Osteoporosis
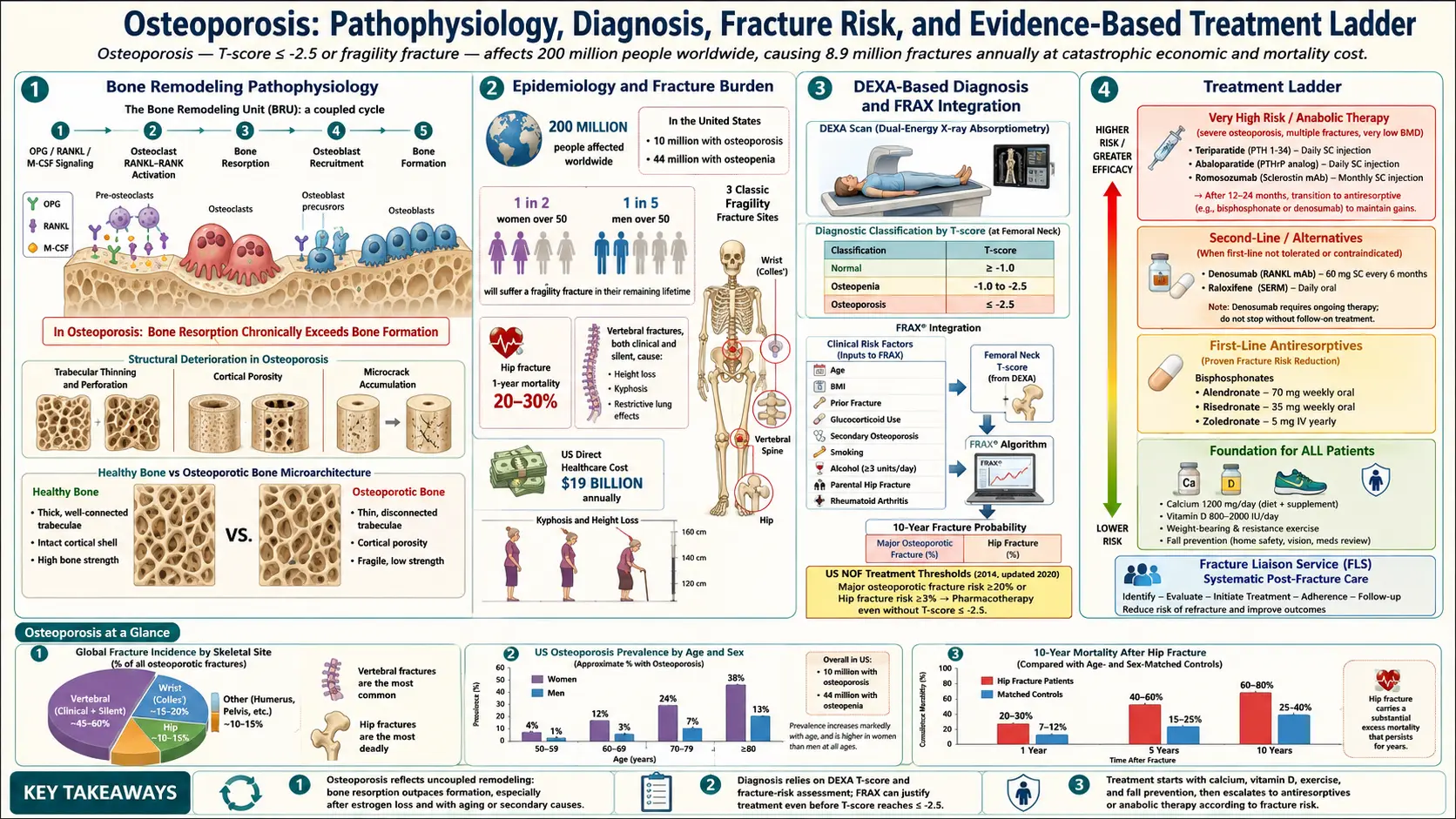
Osteoporosis is a disease in which bone becomes both thinner and structurally worse, until it breaks under forces that should never have broken it. It causes no pain and no symptoms of its own. Most people find out they have it the way you find out a bridge was corroded — when something collapses. The encouraging part is that it is easy to detect with a painless scan, and the treatments that exist are genuinely effective: the best of them cut spine-fracture risk by roughly two-thirds, and one of them has been shown to reduce death after a hip fracture.
