Vitamin D3 and Cancer Prevention
The relationship between vitamin D and cancer was first proposed by Cedric and Frank Garland in 1980, based on the observation that colon cancer mortality in the United States followed a striking geographic gradient, with highest rates in the Northeast (lowest sunlight) and lowest rates in the South and Southwest. Since that seminal ecological observation, extensive laboratory, epidemiological, and clinical trial evidence has accumulated supporting a role for vitamin D in cancer prevention, particularly through the regulation of cell proliferation, differentiation, apoptosis, and angiogenesis. The landmark VITAL trial of nearly 26,000 U.S. adults, while not showing a reduction in overall cancer incidence with 2,000 IU/day of vitamin D3, did demonstrate a meaningful 25% reduction in cancer mortality when the first two years of follow-up were excluded — suggesting that vitamin D's strongest anticancer effect lies in slowing progression rather than preventing initiation.
Table of Contents
- Key Health Benefits at a Glance
- VDR Gene Regulation: Anti-Cancer Mechanisms
- Colorectal Cancer: The Strongest Evidence
- Breast Cancer
- Prostate Cancer
- Pancreatic Cancer
- Cancer Mortality Reduction
- Optimal 25(OH)D Levels for Cancer Prevention
- VITAL Trial Cancer Results
- Lappe Trial
- Extrarenal Calcitriol Production in Tissues
- Clinical Recommendations
- Research Papers and References
- Connections
- Featured Videos
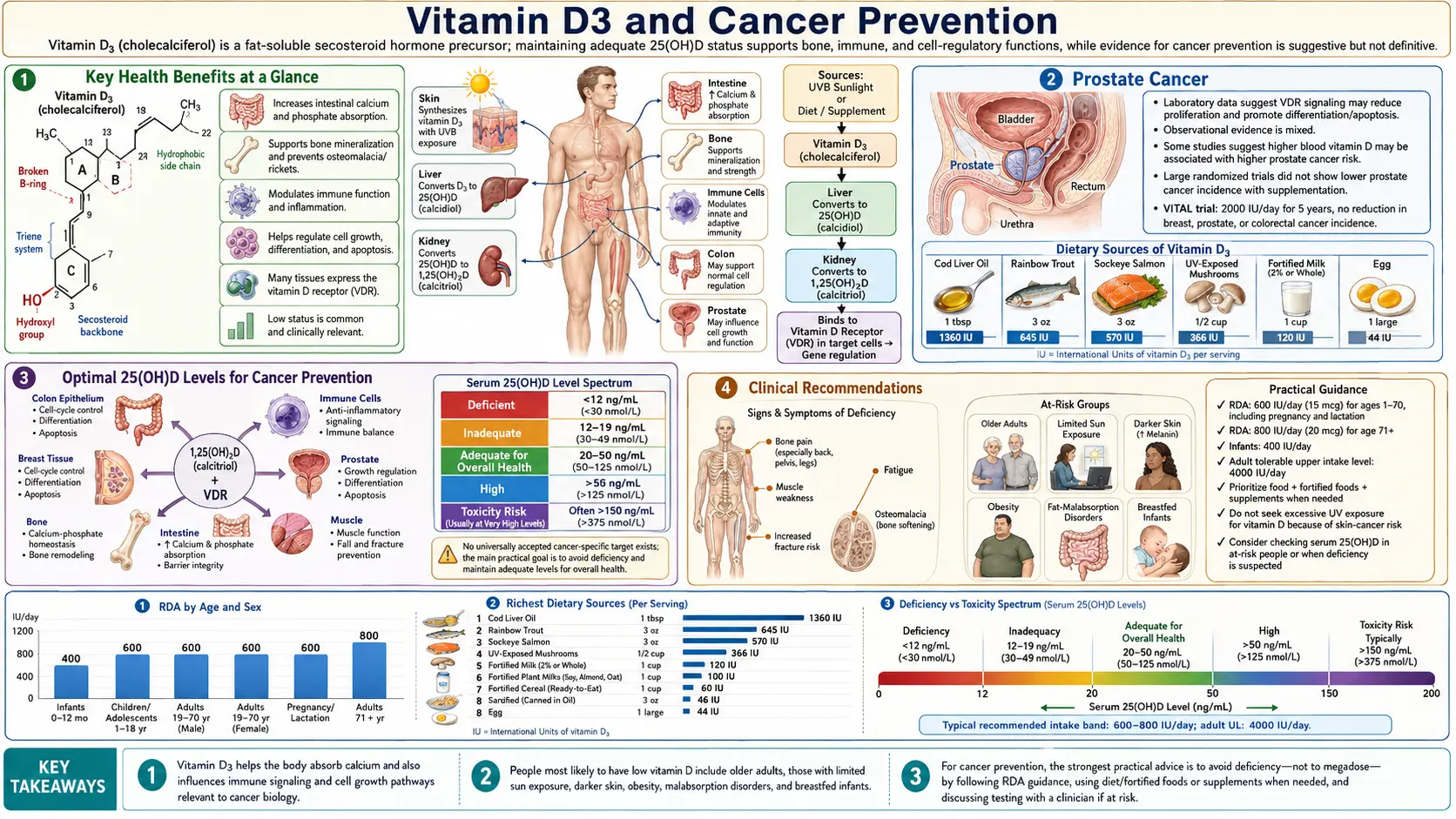
Key Health Benefits at a Glance
The following is a high-level summary of the evidence-backed cancer-prevention benefits of adequate vitamin D3 status. Each is explored in more depth below, and the supporting studies are linked in the Research Papers section.
