Small-Fiber Neuropathy Overlap with Fibromyalgia
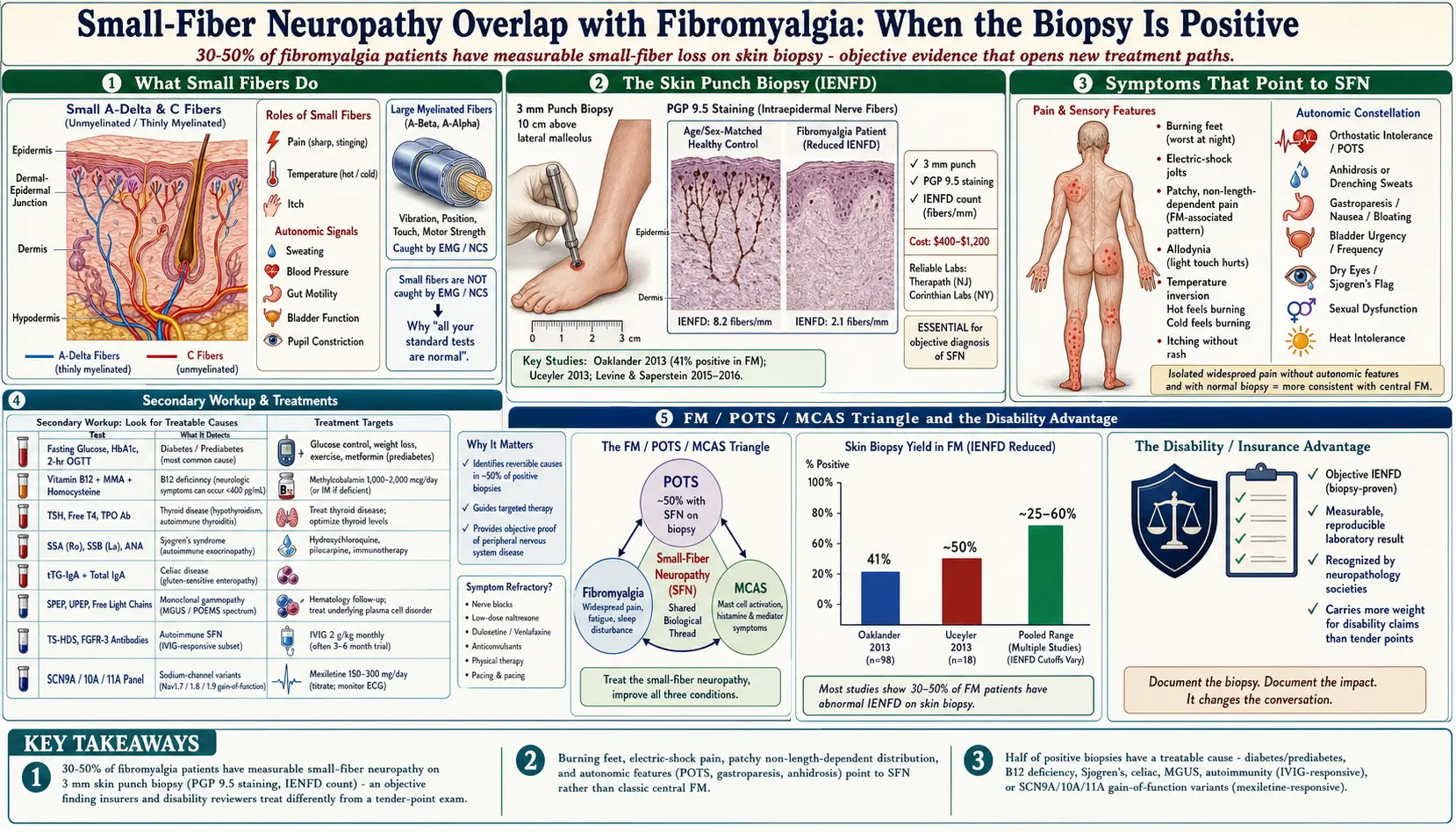
Table of Contents
- Why This Overlap Matters
- What Small-Fiber Neuropathy Actually Is
- The 30–50% Number — Where It Comes From
- Symptoms That Point to SFN Rather Than Classic Fibro
- The Autonomic Side — Often the Bigger Problem
- Testing — Skin Biopsy, QSART, and More
- Finding the Cause — The Secondary Workup
- Overlap with POTS and MCAS
- Treatment Implications
- When to Push for a Neurology Referral
- Insurance, Disability, and the Objective-Finding Advantage
- Key Research Papers
- Connections
- Featured Videos
Why This Overlap Matters
If you have fibromyalgia, you have probably been told, directly or indirectly, that there is nothing wrong with your nerves — that the pain is generated centrally, in the brain and spinal cord, and that imaging and lab tests will all come back normal. That is the textbook framing. It is also wrong for a significant minority of patients.