Deep-Dive Articles
The articles below expand this overview into DEXA, FRAX, specific medications, fracture prevention, and special populations. Written for patients, with real research citations.
DEXA Scan: T-score & Z-score
How DEXA measures bone density, what T-scores and Z-scores mean, trabecular bone score, and when to repeat.
FRAX & Treatment Thresholds
10-year fracture risk scoring, NOF/Endocrine Society thresholds for therapy, and how race/ethnicity modifiers fit.
Bisphosphonates
Oral vs IV bisphosphonates, dosing, drug holiday timing, jaw osteonecrosis and atypical femur fracture risks.
Denosumab, Romosozumab & Teriparatide
Anabolic vs antiresorptive therapy, ARCH/FRAME trials, rebound fractures after stopping denosumab, sequencing.
Calcium, Vitamin D & Protein
Daily targets, food-first vs supplements, vitamin D level goals, and the protein requirement for bone health.
Exercise for Bone Density
LIFTMOR trial, impact loading, balance training to prevent falls, and the exercises that actually build bone.
Postmenopausal Osteoporosis
Estrogen deficiency, hormone therapy's bone benefits, WHI reanalysis, and timing of therapy for bone health.
Secondary Osteoporosis
Hyperparathyroidism, hypogonadism, celiac disease, IBD, glucocorticoids, hyperthyroidism — what to screen for.
Fracture Prevention & Fall Risk
Home modifications, balance, medication reduction, hip protectors, and the post-fracture care gap.
Interactive Visualization Bone Remodeling & Calcium Balance Watch osteoclasts tunnel and osteoblasts rebuild — then drop vitamin D and see PTH quietly strip calcium out of your skeleton. Launch → Interactive Visualization Menopause — run the hormones down and set off a hot flash Empty the ovarian follicle pool and watch estradiol swing, then flatten, while FSH climbs — then trigger a hot flash and see the narrowed thermoneutral zone behind it. Launch →
Table of Contents
- What Osteoporosis Is
