solution is then injected directly into the damaged tendon. PRP provides a concentrated dose of the body's own healing factors and has shown particular promise for chronic tendon injuries that have failed conservative treatment.
Eccentric Exercises
Eccentric exercises (controlled lengthening of the muscle-tendon unit under load) are considered the gold standard exercise intervention for tendinopathy:
- Mechanism: Eccentric loading stimulates tendon remodeling by promoting aligned collagen fiber production and increasing tendon cross-sectional area. It also disrupts the abnormal neovascularization (new blood vessel and nerve growth) associated with tendinosis.
- Achilles tendinitis protocol: The Alfredson protocol involves performing eccentric heel drops (3 sets of 15 repetitions, twice daily) from the edge of a step. This has a 60-90% success rate for mid-portion Achilles tendinopathy.
- Tennis elbow protocol: The Tyler Twist using a FlexBar, or eccentric wrist extensions with a light dumbbell (3 sets of 15 repetitions daily), have strong evidence for lateral epicondylitis.
- Patellar tendinitis: Single-leg eccentric squats on a decline board (25-degree angle) are the standard protocol.
Eccentric exercises should be performed slowly (taking 3-5 seconds per repetition) and may cause mild discomfort during performance but should not cause lasting pain. Improvement typically occurs over 6-12 weeks of consistent daily practice.
Ergonomic Modifications
Addressing the environmental and biomechanical factors that contribute to tendinitis is essential for both treatment and prevention:
- Workstation setup: Monitor at eye level, elbows at 90 degrees, wrists in neutral position, feet flat on the floor. Use an ergonomic keyboard and mouse to reduce strain on forearm tendons.
- Grip modification: Use larger grip handles on tools and racquets to reduce forearm tendon strain. Counterforce braces (tennis elbow straps) can reduce tension on the tendon origin.
- Footwear: Proper shoes with adequate arch support and cushioning. Replace running shoes every 300-500 miles. Custom orthotics may be necessary for biomechanical imbalances contributing to Achilles or patellar tendinitis.
- Activity modification: Take regular breaks during repetitive tasks (5 minutes every 30-60 minutes). Alternate between different activities to avoid sustained tendon loading. Gradually increase workload when returning to activity.
- Technique correction: Work with a coach or therapist to optimize movement patterns in sports and occupational tasks. Poor form is a leading contributor to tendinitis.
Tendon Nutrition and Blood Supply
Understanding tendon biology is crucial for effective naturopathic treatment:
- Blood supply: Tendons have relatively poor blood supply compared to muscles, which is why they heal slowly. The mid-portion of many tendons (such as the Achilles) is a "watershed zone" with particularly limited vascularity, making it vulnerable to degeneration and slow to recover.
- Collagen composition: Tendons are composed primarily of type I collagen (approximately 85% of dry weight), arranged in parallel fibers for maximum tensile strength. Collagen turnover in tendons is slow, with a half-life estimated at 200 days or more.
- Nutritional support: Tendons require adequate protein intake (1.2-1.6 g/kg body weight daily), vitamin C, zinc, copper, and manganese for proper collagen synthesis and cross-linking. Silica (from horsetail herb or dietary sources) also supports connective tissue integrity.
- Hydration: Tendons are 60-70% water. Adequate hydration is essential for maintaining the proteoglycan matrix that gives tendons their viscoelastic properties and allows nutrient diffusion.
- Blood flow enhancement: Gentle, pain-free movement of the affected tendon promotes blood flow and nutrient delivery. Complete rest may actually slow healing by reducing an already limited blood supply.
Important Cautions
- Do not ignore persistent tendon pain. Continuing to load an inflamed or degenerating tendon can lead to partial or complete tendon rupture, which may require surgical repair.
- Corticosteroid injections carry significant risks, including tendon weakening and rupture. Discuss risks thoroughly with your provider, and avoid injections into the Achilles tendon or if partial tears are suspected.
- Fluoroquinolone antibiotics (ciprofloxacin, levofloxacin, moxifloxacin) significantly increase tendon rupture risk, particularly in patients over 60 and those taking corticosteroids concurrently. Inform your healthcare provider about any tendon issues if prescribed these medications.