Starting with a 2013 study from Massachusetts General Hospital, researchers began systematically performing skin punch biopsies on patients who met full criteria for fibromyalgia. Roughly 30 to 50 percent of them turned out to have a measurable, objective nerve abnormality called small-fiber neuropathy (SFN) — not a central-pain mystery, but a structural loss of the thin nerve endings in the skin.
This matters for three concrete reasons:
- Objective evidence changes the conversation. A skin biopsy showing reduced nerve fiber density is not subjective. Insurers, disability reviewers, employers, and skeptical family members treat it differently than a tender-point count.
- It opens different treatments. SFN can be driven by autoimmunity, diabetes, B12 deficiency, or sodium-channel gene variants — and each of those has targeted therapy that standard fibromyalgia protocols ignore.
- It may explain why you have never fully responded to fibro drugs. Duloxetine and pregabalin were designed around central sensitization. If your pain is partly peripheral, the drug is only addressing half the picture.
This article walks through what SFN is, who should be tested, how testing works, what to do if the biopsy is positive, and how SFN connects to POTS, MCAS, and the rest of the fibromyalgia comorbidity cluster.
What Small-Fiber Neuropathy Actually Is
Your peripheral nerves come in two flavors. Large fibers are the thick, myelinated cables that carry vibration, position sense, and motor signals. They are what a neurologist tests with a tuning fork, reflex hammer, or standard nerve-conduction study (EMG/NCS). Small fibers are the thin, lightly myelinated (A-delta) and unmyelinated (C) fibers that carry pain, temperature, itch, and autonomic signals — the messages that run your sweating, blood-pressure regulation, gut motility, and bladder control.
When small fibers are damaged, the classic tests come back normal. Your reflexes are fine, your strength is fine, your EMG is fine. But the nerves carrying burning, stinging, electric-shock, and autonomic signals are either dying back from the tips (length-dependent SFN, starts in the feet) or dying patchily all over (non-length-dependent SFN, common in autoimmune and fibromyalgia-associated cases).
The damage is visible only with specialized testing. The reference standard is a 3 mm skin punch biopsy, usually taken from the distal leg, that is stained for a nerve marker called PGP 9.5 and examined under a microscope. A pathologist counts how many nerve fibers cross the dermal-epidermal junction per millimeter of skin. Below an age- and sex-adjusted cutoff, the diagnosis is SFN.
The 30–50% Number — Where It Comes From
Three landmark studies, all published around 2013, are the foundation of this field:
- Oaklander et al., 2013 (Pain). Anne Louise Oaklander's group at Mass General biopsied 27 patients with fibromyalgia and 30 matched controls. 41% of fibromyalgia patients had reduced intraepidermal nerve fiber density, versus 3% of controls.
- Üçeyler et al., 2013 (Brain). A German group studied 25 fibromyalgia patients with a combination of skin biopsy, quantitative sensory testing, and pain-related evoked potentials. They found reduced small-fiber function across multiple modalities, confirming the finding with a different technique.
- Levine and Saperstein, 2015 (Neurology, published 2016). A larger cohort biopsy study confirmed the 40–50% range and emphasized that many of these patients had treatable underlying causes.