- Reduces cancer mortality by ~13–25% – The 2019 VITAL trial (Manson et al.) found a 25% reduction in cancer deaths in the vitamin D arm when the first two years were excluded; meta-analyses support an overall 13% mortality reduction with supplementation.
- Lowers colorectal cancer risk – Pooled prospective cohort data link each 10 ng/mL rise in 25(OH)D with a ~19% risk reduction; levels above 33 ng/mL carry a 33% lower colorectal cancer risk.
- Reduces advanced/metastatic cancer – VITAL showed a 17% reduction in metastatic or fatal cancer overall and a 38% reduction in normal-BMI participants, consistent with anti-invasion and anti-angiogenesis mechanisms.
- Induces cancer cell apoptosis – Calcitriol upregulates BAX/BAK and downregulates BCL-2/BCL-XL, restoring programmed cell death in pre-malignant and malignant cells.
- Inhibits angiogenesis – Calcitriol suppresses VEGF and upregulates thrombospondin-1, limiting the tumor neovascularization required for growth beyond a few millimeters.
- Promotes differentiation – Calcitriol drives immature proliferating cells toward mature, specialized phenotypes with reduced division capacity — the same principle behind calcipotriol therapy for psoriasis.
- Suppresses Wnt/beta-catenin – In colonocytes, calcitriol dampens the Wnt pathway activated by APC mutations in most colorectal cancers.
- Remodels pancreatic tumor stroma – VDR activation in pancreatic stellate cells (Sherman et al.) returns them to quiescence, improving chemotherapy drug delivery in preclinical models.
VDR Gene Regulation: Anti-Cancer Mechanisms
The vitamin D receptor (VDR) is expressed in most human tissues, including those where the most common cancers arise. When activated by calcitriol, the VDR-RXR heterodimer regulates the expression of genes involved in several hallmarks of cancer.
- Cell Proliferation Control – Calcitriol induces cell cycle arrest, primarily at the G0/G1 checkpoint, by upregulating cyclin-dependent kinase inhibitors (p21 and p27) and downregulating cyclins (cyclin D1) and cyclin-dependent kinases (CDK2, CDK4, CDK6). These actions slow or halt the uncontrolled cell division that characterizes cancer. In addition, calcitriol inhibits the expression of c-Myc, a proto-oncogene that drives proliferation in many cancer types.
- Cellular Differentiation – Calcitriol promotes the differentiation of many cell types, pushing immature, rapidly dividing cells toward a mature, functionally specialized phenotype with reduced proliferative capacity. This pro-differentiation effect has been demonstrated in colonic epithelial cells, breast cells, prostate cells, and myeloid leukemia cells. The therapeutic application of the vitamin D analogue calcipotriol in psoriasis (a hyperproliferative skin disorder) is a clinical example of this principle.