- Osteopenia vs Osteoporosis
- How Common It Is
- How Bone Works
- Causes: Primary and Secondary
- Risk Factors
- Secondary Causes to Screen For
- Symptoms and Fractures
- Diagnosis: DXA, T-Score, FRAX
- Exercise, Calcium and Vitamin D
- Fall Prevention
- Drug Treatment
- Drug Holidays, ONJ and Atypical Fractures
- Special Populations
- Complications
- Deep-Dive Articles
- Key Research Papers
- Connections
- Featured Videos
What Osteoporosis Is
Osteoporosis has two halves, and most short descriptions only mention the first.
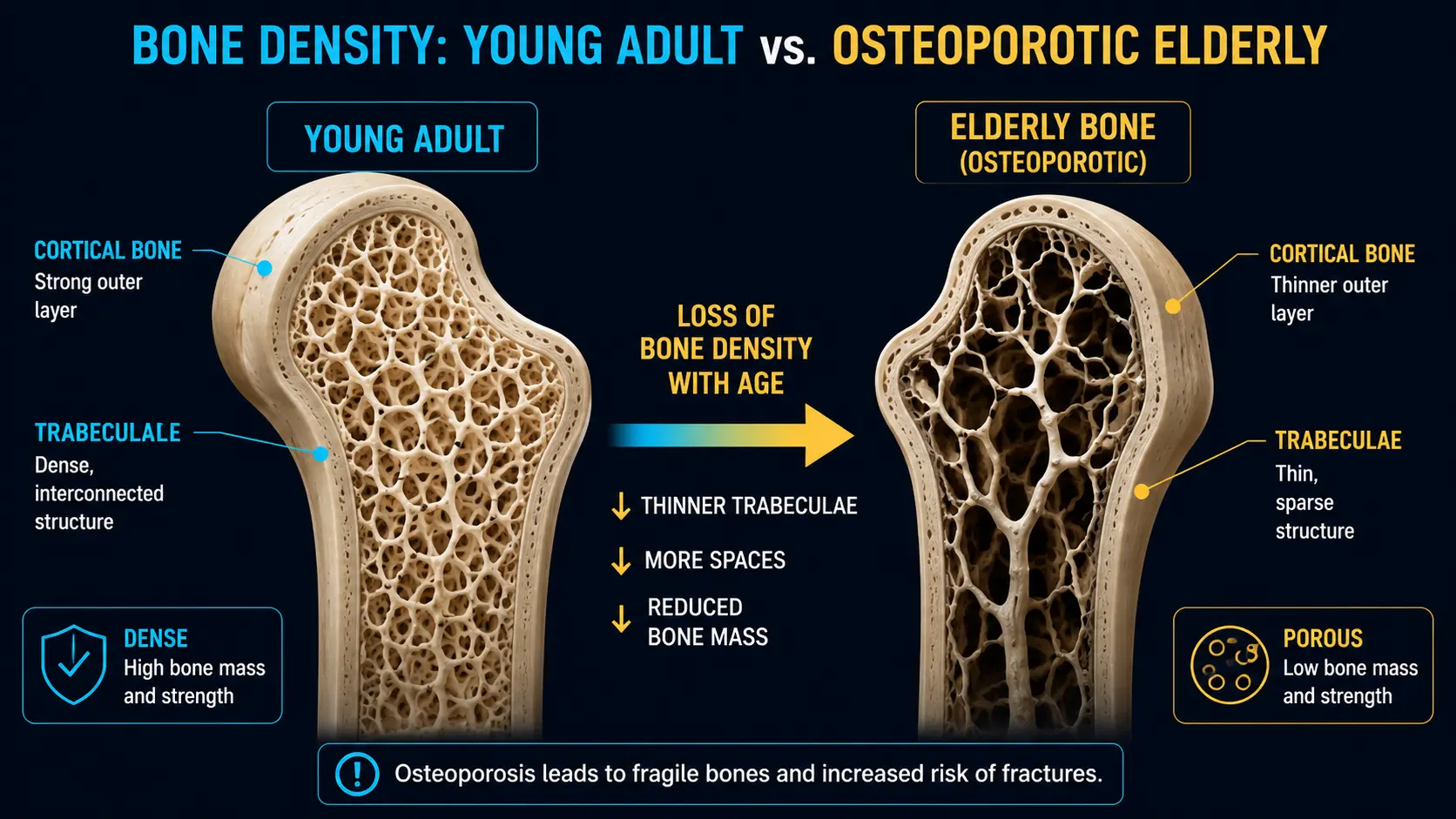
- Loss of bone mass. There is simply less bone tissue than there used to be.
- Deterioration of bone microarchitecture. The internal scaffolding of bone — a lattice of struts called trabeculae — thins, perforates, and loses its cross-connections. Struts that once braced each other end up standing alone.
That second half matters enormously, because it explains something a density number alone cannot: two people can have identical bone density and very different fracture risk. Think of it as the difference between a ladder that is uniformly thinner and a ladder with half its rungs missing. Both weigh less. Only one collapses when you step on it.
This is why the modern definition, from the NIH consensus panel, frames osteoporosis as compromised bone strength, where bone strength reflects the integration of bone density and bone quality. It is also why bone density tests, useful as they are, systematically underestimate who is going to break a bone.
Osteoporosis itself causes no symptoms whatsoever. No ache, no stiffness, no warning twinge. It is not painful, and it is not something you can feel. The first symptom of osteoporosis, in most people, is a broken bone.
Osteopenia vs Osteoporosis — and Where the Fractures Actually Come From
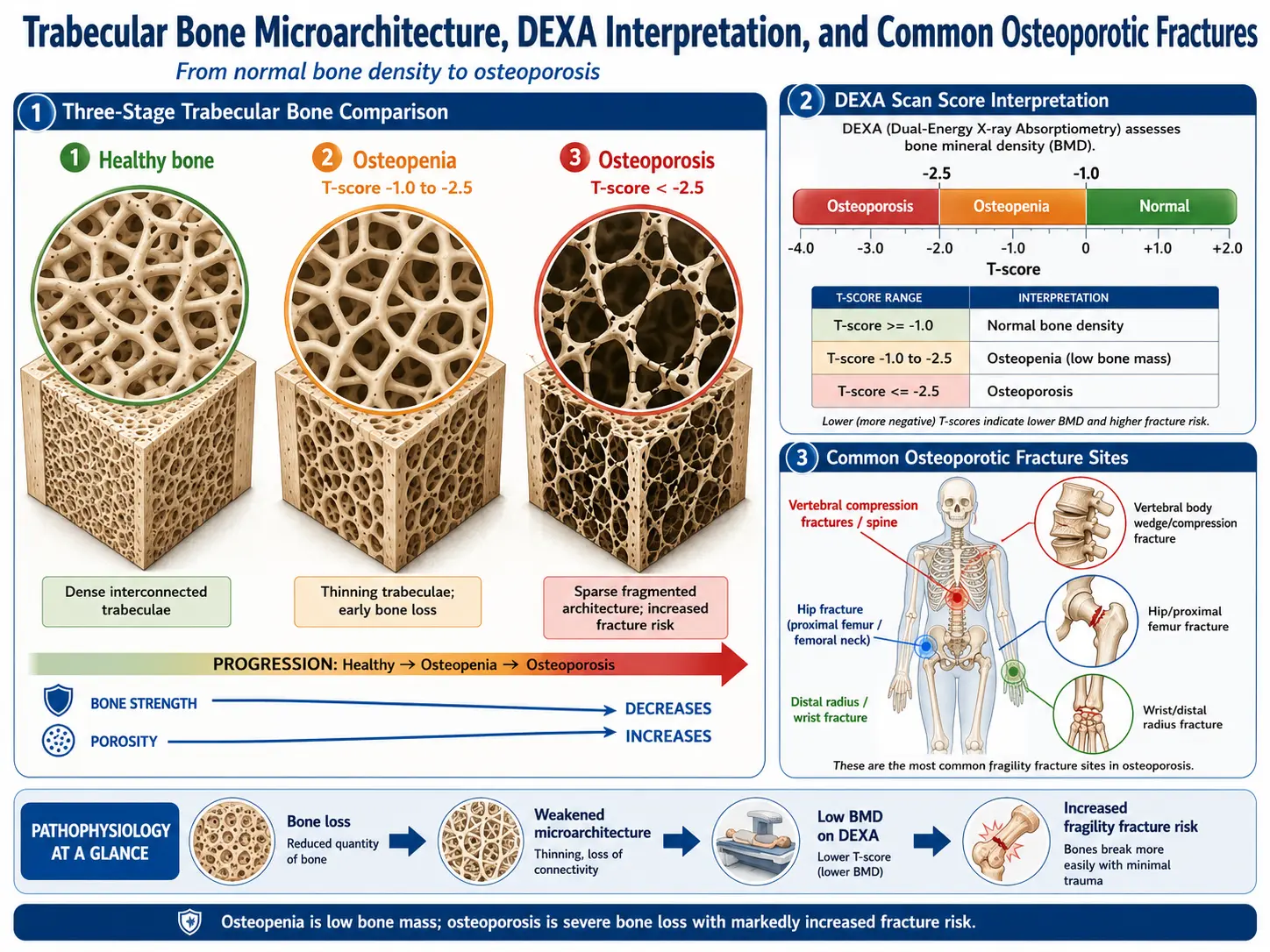