- Bromelain and omega-3 supplements have mild blood-thinning properties. Use with caution if taking anticoagulant or antiplatelet medications, and discontinue before surgery.
- DMSO should only be pharmaceutical-grade. Industrial-grade DMSO may contain harmful impurities. Because DMSO readily penetrates the skin and can carry other substances with it, avoid applying it over areas with topical medications or chemicals.
- Eccentric exercises may initially increase discomfort. Some mild discomfort during the exercise is acceptable, but sharp pain or lasting soreness beyond 24 hours indicates that the load should be reduced.
- Seek immediate medical attention if you experience a sudden pop or snap in a tendon, sudden inability to move a joint, or significant bruising and deformity, as these may indicate a tendon rupture.
13. References & Research
Historical Background
Tendon disorders have been recognized since antiquity, with Hippocrates describing tendon injuries around 400 BCE. The distinction between tendinitis (inflammatory) and tendinosis (degenerative) was clarified by Puddu and colleagues in 1976. Hakan Alfredson developed his landmark eccentric exercise protocol for Achilles tendinopathy in 1998, which transformed conservative treatment of tendon disorders.
Key Research Papers
- Alfredson H, et al. Heavy-load eccentric calf muscle training for the treatment of chronic Achilles tendinosis. American Journal of Sports Medicine. 1998;26(3):360-366.
- Cook JL, Purdam CR. Is tendon pathology a continuum? A pathology model to explain the clinical presentation of load-induced tendinopathy. British Journal of Sports Medicine. 2009;43(6):409-416.
- Khan KM, et al. Histopathology of common tendinopathies: update and implications for clinical management. Sports Medicine. 1999;27(6):393-408.
- Nirschl RP, Ashman ES. Elbow tendinopathy: tennis elbow. Clinics in Sports Medicine. 2003;22(4):813-836.
- Tyler TF, et al. Addition of isolated wrist extensor eccentric exercise to standard treatment for chronic lateral epicondylosis: a prospective randomized trial. Journal of Hand Therapy. 2010;23(3):248-254.
- Maffulli N, et al. Tendon healing: can it be optimised? British Journal of Sports Medicine. 2002;36(5):315-316.
- Coombes BK, et al. Effect of corticosteroid injection, physiotherapy, or both on clinical outcomes in patients with unilateral lateral epicondylalgia: a randomized controlled trial. JAMA. 2013;309(5):461-469.
- Bisset L, et al. Mobilisation with movement and exercise, corticosteroid injection, or wait and see for tennis elbow: randomised trial. BMJ. 2006;333(7575):939.
- de Vos RJ, et al. Platelet-rich plasma injection for chronic Achilles tendinopathy: a randomized controlled trial. JAMA. 2010;303(2):144-149.
- Malliaras P, et al. Patellar tendinopathy: clinical diagnosis, load management, and advice for challenging case presentations. Journal of Orthopaedic & Sports Physical Therapy. 2015;45(11):887-898.
- Shaw HM, Benjamin M. Structure-function relationships of entheses in relation to mechanical load and exercise. Scandinavian Journal of Medicine & Science in Sports. 2007;17(4):303-315.
- Millar NL, et al. Tendinopathy. Nature Reviews Disease Primers. 2021;7(1):1-21.
Research Papers
- Clinical trials on tendinitis — PubMed search
- Systematic reviews of tendinitis — PubMed search
- Meta-analyses on tendinitis — PubMed search
- Treatment research on tendinitis — PubMed search
- Mechanism studies of tendinitis — PubMed search
- Epidemiology of tendinitis — PubMed search
Connections
- Orthopedics
- Collagen
- Turmeric
- Herniated Disc
- Carpal Tunnel Syndrome
- Fibromyalgia
- Magnesium
- Anti-Inflammatory Diet
- Vitamin C
- Arthritis
- Diabetes
- Thyroid Disorders
- Proline
- Sulfur
- Omega-3 Fatty Acids
- Edema
- Sciatica
- Joint Pain
- Exercise and PT Protocol
- Osteoarthritis
- Plantar Fasciitis
- Frozen Shoulder