Sleep and Non-Restorative Sleep in Fibromyalgia
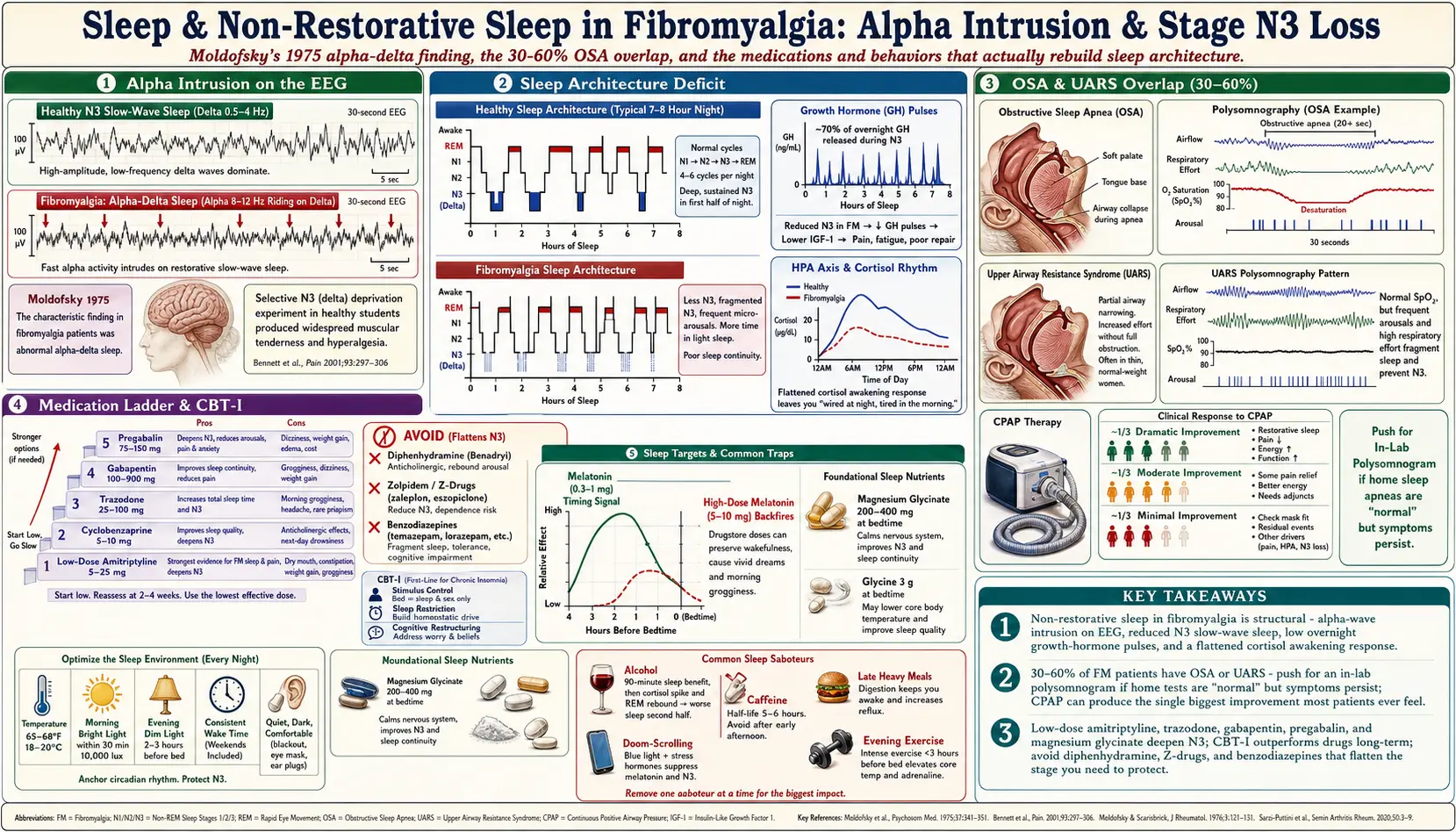
Table of Contents
- What “Non-Restorative Sleep” Actually Means
- Moldofsky and the Alpha-Intrusion Finding
- The Stage N3 (Slow-Wave) Deficit
- HPA Axis, Growth Hormone, and Why You Wake Up Sore
- When to Get a Sleep Study
- OSA, UARS, and the 30–60% Overlap
- Restless Legs and PLMD
- CPAP When Indicated
- Bedtime Protocol: Light, Temperature, Schedule
- Medication Options — Pros, Cons, Dosing
- Why Melatonin Alone Rarely Fixes It — and Where Magnesium Glycinate Fits
- CBT-I: The Treatment Nobody Offers You
- Common Traps: Alcohol, Late Caffeine, Doom-Scrolling
- Key Research Papers
- Connections
- Featured Videos
What “Non-Restorative Sleep” Actually Means
If you have fibromyalgia, you already know the pattern. You go to bed tired. You fall asleep — maybe quickly, maybe after an hour of staring at the ceiling. You might sleep eight hours by the clock. And you wake up feeling as if you have been run over by a truck. Stiff. Foggy. Somehow more exhausted than when you lay down.