Since then, dozens of follow-up studies have reported rates anywhere from 25% to over 60%, depending on how strictly fibromyalgia was defined and which biopsy cutoffs were used. The consensus rough estimate is one in three to one in two fibromyalgia patients. That is far too many to ignore.
Importantly, these are not different diseases layered on top of each other — the SFN often is the source of much of the pain being labeled fibromyalgia. The label is a description of symptoms, not a mechanism.
Symptoms That Point to SFN Rather Than Classic Fibro
Classic fibromyalgia pain is widespread, deep, aching, and migratory — it feels muscular. SFN pain has a different texture. If the following descriptions sound like your pain, push harder for a workup:
- Burning feet, especially at night. The sheets feel too hot. You kick your feet out from under the covers. The burning can extend up the calves.
- Electric-shock sensations. Sudden, brief, lightning-like jolts in the feet, hands, or randomly across the body.
- Pins and needles that are not positional. Unlike a foot that has fallen asleep, this tingling comes and goes without you sitting on a limb.
- Allodynia. Light touch — the seam of a sock, a bed sheet, a breeze — hurts. This is also seen in central sensitization, but in SFN it is often most intense distally.
- Pain that is patchy rather than widespread. A burning patch on the thigh, a stinging area on the back, numb fingertips. Non-length-dependent SFN (the kind most associated with fibromyalgia) produces these random distributions.
- Temperature intolerance. Hot showers feel painfully hot. Cold floors feel painfully cold. Your temperature sensation may also feel inverted — a cold object feels burning.
- Itching without a rash. Itch is a small-fiber signal.
The Autonomic Side — Often the Bigger Problem
Small fibers also run the autonomic nervous system — the unconscious wiring for blood pressure, heart rate, sweating, digestion, bladder, and pupils. When they are damaged, autonomic symptoms often dominate the clinical picture, and these are exactly the symptoms that most fibromyalgia patients describe as "weird extras" their doctors dismiss.
- Orthostatic intolerance. Lightheadedness, tunnel vision, or brain fog when standing. Heart rate that jumps 30+ beats per minute within 10 minutes of standing is diagnostic of POTS.
- Sweating abnormalities. Either not sweating enough (anhidrosis — you overheat easily, no sweat on the forehead in the sun) or drenching sweats in odd places and times.
- GI dysmotility. Gastroparesis (fullness after a few bites, nausea, bloating), chronic constipation, or SIBO that keeps relapsing. Many "IBS" patients in the fibromyalgia population actually have autonomic gut neuropathy.
- Bladder issues. Urinary frequency, urgency, incomplete emptying, or interstitial-cystitis-type pain.
- Dry eyes and dry mouth. Raises the question of Sjögren's syndrome (see workup below).
- Sexual dysfunction. Erectile dysfunction in men, reduced genital sensation or arousal in women, from autonomic nerve involvement.
- Heat intolerance. Getting sick from warm rooms, hot cars, or mild exertion — a combination of impaired sweating and blood-pressure regulation.
If you have fibromyalgia plus POTS plus IBS plus dry eyes plus temperature-regulation trouble, small-fiber neuropathy is the single hypothesis that ties all of it together.
Testing — Skin Biopsy, QSART, and More
Testing for SFN is specialized. Most primary care doctors and even many general neurologists will not order these. You usually need an academic medical center, a peripheral-neuropathy specialty clinic, or an autonomic-disorders center.
Skin punch biopsy (IENFD)
The diagnostic reference standard. A neurologist or dermatologist numbs a small spot, typically on the distal leg 10 cm above the lateral malleolus, and takes a 3 mm punch. A second sample is often taken higher up (thigh or trunk) to look for non-length-dependent patterns. The sample is fixed, sectioned, and stained for PGP 9.5. A trained pathologist counts the intraepidermal nerve fiber density (IENFD) per millimeter.