Bone density is reported as a T-score, which says how far your bone density sits above or below that of a healthy young adult, measured in standard deviations. The World Health Organization cut-offs are:
- Normal — T-score above −1.0
- Osteopenia (low bone mass) — T-score between −1.0 and −2.5
- Osteoporosis — T-score of −2.5 or below
- Severe (established) osteoporosis — T-score of −2.5 or below plus a fragility fracture
Osteopenia is the middle ground: thinner than ideal, not yet osteoporotic. It sounds like the safe category. Here is the part almost nobody is told.
Most fragility fractures happen to people who do not have osteoporosis. They happen to people with osteopenia — or with perfectly ordinary bone density.
This is not a subtle statistical footnote. In the NORA study, which tracked nearly 150,000 postmenopausal women for a year after a bone density measurement, only 6.4% had a T-score in the osteoporosis range. Those women did have the highest fracture rate per person. But because they were such a small slice of the population, they accounted for only 18% of the osteoporotic fractures and 26% of the hip fractures. The other 82% of fractures — and 74% of hip fractures — happened to women whose bone density was not in the osteoporotic range. An Australian study put the same finding in its title: the population burden of fractures originates in women with osteopenia, not osteoporosis.
The reason is unglamorous arithmetic. A high-risk group that is small contributes fewer total events than a lower-risk group that is enormous. There are many, many more people with osteopenia than with osteoporosis.
Two practical consequences follow, and they pull in opposite directions:
- "Just osteopenia" is not a clean bill of health. If you have osteopenia plus other risk factors — age, a prior fragility fracture, steroids, a parent who broke a hip — your absolute fracture risk can easily exceed treatment thresholds even though your T-score never crossed −2.5.