That is non-restorative sleep. It is not the same as insomnia, although the two often coexist. Insomnia is a problem of quantity — you cannot get enough hours. Non-restorative sleep is a problem of quality — the hours are there, but the repair work that sleep is supposed to do never happens. Roughly 90% of fibromyalgia patients report this symptom, and in the ACR 2016 diagnostic criteria, non-restorative sleep is not a side effect of the disease. It is one of the core features used to diagnose it.
This article is about why sleep breaks in fibromyalgia, how to figure out which flavor of broken you have, and what actually helps — not just platitudes about “good sleep hygiene.” If you have been told to “try melatonin and a warm bath,” you already know that advice rarely moves the needle. There is more to it than that.
Moldofsky and the Alpha-Intrusion Finding
In 1975, a Canadian sleep researcher named Harvey Moldofsky published one of the most influential fibromyalgia papers ever written. He hooked up patients with what was then called “fibrositis” to EEG machines overnight and discovered something strange. During deep sleep — the phase where brain waves should be slow and rolling, like ocean swells — their EEGs showed a faster, jagged wave pattern riding on top. That faster rhythm, around 8–12 Hz, is called the alpha rhythm, and it belongs to quiet wakefulness, not deep sleep.
Moldofsky called this alpha-delta sleep or alpha intrusion: the waking brain refusing to let go even while the body was, by every other measure, asleep. Then he did something even more striking. He took healthy university students and woke them up every time their EEG slipped into deep sleep — selectively depriving them of stage N3 for several nights in a row. Within days, those healthy volunteers developed diffuse muscle aches, tender points, and morning stiffness. The symptoms disappeared once they were allowed normal sleep again.
That experiment is the foundation of the idea that in fibromyalgia, disordered deep sleep is not just a symptom — it is part of what drives the pain. Fifty years later, the mechanism has been refined and re-interpreted many times, but Moldofsky’s core observation has held up.
The Stage N3 (Slow-Wave) Deficit
Sleep comes in stages. Stage N1 is the drowsy edge as you drift off. N2 is light sleep, about half your night. N3 is slow-wave sleep — the deepest, most physically restorative phase. REM is the dreaming phase. You cycle through these roughly every 90 minutes, and most of your N3 happens in the first third of the night.
Polysomnography studies consistently show that fibromyalgia patients get less N3, more fragmented N3, and more micro-arousals (brief wake-ups so short you do not remember them). Roizenblatt and colleagues, in a 2001 study in Arthritis & Rheumatism, documented the alpha-intrusion pattern in a larger cohort and linked its severity to pain scores and fatigue. The worse the sleep architecture, the worse the daytime symptoms.
Why does this matter? Because N3 is when a long list of maintenance jobs happens: the glymphatic system flushes metabolic waste from the brain, the immune system regulates inflammatory cytokines, muscles repair micro-damage, and the pituitary releases the majority of your growth hormone pulse. Miss enough N3 and every one of those jobs falls behind. That is, in plain language, why you wake up feeling like you did not sleep at all.