- Apoptosis Induction – Calcitriol activates both intrinsic and extrinsic apoptotic pathways in cancer cells. It upregulates pro-apoptotic proteins (BAX, BAK) and downregulates anti-apoptotic proteins (BCL-2, BCL-XL). Calcitriol also sensitizes cancer cells to other apoptotic stimuli, including chemotherapy agents, through caspase activation and mitochondrial membrane permeabilization. The ability to restore apoptotic potential in cancer cells that have evaded programmed cell death is one of the most important anti-cancer properties of vitamin D.
- Angiogenesis Inhibition – Tumors require new blood vessel formation (angiogenesis) to grow beyond a few millimeters in diameter. Calcitriol inhibits angiogenesis by suppressing the expression of vascular endothelial growth factor (VEGF) and its receptors in tumor cells and by directly inhibiting endothelial cell proliferation and migration. Calcitriol also upregulates thrombospondin-1, a potent endogenous angiogenesis inhibitor.
- Invasion and Metastasis Suppression – Calcitriol upregulates E-cadherin, a cell adhesion molecule that maintains epithelial cell-cell contacts and whose loss is associated with epithelial-to-mesenchymal transition (EMT) and metastatic potential. Calcitriol also inhibits matrix metalloproteinases (MMPs) that degrade the extracellular matrix, reducing tumor invasiveness. Additionally, vitamin D suppresses the Wnt/beta-catenin signaling pathway, which drives both proliferation and invasion in colorectal and other cancers.
- DNA Repair – Emerging evidence suggests that calcitriol may enhance DNA damage repair mechanisms, reducing the accumulation of mutations that drive carcinogenesis. This effect has been demonstrated in colonocytes exposed to oxidative stress and may contribute to the cancer-preventive effect independent of proliferation control.
Colorectal Cancer: The Strongest Evidence
- Ecological Studies – The Garland brothers' original observation of a latitude gradient in colon cancer mortality has been replicated in multiple countries and time periods. Regions with greater UVB exposure consistently show lower colorectal cancer incidence and mortality.
- Prospective Cohort Studies – Multiple large prospective studies have found significant inverse associations between 25(OH)D levels and colorectal cancer risk. A pooled analysis of 17 cohorts by the Vitamin D Pooling Project found that participants with 25(OH)D levels above 33 ng/mL had a 33 percent lower risk of colorectal cancer compared to those with levels below 12 ng/mL. The dose-response relationship was approximately linear, with each 10 ng/mL increase in 25(OH)D associated with a 19 percent reduction in risk.
- Mechanistic Support – The colon is one of the tissues with the highest VDR expression and local CYP27B1 activity. Calcitriol suppresses the Wnt/beta-catenin pathway, which is activated by APC gene mutations in the majority of colorectal cancers. This provides a compelling mechanistic link between vitamin D signaling and colorectal carcinogenesis. Vitamin D also promotes E-cadherin expression in colonocytes and reduces the pro-proliferative effects of secondary bile acids.
- Clinical Implications – Based on the strength and consistency of the colorectal cancer evidence, several expert panels have recommended maintaining 25(OH)D levels above 30 ng/mL for colorectal cancer risk reduction. Some researchers advocate for levels above 40 ng/mL based on the dose-response data.
Breast Cancer
- Epidemiological Evidence – Higher 25(OH)D levels are consistently associated with lower breast cancer risk in observational studies, particularly for premenopausal breast cancer. A meta-analysis by Garland et al. estimated that maintaining 25(OH)D levels above 47 ng/mL was associated with a 50 percent reduction in breast cancer risk compared to levels below 13 ng/mL.
- Tumor Biology – VDR is expressed in normal breast tissue and in the majority of breast tumors. Calcitriol inhibits proliferation and induces apoptosis in breast cancer cell lines, and animal studies show that vitamin D deficiency accelerates mammary tumor development. VDR expression in breast tumors is associated with better prognosis, smaller tumor size, and lower grade.
- Breast Density – Higher vitamin D levels are associated with lower mammographic breast density, an established risk factor for breast cancer. This relationship may represent one mechanism through which vitamin D reduces breast cancer risk.
- Survival – Among women diagnosed with breast cancer, higher 25(OH)D levels at diagnosis are associated with improved overall survival and lower rates of recurrence in multiple observational studies. This prognostic association persists after adjustment for stage, grade, and treatment.
Prostate Cancer
- Mixed Epidemiological Data – The association between vitamin D and prostate cancer is less consistent than for colorectal cancer. Some studies show an inverse association (higher vitamin D, lower risk), while others show no association or even a U-shaped relationship with increased risk at both very low and very high 25(OH)D levels.