Results come back as fibers per mm with an age- and sex-matched normal range. Anything below the 5th percentile is diagnostic of SFN. The biopsy leaves a scar the size of a large pinhead. Cost ranges from $400 to $1,200, generally insurance-covered with the right neurology referral. Turnaround is 2–4 weeks. Labs that specialize in IENFD (such as Therapath or Corinthian) are more reliable than local hospital pathology.
QSART (Quantitative Sudomotor Axon Reflex Test)
Measures how well your sweat nerves respond to acetylcholine stimulation. Small capsules are strapped to the forearm, calf, foot, and thigh; a mild chemical current drives the drug into the skin and the machine records the sweat output. Reduced sweat response in a length-dependent pattern suggests small-fiber autonomic neuropathy. QSART is available at most autonomic centers (Mayo, Vanderbilt, Cleveland Clinic, and a growing number of regional programs).
Autonomic function testing panel
Usually done as a combined session: tilt-table test, Valsalva maneuver, deep breathing heart-rate variability, and QSART. This panel can objectively document POTS, orthostatic hypotension, and reduced heart-rate variability — all surrogates for autonomic small-fiber damage.
Corneal confocal microscopy
A newer, non-invasive option. A specialized eye microscope images the small nerves in your cornea. Reduced corneal nerve fiber length correlates with IENFD. Only a handful of U.S. centers offer it clinically, but it is painless, repeatable, and increasingly used for research and monitoring.
Quantitative sensory testing (QST)
Measures your threshold for detecting warm, cool, and vibratory stimuli. Abnormal temperature thresholds with normal vibration thresholds is a classic small-fiber pattern. QST is useful but does not distinguish central from peripheral mechanisms on its own — pair it with biopsy.
Finding the Cause — The Secondary Workup
If your biopsy is positive, the next step is not symptomatic treatment — it is figuring out why. Roughly half of SFN cases have an identifiable, sometimes reversible cause. A thorough workup includes:
- Diabetes and prediabetes. Fasting glucose, HbA1c, and ideally a 2-hour oral glucose tolerance test. Even impaired glucose tolerance (prediabetes) causes SFN, and standard HbA1c can miss it.
- B12 deficiency. Serum B12, methylmalonic acid, and homocysteine. Anyone on long-term metformin, proton pump inhibitors, or a vegan diet is at risk. See Vitamin B12.
- Thyroid disease. TSH, free T4, and in women TPO antibodies. Both hypothyroidism and Hashimoto's have been associated with SFN. See Hashimoto's Thyroiditis.
- Sjögren's syndrome. SSA (Ro) and SSB (La) antibodies, ANA, and a lip biopsy if symptoms of dry eyes/dry mouth are present. Seronegative Sjögren's is common, so a normal antibody panel does not rule it out.
- Celiac disease. Tissue transglutaminase (tTG-IgA) with total IgA. Celiac can cause SFN independent of GI symptoms.
- Monoclonal gammopathy. SPEP, UPEP, and serum free light chains. An MGUS (monoclonal gammopathy of undetermined significance) found on SFN workup can rarely signal an early plasma-cell disorder requiring hematology follow-up.
- Other autoimmune. ANA, rheumatoid factor, anti-CCP, complement levels. TS-HDS and FGFR-3 antibodies are newer markers specifically linked to autoimmune SFN; they are available through a few reference labs.
- Sodium channel genes. Gain-of-function mutations in SCN9A, SCN10A, and SCN11A (encoding the Nav1.7, Nav1.8, and Nav1.9 sodium channels) cause familial SFN with burning pain. Panel testing is available through neurogenetics labs and is worth considering in patients with a family history of unexplained pain, early-onset burning feet, or non-length-dependent patterns.
- Infections and toxins. HIV, hepatitis C, Lyme disease (in endemic areas), and heavy metals round out the list.
- Alcohol. Chronic alcohol use causes SFN directly. An honest conversation about intake is part of the workup.
A basic workup can be ordered by primary care; the autoimmune and genetic pieces usually require neurology or rheumatology. Many patients with fibromyalgia-associated SFN end up with a diagnosis of idiopathic SFN (no cause found) or presumed autoimmune SFN — a category that is increasingly treated empirically with immune therapy.