HPA Axis, Growth Hormone, and Why You Wake Up Sore
Two hormonal systems take the biggest hit when deep sleep is disrupted.
Growth hormone (GH). About 70% of your daily GH is released in pulses during N3. In adults, growth hormone is not about getting taller — it drives tissue repair, collagen turnover, and IGF-1 production. Fibromyalgia patients have measurably lower IGF-1 levels on average, consistent with chronic GH under-secretion. That is a plausible reason why minor exertion leaves you sore for days: the overnight repair cycle is running on a fraction of its normal output.
HPA axis (hypothalamic-pituitary-adrenal). This is your stress-and-cortisol system. Normally cortisol bottoms out around midnight and surges just before you wake — the cortisol awakening response. In fibromyalgia, that rhythm is flattened. Cortisol stays mildly elevated through the night (keeping you “wired”) and does not rise properly in the morning (leaving you “tired”). The result is the classic fibro paradox: wired at bedtime, exhausted at 9 a.m.
You cannot fix either of these systems by willpower. You can influence them by protecting whatever N3 you still have, treating any co-existing sleep disorder that fragments it further, and using medications or routines that deepen sleep architecture rather than just knocking you unconscious.
When to Get a Sleep Study
Many fibromyalgia patients go years without a formal sleep evaluation because their doctor chalks the fatigue up to “the fibro.” That is a mistake. A sleep study (polysomnogram, or PSG) is warranted if you have any of the following on top of non-restorative sleep:
- Loud snoring, witnessed pauses in breathing, or gasping awake.
- Morning headaches that fade through the day.
- Dry mouth or sore throat every morning.
- High blood pressure that is hard to control.
- A neck circumference over 16 inches (women) or 17 inches (men).
- BMI over 30 — although thin patients get OSA too.
- Kicking or jerking legs that your partner notices.
- Daytime sleepiness severe enough to nod off while driving, reading, or in meetings.
Home sleep apnea tests are cheaper and more convenient, but they can miss upper airway resistance syndrome (UARS) and central apneas. If you have fibromyalgia and a home test comes back “normal” but your symptoms persist, push for an in-lab polysomnogram. The lab study captures EEG, leg movements, airflow, oxygen, and breathing effort — all of which matter for you specifically.
OSA, UARS, and the 30–60% Overlap
This is the single most under-appreciated fact in fibromyalgia care. Depending on the study, 30% to 60% of fibromyalgia patients have obstructive sleep apnea (OSA). The range is wide because screening criteria differ, but even the low end is staggeringly high compared to the general population (roughly 10–15%). In men with fibromyalgia, rates cluster near the top of that range.
OSA means your upper airway collapses partially or fully dozens or hundreds of times an hour while you sleep. Each collapse drops your oxygen and jolts you into a micro-arousal you do not remember. Those micro-arousals destroy N3. If you have fibromyalgia and untreated OSA, you have two engines wrecking your sleep architecture, and no amount of melatonin, amitriptyline, or sleep hygiene will fix the apnea piece.
UARS is the quieter cousin. Your airway does not fully collapse, but it narrows enough to make you work harder to breathe. You do not drop your oxygen, so a crude home test misses it, but the extra respiratory effort still triggers arousals. UARS patients are often thin women — exactly the demographic most likely to be told “you can’t have sleep apnea, you’re not overweight.” That dismissal is wrong. UARS requires esophageal pressure monitoring or a careful in-lab study to catch.
If any part of your history fits, get evaluated. Treating OSA or UARS can produce the single biggest improvement in fibromyalgia symptoms most patients ever experience.
Restless Legs and PLMD
Restless legs syndrome (RLS) and periodic limb movement disorder (PLMD) are also over-represented in fibromyalgia, with prevalence estimates of 30–40%. RLS is the conscious, crawling, have-to-move sensation you get in the evening. PLMD is the involuntary leg jerking during sleep that you may not notice but your partner will.