- Laboratory Evidence – In contrast to the mixed epidemiological data, laboratory evidence is compelling. Prostate epithelial cells express VDR and CYP27B1, and calcitriol consistently inhibits prostate cancer cell proliferation, induces apoptosis, and reduces invasiveness in cell culture and animal models. The discrepancy between laboratory and epidemiological findings may reflect the complexity of prostate cancer biology, including the influence of androgen signaling on VDR expression.
- Clinical Applications – High-dose calcitriol in combination with chemotherapy (docetaxel) has been studied in advanced prostate cancer, with some trials showing improved PSA response rates. However, hypercalcemia limits the therapeutic window of calcitriol, and vitamin D analogues with reduced calcemic activity are under development for oncology applications.
Pancreatic Cancer
- Epidemiological Associations – Several prospective studies have found inverse associations between 25(OH)D levels and pancreatic cancer risk. A pooled analysis found that levels above 32 ng/mL were associated with a 45 percent reduction in pancreatic cancer risk compared to levels below 16 ng/mL.
- Stromal VDR Targeting – Particularly exciting research by Sherman and colleagues has demonstrated that VDR activation in pancreatic stellate cells (the cells that create the dense fibrotic stroma characteristic of pancreatic cancer) can reprogram these cells from an activated, tumor-promoting state to a quiescent state. This stromal remodeling enhances chemotherapy drug delivery and improves treatment efficacy in preclinical models.
- Calcipotriol Combination Therapy – Based on the stromal VDR data, clinical trials are investigating the combination of the vitamin D analogue calcipotriol with gemcitabine (standard pancreatic cancer chemotherapy) to improve treatment outcomes. This represents one of the most promising translational applications of vitamin D in oncology.
Cancer Mortality Reduction
- Meta-Analysis Evidence – While randomized trials have generally not shown reduced cancer incidence with vitamin D supplementation, meta-analyses of trial data have consistently found reduced cancer mortality. A 2019 meta-analysis by Keum et al. of randomized trials found a 13 percent reduction in cancer mortality with vitamin D supplementation (RR 0.87, 95% CI 0.79 to 0.96), despite no significant effect on cancer incidence. The Chowdhury et al. (2014) meta-analysis also found an inverse relationship between 25(OH)D concentration and cause-specific mortality including cancer.
- Interpretation – The dissociation between incidence and mortality effects suggests that vitamin D may be more important in slowing cancer progression, reducing metastatic potential, and improving treatment responsiveness than in preventing the initial malignant transformation. This is consistent with vitamin D's effects on differentiation, apoptosis, angiogenesis, and immune surveillance against established tumors.
- Clinical Relevance – If vitamin D supplementation reduces cancer mortality by 13 percent, this would translate to tens of thousands of avoided cancer deaths annually in the United States alone. This population-level impact, combined with the safety and low cost of vitamin D3 supplementation, makes this one of the most important public health implications of vitamin D research.
Optimal 25(OH)D Levels for Cancer Prevention
- Minimum Threshold – Epidemiological evidence suggests that cancer risk reduction begins at 25(OH)D levels above 20 ng/mL (50 nmol/L), with progressively greater protection at higher levels.
- Target Range: 40 to 60 ng/mL – Based on dose-response analyses of prospective cohort data, many cancer researchers and integrative oncologists recommend maintaining 25(OH)D levels between 40 and 60 ng/mL (100 to 150 nmol/L) for optimal cancer prevention. The Grassroots Health D*Action project, a large prospective cohort study, found that participants maintaining levels above 40 ng/mL had a 67 percent lower cancer risk compared to those with levels below 20 ng/mL.
- Dose Required – To achieve 25(OH)D levels of 40 to 60 ng/mL, most adults require 4,000 to 6,000 IU of vitamin D3 daily, depending on body weight, baseline levels, and sun exposure. Obese individuals may require 2 to 3 times higher doses due to vitamin D sequestration in adipose tissue.
- Safety at These Levels – 25(OH)D levels of 40 to 60 ng/mL are well below the toxicity threshold (typically above 150 ng/mL) and have not been associated with hypercalcemia or other adverse effects in clinical studies. The IOM's tolerable upper intake of 4,000 IU daily is considered conservative by many vitamin D researchers.