Overlap with POTS and MCAS
Three diagnoses sit in a tight triangle: fibromyalgia, postural orthostatic tachycardia syndrome (POTS), and mast cell activation syndrome (MCAS). Small-fiber neuropathy is the biological link between them.
- POTS. Roughly half of POTS patients have evidence of small-fiber neuropathy on biopsy or QSART. The neuropathic subtype of POTS is driven by impaired small-fiber sympathetic control of peripheral blood vessels — blood pools in the legs, so the heart races to compensate. See POTS for the full picture.
- MCAS. Mast cells and small nerve fibers sit millimeters apart in skin and gut and talk constantly. Mast-cell mediators (tryptase, histamine, prostaglandin D2) can sensitize and damage small fibers; in turn, damaged small fibers can trigger mast cell degranulation. Flushing, itching, abdominal cramps, and food reactions in a fibromyalgia patient are worth an MCAS workup alongside SFN.
- Hypermobility. Patients with hypermobile Ehlers-Danlos or hypermobility spectrum disorders also show elevated rates of SFN on biopsy. The triad of hypermobility + POTS + MCAS, long recognized clinically, has small-fiber neuropathy as a shared thread.
If you check off two or three of these at once, a skin biopsy is not a fishing expedition — it is the single most informative next test.
Treatment Implications
Once SFN is documented, treatment has two layers: treat the underlying cause if one was found, and manage the pain and autonomic symptoms while you do.
Cause-directed therapy
- Diabetes/prediabetes: aggressive glucose control, ideally with a low-carbohydrate diet, weight loss, and metformin or GLP-1 agonists. Small-fiber density can actually regenerate when glucose is normalized.
- B12 deficiency: oral or injectable methylcobalamin, usually 1 mg daily or weekly injections until levels normalize.
- Celiac: strict gluten-free diet.
- Autoimmune / Sjögren's-associated SFN: this is where IVIG (intravenous immunoglobulin) comes in. Open-label studies and case series report meaningful pain reduction and partial IENFD recovery in a subset of patients, typically at 2 g/kg per month for 3–6 months. Access is controlled by insurance and usually requires failed first-line drugs plus documented SFN plus a positive autoimmune marker. Other immune options include rituximab and plasmapheresis in selected cases.
- SCN9A/10A/11A variants: mexiletine, an oral sodium-channel blocker, can dramatically reduce pain in patients with gain-of-function mutations. Requires baseline ECG and cardiology clearance.
Symptomatic therapy
- Topical agents. Lidocaine 5% patches (up to three at a time for 12 hours on, 12 hours off) for focal burning. Capsaicin 8% patches (Qutenza), applied in-clinic, deplete substance P and can give 3 months of pain reduction per application. Compounded topical ketamine, amitriptyline, and gabapentin creams are used off-label.
- Gabapentinoids. Gabapentin (titrated to 900–3600 mg/day in divided doses) or pregabalin (150–450 mg/day). Same drugs used in fibromyalgia, but they address peripheral neuropathic pain directly.
- SNRIs. Duloxetine 30–60 mg daily has evidence in diabetic SFN and is already a first-line fibromyalgia drug, which is convenient.
- Tricyclics. Low-dose amitriptyline or nortriptyline (10–50 mg at bedtime) help pain and sleep, though anticholinergic side effects are worse in patients with autonomic dysfunction — watch for constipation, dry mouth, and orthostatic worsening.
- Alpha-lipoic acid. 600 mg daily has modest evidence in diabetic SFN; reasonable to try in idiopathic cases.
- Autonomic-targeted care. Salt and fluid loading, compression stockings, midodrine, or ivabradine for the POTS component. Low-dose naltrexone (LDN, 1.5–4.5 mg at bedtime) is increasingly used for the overlapping pain and immune picture.