Both fragment sleep, and both are often driven by low brain iron even when your blood iron looks “normal.” Ask for a ferritin level. If it is under 75 ng/mL (some specialists use 100), oral or IV iron supplementation frequently resolves RLS within weeks. Other triggers include SSRIs, SNRIs, and diphenhydramine (the antihistamine in Benadryl and most over-the-counter sleep aids) — all of which can worsen RLS and are commonly prescribed for fibromyalgia sleep complaints. Many patients are trapped in a loop where the drug for sleep is causing the leg problem that ruins the sleep.
CPAP When Indicated
If your sleep study shows an AHI (apnea-hypopnea index) over 5 with symptoms, or over 15 without, the treatment is usually continuous positive airway pressure (CPAP). CPAP blows a steady stream of air that splints your airway open.
CPAP has a reputation for being intolerable. Modern machines are quiet, the masks come in dozens of shapes, and the ramp features ease you in. The two keys to adherence are mask fit and pressure titration. If you hate your first mask, ask for a different style — nasal pillow, nasal mask, full face — until one works. If the pressure feels suffocating, ask about a BiPAP (separate inhale and exhale pressures) or an APAP (auto-adjusting). Insurance usually covers them.
Fibromyalgia patients who stick with CPAP report outcomes in three buckets. A third feel dramatically better within a month — more energy, less pain, clearer head. A third feel moderate improvement. A third feel little change, usually because the apnea was not the main driver of their symptoms. Even in the last group, treating OSA is still worth it for cardiovascular and cognitive reasons.
Bedtime Protocol: Light, Temperature, Schedule
Sleep hygiene is boring, overprescribed advice — and for fibromyalgia, it is still the foundation everything else sits on. Three variables matter more than the rest.
Light. Your brain sets its circadian clock from light, not clocks. Get bright outdoor light within 30 minutes of waking — even 10 minutes on a cloudy day is stronger than any indoor bulb. In the evening, dim household lights after sunset and kill blue-heavy screen light in the last hour before bed (night-shift modes help; amber glasses help more). If you have ever fallen asleep fine on vacation and lain awake for hours at home, your evening light exposure is probably the difference.
Temperature. Your core body temperature has to drop about 1–2°F to initiate and maintain deep sleep. A bedroom at 65–68°F (18–20°C) is the sweet spot for most adults. A hot bath or shower 90 minutes before bed sounds counterintuitive but works by dilating surface blood vessels and then rebound-cooling your core faster. Cooling mattress pads (Chilipad, Eight Sleep) are overpriced but genuinely help light sleepers.
Schedule. A consistent wake time every single day, weekends included, is worth more than a consistent bedtime. Pick a wake time, protect it, and bedtime will sort itself out. Variable wake times confuse the circadian clock and lock in fragmented sleep even when total hours look fine on paper.
Medication Options — Pros, Cons, Dosing
No drug fixes fibromyalgia sleep, but several partially rebuild sleep architecture or ease the specific bottleneck you are stuck on. All of these are off-label for sleep in most cases; doses below are starting ranges and every one needs a prescriber.
Low-dose amitriptyline (Elavil). 5–25 mg at bedtime. The single most-studied fibromyalgia sleep drug. A tricyclic antidepressant in full doses (150 mg), but at 10–25 mg it is a sleep and pain modulator. Pros: deepens N3, reduces pain, cheap, decades of data. Cons: morning grogginess, dry mouth, constipation, weight gain, avoid if you have heart rhythm problems or glaucoma. Take 2–3 hours before bed, not at lights-out.
Cyclobenzaprine (Flexeril). 5–10 mg at bedtime. Structurally similar to amitriptyline. Pros: relaxes muscles, improves perceived sleep quality, useful if stiffness is a big part of your presentation. Cons: next-day sedation, dry mouth, tolerance after a few weeks in many patients. Some clinicians rotate it 5 nights on, 2 nights off to preserve effect.