VITAL Trial Cancer Results
- Primary Cancer Endpoint – The VITAL trial (25,871 participants, 2,000 IU vitamin D3 daily, median follow-up 5.3 years) did not find a statistically significant reduction in total invasive cancer incidence in the vitamin D group compared to placebo (HR 0.96, 95% CI 0.88 to 1.06).
- Cancer Mortality – However, when excluding the first two years of follow-up (to allow a latency period for vitamin D to exert anti-cancer effects), the vitamin D group showed a 25 percent reduction in cancer mortality (HR 0.75, 95% CI 0.59 to 0.96). This time-dependent pattern is biologically plausible, as the effects of vitamin D on tumor biology would require time to manifest in mortality outcomes.
- BMI Interaction – A significant interaction with BMI was observed. In participants with normal BMI (under 25), vitamin D supplementation reduced cancer incidence by 24 percent. In overweight and obese participants, no benefit was observed. This finding is attributed to the dilution of 2,000 IU daily across larger body mass, resulting in smaller increments in 25(OH)D levels in heavier individuals.
- Metastatic Cancer – A secondary analysis found that vitamin D supplementation reduced the incidence of advanced (metastatic or fatal) cancer by 17 percent overall, and by 38 percent in the normal-BMI subgroup. This reduction in metastatic cancer is consistent with vitamin D's effects on tumor invasion, angiogenesis, and immune surveillance.
Lappe Trial
- Study Design – The Lappe et al. trial randomized 2,303 healthy postmenopausal women in Nebraska to vitamin D3 (2,000 IU daily) plus calcium (1,500 mg daily) or placebo for 4 years, with cancer incidence as the primary outcome.
- Results – The intervention group showed a non-significant 30 percent reduction in total cancer incidence (HR 0.70, 95% CI 0.47 to 1.02, p = 0.06). While not reaching statistical significance in the intention-to-treat analysis, the direction and magnitude of the effect were consistent with a meaningful cancer-preventive effect.
- 25(OH)D Levels Achieved – The supplementation group achieved mean 25(OH)D levels of approximately 44 ng/mL, well within the proposed optimal range. The control group had mean levels of approximately 32 ng/mL, which was higher than expected and may have attenuated the between-group difference, reducing the power to detect a significant effect.
- Earlier Lappe Trial (2007) – A previous trial by Lappe et al. with 1,179 postmenopausal women using vitamin D3 (1,100 IU daily) plus calcium did find a significant 60 percent reduction in all-cancer risk over 4 years (RR 0.40, p less than 0.01). The discrepancy between the two trials may reflect differences in baseline vitamin D status, statistical power, and the specific cancer types that occurred.
Extrarenal Calcitriol Production in Tissues
- Local Synthesis – Many tissues outside the kidney express CYP27B1 (1-alpha-hydroxylase) and can convert circulating 25(OH)D to active calcitriol locally. These include colonic epithelial cells, breast cells, prostate cells, pancreatic cells, skin keratinocytes, and immune cells within the tumor microenvironment. This local production is critical because it allows tissue-specific regulation of cell growth and differentiation independently of systemic calcium homeostasis.
- Substrate Dependence – Unlike renal calcitriol production (which is tightly regulated by PTH, calcium, and FGF23), extrarenal calcitriol synthesis is primarily substrate-dependent, meaning it is directly proportional to the circulating concentration of 25(OH)D. This explains why maintaining adequate 25(OH)D levels is important for cancer prevention: higher circulating 25(OH)D provides more substrate for local calcitriol production in tissues at risk for malignant transformation.
- Loss in Cancer – As tumors progress, they often downregulate CYP27B1 and upregulate CYP24A1 (the enzyme that degrades calcitriol), effectively disabling the local vitamin D-mediated growth control. This loss of local vitamin D signaling may represent a selective advantage for tumor cells that escape growth inhibition. Restoring vitamin D signaling through pharmacological means (high-dose calcitriol or analogues) is an active area of therapeutic research.
- Tumor Microenvironment – Immune cells within the tumor microenvironment (tumor-associated macrophages, tumor-infiltrating lymphocytes) also produce calcitriol locally, which may influence anti-tumor immune surveillance. Adequate vitamin D status may therefore support immune-mediated tumor control in addition to direct effects on cancer cell biology.