- Osteopenia is not, by itself, a disease that needs a drug. Tens of millions of people have it. Treating all of them would be a poor use of medication. The answer is not to treat the label; it is to calculate absolute fracture risk, which is what FRAX exists to do.
In other words: the T-score is an input, not a verdict. Treatment decisions should be driven by overall fracture probability, not by which side of a line your density landed on.
How Common It Is
Roughly 10 million Americans have osteoporosis — about 8 million women and 2 million men — and another 44 million have low bone mass (osteopenia). Together that is more than half of all Americans over 50 with bone density below the healthy range.
Osteoporosis causes about 2 million fractures a year in the United States, at a direct medical cost running into the tens of billions of dollars. After age 50, the lifetime risk of an osteoporotic fracture is roughly 1 in 2 for women and 1 in 4 for men.
- Vertebral (spine) compression fractures are the most common — around 700,000 a year. About two-thirds are silent, discovered incidentally on an X-ray taken for something else entirely.
- Hip fractures — about 300,000 a year — are the most serious. Roughly one in five people dies within a year of a hip fracture (higher in men), and more than half of survivors never return to their previous level of walking or independence.
- Wrist (Colles) fractures, from falling onto an outstretched hand, are often the first osteoporotic fracture, typically in women in their late 50s and 60s. They are a warning shot: the same fragility that let the wrist break also threatens the hip and spine.
Men are consistently under-diagnosed and under-treated. Osteoporosis is not a women's disease; it is a disease that is more common in women.
How Bone Works: Remodeling and Peak Bone Mass
Bone is living tissue that is continuously torn down and rebuilt. Understanding that cycle makes every treatment below make sense.
What bone is made of
By weight, bone is roughly 60–70% mineral, 20–30% organic matrix, and about 10% water. The mineral is hydroxyapatite, a calcium-phosphate crystal that supplies hardness and resistance to compression. The organic matrix is mostly type I collagen — the protein scaffolding that gives bone flexibility and tensile strength. You need both. Mineral without collagen is brittle, like chalk. Collagen without mineral is floppy, like rubber.
The three cell types
- Osteoclasts dissolve bone. They are large multinucleated cells that latch onto bone and secrete acid and enzymes. Their activity is driven by a signal called RANK-L. When oestrogen falls at menopause, RANK-L rises and osteoclasts go into overdrive. Most osteoporosis drugs are, one way or another, ways of shutting osteoclasts down.
- Osteoblasts build bone. They lay down collagen matrix and then mineralize it. Glucocorticoids kill osteoblasts, which is why steroid-induced bone loss is so fast. The newer anabolic drugs work by driving osteoblasts.
- Osteocytes are former osteoblasts now buried inside the bone matrix, wired together through microscopic channels. They are the skeleton's strain gauges: they sense mechanical loading and bending and signal accordingly. This is the mechanism behind "exercise builds bone" — loading deforms bone, osteocytes detect it, and signalling (notably the Wnt pathway) tells osteoblasts to build. Osteocytes also secrete sclerostin, a brake on bone formation — which is precisely the target the drug romosozumab blocks.
Peak bone mass, and the long slide after it
Bone mass builds through childhood and adolescence and peaks somewhere around ages 25 to 30. Roughly 60–80% of your peak is set by genetics; the rest is shaped by nutrition, physical activity, and avoiding smoking during those growing years. A higher peak means more reserve to spend later.
After the peak, everyone loses bone — on the order of 0.5% a year from around age 40. Women then get an additional, much steeper phase: for the first 5 to 10 years after menopause, oestrogen withdrawal drives bone loss of roughly 2–3% per year, sometimes more. That accelerated window is why postmenopausal women dominate the statistics.
Two kinds of bone, and why the spine goes first
Cortical bone is the dense outer shell and makes up about 80% of skeletal mass. Trabecular bone is the inner spongy lattice, concentrated in the vertebrae, the wrist, and the femoral neck. Trabecular bone has far more surface area and turns over much faster — so it is hit first and hardest. That is the anatomical reason vertebral and wrist fractures typically precede hip fractures by a decade or more.
Causes: Primary and Secondary Osteoporosis
Primary osteoporosis
Primary osteoporosis has no other disease driving it.
- Postmenopausal (type I) — driven by oestrogen deficiency. Oestrogen restrains osteoclasts; when it drops, RANK-L surges and resorption outruns formation. It preferentially strips trabecular bone, so vertebral and wrist fractures predominate.