Trazodone. 25–100 mg at bedtime. A serotonin modulator that at low doses is primarily sedating. Pros: non-habit-forming, helps sleep maintenance (not just onset), well-tolerated long-term, cheap. Cons: hangover, orthostatic dizziness, rarely priapism in men. A reasonable first-line for patients who cannot tolerate tricyclics.
Gabapentin (Neurontin). 100–900 mg at bedtime. A seizure drug with pain-modulating and sleep-deepening effects in the fibromyalgia population. Pros: improves slow-wave sleep, reduces nerve-type pain, useful if RLS is also present. Cons: weight gain, dizziness, swelling, withdrawal if stopped abruptly. Titrate up slowly over 1–2 weeks.
Pregabalin (Lyrica). 75–150 mg at bedtime, up to 450 mg/day in divided doses. FDA-approved for fibromyalgia. Similar mechanism to gabapentin with more predictable absorption. Pros: approved indication, proven sleep and pain benefit. Cons: expensive, same side-effect profile as gabapentin, scheduled (Class V) in the U.S.
What to avoid if you can: diphenhydramine (Benadryl, most PM formulations), zolpidem (Ambien) and the other Z-drugs for chronic use, and benzodiazepines. They induce sleep but flatten N3 — the exact stage you need to protect — and carry tolerance, cognitive, and falls risks that compound over time.
Why Melatonin Alone Rarely Fixes It — and Where Magnesium Glycinate Fits
Melatonin is a hormone, not a sedative. It is a timing signal that tells your brain “it is nighttime.” If your problem is that you cannot fall asleep at a reasonable clock time (delayed sleep phase, jet lag, shift work), melatonin 0.3–1 mg taken 2–4 hours before desired bedtime works beautifully. If your problem is that you do fall asleep but your sleep is fragmented, alpha-intruded, or apneic, melatonin does essentially nothing. This is the mismatch that leaves most fibromyalgia patients saying “I tried melatonin, it didn’t help.” It was the wrong tool.
Drugstore doses of 5–10 mg are too high. Supraphysiologic doses can cause vivid dreams, next-day fog, and receptor downregulation. Start at 0.3 mg if you can find it, or 1 mg. More is not better.
Magnesium glycinate at night is different and, for many fibromyalgia patients, genuinely useful. Magnesium is a cofactor for GABA activity and NMDA receptor regulation — both central to calming an overactive nervous system. Glycinate is a well-absorbed, non-laxative form (unlike magnesium oxide or citrate, which send you to the bathroom). A common dose is 200–400 mg elemental magnesium 30–60 minutes before bed. Many patients pair it with glycine itself (3 g) which independently lowers core body temperature and improves subjective sleep quality. Both are cheap, both are low-risk, and neither requires a prescription. See the nutrient gaps article for the full picture on why magnesium deficiency is so common in this population.
CBT-I: The Treatment Nobody Offers You
Cognitive behavioral therapy for insomnia (CBT-I) is the first-line treatment recommended by the American College of Physicians for chronic insomnia — ahead of any drug. It is also the treatment most fibromyalgia patients never hear about. It is not “therapy for sleep anxiety.” It is a structured 6–8 session protocol that retrains your brain’s association between bed and sleep using three core tools: stimulus control (bed is only for sleep), sleep restriction (compressing your time in bed to rebuild sleep pressure), and cognitive restructuring (unwinding the catastrophizing that keeps you awake).
CBT-I has stronger long-term evidence for chronic insomnia than any medication. In fibromyalgia cohorts specifically, randomized trials show improvements in sleep efficiency, pain, and fatigue that persist after the program ends — the opposite of what happens when you stop a sleep drug.
Access is the hard part. In-person CBT-I therapists are scarce. Free and low-cost digital alternatives that work almost as well include Sleepio, Somryst (FDA-cleared prescription app), and the VA’s CBT-i Coach app (free, public). If you have ever tried one drug after another for sleep, CBT-I is probably the highest-yield intervention you have not yet tried.