When to Push for a Neurology Referral
You should ask your primary care doctor — and insist, politely, if needed — for a neurology referral for SFN workup if any of the following apply:
- Your fibromyalgia pain has a burning, electric, or stinging quality, especially in the feet.
- You have unexplained autonomic symptoms (orthostatic intolerance, GI dysmotility, sweating abnormalities, unexplained palpitations).
- You have dry eyes and dry mouth and have never been evaluated for Sjögren's.
- A first-line fibromyalgia drug (duloxetine or pregabalin) has failed or given only partial benefit.
- You are pursuing disability or long-term leave and need objective evidence.
- You have a family history of unexplained chronic pain or burning feet.
Ask specifically for a neurologist who does skin biopsy for intraepidermal nerve fiber density, or for a peripheral-nerve or autonomic subspecialty clinic. A generic neurology referral may end with a normal EMG and a shrug — EMG does not test small fibers. If the local wait is long, teaching hospitals and academic centers usually have shorter waits for subspecialty clinics than for general neurology.
Insurance, Disability, and the Objective-Finding Advantage
One of the most quietly life-altering effects of an SFN diagnosis is administrative. Fibromyalgia is classed by many insurers and disability reviewers as a subjective condition — you describe pain, a doctor records tender points, nothing shows on imaging or labs. Claims get denied or sent to review.
An IENFD-proven SFN is different. It is an ICD-10-coded neurological disorder (G60.8 or G90.09, depending on autonomic involvement) with a measurable pathology report. Short-term and long-term disability insurers, Social Security Disability examiners, and health insurers authorizing IVIG or specialty drugs respond measurably better to a biopsy result than to a fibromyalgia letter alone.
This is not a reason to pursue testing if you do not have symptoms that warrant it. But if you have been living under-treated because your pain is labeled "just fibromyalgia," and the symptom pattern above fits, the workup can change not only your treatment but your financial stability.
Key Research Papers
- Oaklander AL, Herzog ZD, Downs HM, Klein MM. Objective evidence that small-fiber polyneuropathy underlies some illnesses currently labeled as fibromyalgia. Pain. 2013;154(11):2310–2316.
- Üçeyler N, Zeller D, Kahn AK, et al. Small fibre pathology in patients with fibromyalgia syndrome. Brain. 2013;136(Pt 6):1857–1867.
- Levine TD, Saperstein DS. Routine use of punch biopsy to diagnose small fiber neuropathy in fibromyalgia patients. Muscle & Nerve. 2015/2016.
- Faber CG, Hoeijmakers JG, Ahn HS, et al. Gain of function Nav1.7 mutations in idiopathic small fiber neuropathy. Ann Neurol. 2012.
- Gemignani F, Bellanova MF, Saccani E, Pavesi G. Non-length-dependent small fiber neuropathy: a prospective case series. J Peripher Nerv Syst. 2019.
Live PubMed Searches
For further reading, the following PubMed topic searches return current peer-reviewed work on the fibromyalgia–SFN overlap, testing, and treatment:
- Small-fiber neuropathy and fibromyalgia
- Intraepidermal nerve fiber density and skin biopsy
- QSART and autonomic small-fiber testing
- Corneal confocal microscopy in small-fiber neuropathy
- IVIG in autoimmune small-fiber neuropathy
- Sodium channel gene variants in small-fiber neuropathy
- POTS and small-fiber neuropathy
- Sjögren's syndrome and small-fiber neuropathy
- Mexiletine for sodium-channel small-fiber neuropathy
Connections
- POTS
- Hashimoto's Thyroiditis
- Vitamin B12
- Fibromyalgia Overview
- Diabetes
- Chronic Pain
- Fibromyalgia and ME/CFS Overlap
- Central Sensitization Explained
- Peripheral Neuropathy
- Thyroid Disorders
- MCAS
- ACR 2016 Diagnostic Criteria
- Exercise Pacing and Graded Movement
- Low-Dose Naltrexone for Fibromyalgia
- Nutrient Gaps in Fibromyalgia
- Homocysteine
- SIBO
- Vitamin B12 Test