- Age-related (type II) — affects both sexes over roughly 70, and involves both cortical and trabecular bone. The drivers are different: the kidney makes less active vitamin D, the gut absorbs less calcium, and parathyroid hormone (PTH) rises to compensate — quietly pulling calcium out of the skeleton. Hip fractures are the characteristic injury.
Secondary osteoporosis
Secondary osteoporosis is caused by another disease or a medication. It is much more often the story in men — a secondary cause is found in up to half of men with osteoporosis — and in premenopausal women, where it is nearly always the explanation. Common causes:
- Glucocorticoids — by far the most common drug cause. Prednisone and its relatives kill osteoblasts and raise RANK-L, so bone is lost fast, most of it within the first 6–12 months. Fracture risk rises before bone density has fallen much, which is why the DXA can look reassuring while the risk is already real.
- Aromatase inhibitors (breast cancer) and androgen deprivation therapy (prostate cancer) — both deliberately strip out the sex hormones that protect bone, and both cause rapid loss.
- Malabsorption — coeliac disease, Crohn's disease, and bariatric surgery all impair calcium and vitamin D absorption.
- Anorexia nervosa and the female athlete triad — low body weight, low oestrogen, and low energy intake, often in women who should still be at peak bone mass.
- Chronic kidney disease — leads to a complex bone disorder (renal osteodystrophy) and secondary hyperparathyroidism. It also changes which drugs are safe.
- Anticonvulsants (phenytoin, carbamazepine) — induce liver enzymes that accelerate vitamin D breakdown.
- Proton pump inhibitors — long-term use is associated with modestly higher fracture risk in observational studies. The evidence is associational, not proven cause and effect, and should not by itself stop a PPI that is genuinely needed.
Risk Factors
Things you cannot change
- Age — the single most powerful risk factor. Risk climbs steeply with each decade.
- Postmenopausal oestrogen loss — the accelerating event for most women. Early menopause (before 45) or surgical removal of the ovaries increases risk further.
- Prior fragility fracture — the strongest single predictor of the next one. Any bone broken by a fall from standing height or less counts, and roughly doubles-to-triples future fracture risk. Risk is highest in the first 1–2 years afterwards — a window in which treatment is most valuable and least often started.
- Family history, particularly a parent who fractured a hip — roughly doubles risk.
- Female sex — smaller, less dense bones at peak, plus the menopausal cliff.
- Ethnicity — fracture rates are highest in white and Asian populations and lowest in Black populations, though the reasons are not fully understood and the practice of applying race adjustments in risk calculators is now actively debated.
Things you can change
- Glucocorticoids — the most important modifiable medical risk. Any dose from about 2.5–5 mg of prednisone-equivalent daily for 3 months or more warrants a formal fracture-risk assessment, and risk climbs steeply above 5–7.5 mg/day. Use the lowest dose for the shortest time, and assess bone at the start, not later.
- Smoking — a dose-dependent, independent risk factor for fracture in meta-analysis, and part of the FRAX calculation. Stopping helps; some of the effect is reversible.
- Low body weight — a BMI below about 20 is an independent risk factor. Less mechanical loading, less padding over the hip, and less peripheral oestrogen.
- Excess alcohol — more than about 2–3 units a day suppresses osteoblasts, worsens nutrition, and sharply raises the odds of falling.
- Physical inactivity — bone maintains only what it is asked to carry.
- Low vitamin D and low calcium intake — not usually a cause of osteoporosis on their own, but they make everything else worse and they blunt the drugs.
- Anything that makes you fall — poor balance, weak legs, bad vision, sedatives, blood-pressure drops on standing, clutter on the floor.
Secondary Causes Worth Screening For
When osteoporosis is diagnosed — and especially in a man, a premenopausal woman, or anyone whose bone loss looks out of proportion to their age — it is worth a deliberate hunt for a treatable underlying cause. Finding one can change the treatment entirely, and sometimes stops the bone loss at its source.
The conditions most worth excluding, and the tests that find them:
- Vitamin D deficiency — measure 25-hydroxyvitamin D. Common, easily corrected, and it must be corrected before starting a potent antiresorptive drug, or you risk provoking hypocalcaemia.
- Primary hyperparathyroidism — measure serum calcium and PTH. Excess PTH strips cortical bone. A high calcium with a non-suppressed PTH is the giveaway. It is surgically curable.