Clinical Recommendations
- General Population – While definitive randomized trial evidence for cancer prevention is still emerging, the combined weight of ecological, observational, mechanistic, and trial data supports maintaining 25(OH)D levels of at least 30 ng/mL and ideally 40 to 60 ng/mL. This can typically be achieved with 2,000 to 4,000 IU of vitamin D3 daily for most adults.
- High-Risk Individuals – Those with a family history of colorectal, breast, or prostate cancer, or with pre-malignant conditions (colorectal adenomas, ductal carcinoma in situ), may wish to target the higher end of the recommended range (50 to 60 ng/mL) in consultation with their healthcare provider.
- Cancer Survivors – Maintaining adequate vitamin D status during and after cancer treatment is recommended based on the mortality data. Vitamin D deficiency is common in cancer patients due to reduced outdoor activity, chemotherapy effects, and other factors. Supplementation to maintain levels above 30 ng/mL is supported by multiple oncology guidelines.
- Monitoring – Regular 25(OH)D testing is recommended for individuals supplementing at doses above 2,000 IU daily or for those with risk factors for deficiency (obesity, dark skin, limited sun exposure, malabsorption). Testing ensures that target levels are achieved without oversupplementation.
- Vitamin D3 vs. D2 – Vitamin D3 (cholecalciferol) is preferred over D2 (ergocalciferol) for supplementation due to its superior potency in raising and maintaining 25(OH)D levels. D3 has approximately 87 percent greater potency than D2 and a longer duration of action, making it the form of choice for cancer prevention strategies.
- Comprehensive Approach – Vitamin D supplementation should be viewed as one component of a comprehensive cancer prevention strategy that includes a healthy diet rich in fruits, vegetables, and fiber; regular physical activity; maintaining a healthy body weight; limiting alcohol consumption; avoiding tobacco; and participating in age-appropriate cancer screening programs.
This content is provided for informational purposes only and does not constitute medical advice. Vitamin D supplementation is not a substitute for cancer screening, proven cancer therapy, or the guidance of an oncologist. Consult a qualified healthcare provider before beginning any supplementation regimen.
Research Papers and References
The following are landmark and frequently cited research papers underpinning the claims on this page. Links resolve to the publisher DOI or PubMed record.
Foundational Reviews
- Holick MF. Vitamin D deficiency. New England Journal of Medicine. 2007;357(3):266-281.
- Bikle DD. Vitamin D metabolism, mechanism of action, and clinical applications. Chemistry & Biology. 2014;21(3):319-329.
Major Cancer Prevention Trials
- Manson JE, Cook NR, Lee IM, et al. Vitamin D supplements and prevention of cancer and cardiovascular disease (VITAL). New England Journal of Medicine. 2019;380(1):33-44.
- Chowdhury R, Kunutsor S, Vitezova A, et al. Vitamin D and risk of cause specific death: systematic review and meta-analysis. BMJ. 2014;348:g1903.
- Lappe JM et al. Vitamin D and calcium supplementation and cancer risk in postmenopausal women. PubMed search.
- Keum N et al. Vitamin D supplementation and total cancer incidence and mortality: a meta-analysis of RCTs. PubMed search.
Colorectal, Breast, and Prostate Cancer Epidemiology
- Vitamin D Pooling Project — 25(OH)D and colorectal cancer risk (PubMed search).
- Garland CF et al. Vitamin D and breast cancer meta-analysis (PubMed search).
- Vitamin D and prostate cancer risk (PubMed search).
Mechanistic and Translational Research
- Sherman MH et al. Vitamin D receptor in pancreatic stellate cells: stromal reprogramming (PubMed search).
- Calcitriol, VDR signaling, and apoptosis in cancer cells (PubMed search).
External Authoritative Resources
- NIH Office of Dietary Supplements — Vitamin D Fact Sheet for Health Professionals
- Linus Pauling Institute — Vitamin D
- Harvard T.H. Chan School of Public Health — The Nutrition Source: Vitamin D
Connections
- All Vitamins
- Vitamin D3
- Cancer
- Calcium
- Vitamin D3 and Immune System
- Vitamin D3 and Bone Health
- Magnesium
- Vitamin D Test
- Vitamin K2 and Arterial Calcification
- Selenium
- Vitamin C
- Vitamin E
- Vitamin A
- Obesity
- Cardiovascular Disease