Common Traps: Alcohol, Late Caffeine, Doom-Scrolling
Alcohol. A glass of wine is the most common self-prescribed sleep aid. It works for the first 90 minutes — you fall asleep faster — and then it wrecks the rest of the night. Alcohol suppresses REM early and fragments N3 late. As it metabolizes around 2–3 a.m., it triggers a cortisol spike that wakes you. For fibromyalgia sleep in particular, the net effect is deeply negative. If you drink, finish at least 3–4 hours before bedtime and keep the total modest.
Caffeine. Caffeine has a half-life of 5–6 hours, meaning a 3 p.m. coffee still has a quarter of its dose circulating at 11 p.m. In slow metabolizers (a common genetic variant at CYP1A2), the half-life can exceed 8 hours. The rule of thumb is no caffeine after noon, period. If you depend on afternoon coffee to function, that is a flag that your sleep is broken — not a reason to keep drinking it.
Doom-scrolling. The phone-in-bed problem is not mainly about blue light. It is about cognitive and emotional arousal. News, social media, and email trigger the same alerting systems you are trying to quiet. Moving the phone out of the bedroom (or at least across the room, on a real alarm clock) is the single highest-yield behavioral change most people can make. If the idea of sleeping without your phone next to you generates anxiety, that is diagnostic — it is exactly the arousal keeping you out of N3.
Other traps worth naming: heavy late meals (raise core temperature, trigger reflux), intense evening exercise (raises cortisol; morning or early afternoon is better), and weekend sleep-ins longer than an hour past your weekday wake time (recreates a mini jet lag every Monday).
Key Research Papers
- Moldofsky H, Scarisbrick P, England R, Smythe H. Musculoskeletal symptoms and non-REM sleep disturbance in patients with “fibrositis syndrome” and healthy subjects. Psychosom Med. 1975;37(4):341–351.
- Roizenblatt S, Moldofsky H, Benedito-Silva AA, Tufik S. Alpha sleep characteristics in fibromyalgia. Arthritis Rheum. 2001;44(1):222–230. doi:10.1002/art.1780441102
- Diaz-Piedra C, Catena A, Sanchez AI, Miro E, Martinez MP, Buela-Casal G. Sleep disturbances in fibromyalgia syndrome: the role of clinical and polysomnographic variables. Sleep Med Rev. 2015;21:86–99.
- Bigatti SM, Hernandez AM, Cronan TA, Rand KL. Sleep disturbances in fibromyalgia syndrome: relationship to pain and depression. Arthritis Rheum. 2008.
- Wu YL, Chang LY, Lee HC, Fang SC, Tsai PS. Sleep disturbances in fibromyalgia: a meta-analysis of case-control studies. J Psychosom Res. 2017.
Live PubMed Searches
For further reading, the following PubMed topic searches return current peer-reviewed work on fibromyalgia sleep biology, sleep-disordered breathing overlap, and behavioral and pharmacologic interventions:
- Fibromyalgia and non-restorative sleep
- Alpha intrusion and EEG findings in fibromyalgia
- Fibromyalgia and obstructive sleep apnea overlap
- Fibromyalgia and upper airway resistance syndrome
- Fibromyalgia, restless legs, and periodic limb movements
- CBT-I in fibromyalgia patients
- Amitriptyline and cyclobenzaprine for fibromyalgia sleep
- Pregabalin and gabapentin effects on fibromyalgia sleep
- Growth hormone, IGF-1, and fibromyalgia
- HPA axis and cortisol rhythms in fibromyalgia
Connections
- Nutrient Gaps in Fibromyalgia
- Fibromyalgia Overview
- Insomnia
- Magnesium
- ACR 2016 Diagnostic Criteria
- Sleep Hygiene
- Fibromyalgia and ME/CFS Overlap
- Low-Dose Naltrexone for Fibromyalgia
- Central Sensitization Explained
- Small-Fiber Neuropathy Overlap
- Exercise Pacing and Graded Movement
- Chronic Fatigue Syndrome
- Insomnia (Symptoms)
- Magnesium Glycinate
- Fatigue
- Obstructive Sleep Apnea
- POTS
- Chronic Pain