- Coeliac disease — tissue transglutaminase (tTG-IgA) antibodies, with total IgA. It can be entirely silent in the gut and present as bone loss. A gluten-free diet reverses the malabsorption.
- Hyperthyroidism — measure TSH. Excess thyroid hormone speeds up remodeling and tips it toward net loss. Note this includes over-replacement with levothyroxine, which is a very common and easily fixed cause.
- Hypogonadism — measure testosterone in men; ask about periods in premenopausal women. Low testosterone is the male equivalent of oestrogen loss and one of the leading secondary causes in men.
- Multiple myeloma — serum protein electrophoresis with free light chains, plus a full blood count. Myeloma can masquerade as osteoporosis with vertebral collapse. Missing it is a serious error, and unexplained anaemia, kidney impairment, or high calcium alongside fractures should raise the alarm loudly.
A reasonable baseline panel: full blood count, comprehensive metabolic panel (calcium, kidney and liver function), 25-hydroxyvitamin D, PTH, TSH, tTG-IgA, serum protein electrophoresis, testosterone in men, and a 24-hour urine calcium (which detects both malabsorption and excessive renal calcium loss).
Symptoms and What Fractures Actually Do
To repeat, because it is the most misunderstood thing about this disease: osteoporosis has no symptoms. Everything below is a symptom of a fracture.
Vertebral compression fractures
These can happen from astonishingly little — bending to lift a bag of shopping, a hard sneeze, or nothing identifiable at all. Two-thirds produce no acute symptoms. When they do, it is sudden, often severe mid or lower back pain.
Accumulated silently over years, they produce the visible signature of the disease: height loss, and a forward curve of the upper spine (kyphosis). In severe cases the ribcage descends toward the pelvis, which compresses the chest and abdomen and causes breathlessness and early fullness at meals. Losing more than 4 cm (about 1.5 inches) of height from your young-adult height is a genuine clinical signal and should prompt spine imaging — not a shrug about getting older.
Hip fractures
The leg typically cannot bear weight, and looks shortened and turned outward. This is a surgical emergency; guidelines push for repair within 24–48 hours because delay costs lives. Even with prompt surgery, roughly one in five patients dies within the year, and more than half never walk as well as they did.
The rule that matters most
Any fracture from a fall from standing height or less is a fragility fracture — and a fragility fracture at the hip or spine is diagnostic of osteoporosis on its own, no matter what the DXA says. The bone failed under a force that should not have broken it. That is the diagnosis. A normal-looking bone density scan does not overrule it.
And yet the majority of people who break a bone this way are never assessed, never diagnosed, and never treated. That gap — the failure to act on the single loudest warning the body can give — is the biggest missed opportunity in the whole field.
Diagnosis: DXA, T-Score and FRAX
The DXA scan
Dual-energy X-ray absorptiometry — DXA, said "dexa" — is the standard test. It measures bone mineral density at the lumbar spine and the hip. It takes 10–20 minutes, requires no preparation, involves no injections, and delivers less radiation than a chest X-ray.
T-score and Z-score
The T-score compares you to a healthy young adult, and generates the WHO categories listed above: normal above −1.0, osteopenia between −1.0 and −2.5, osteoporosis at or below −2.5.
The Z-score compares you to people of your own age and sex. It is the more meaningful number in premenopausal women, in men under 50, and in children. A Z-score below −2.0 means you are losing bone faster than your peers, which is a strong prompt to go hunting for a secondary cause.
FRAX — 10-year fracture risk
A T-score tells you about density. FRAX tells you about risk, which is what you actually want to know. It is a free calculator that estimates your 10-year probability of a major osteoporotic fracture (spine, hip, wrist, or shoulder) and, separately, of a hip fracture.
It folds in age, sex, BMI, prior fragility fracture, parental hip fracture, current smoking, alcohol intake, glucocorticoid use, rheumatoid arthritis, and other secondary causes — plus, optionally, your femoral neck bone density. It works with or without a DXA result, which makes it useful before anyone has been scanned.
In the United States, the commonly used treatment thresholds are a 10-year risk of ≥20% for major osteoporotic fracture or ≥3% for hip fracture. Crossing either one is grounds for drug therapy regardless of whether the T-score ever reached −2.5.
That last clause is the whole point, and it is how the profession answers the osteopenia problem described earlier. FRAX exists precisely so that a 72-year-old with a T-score of −1.8, a wrist fracture last year, and 10 mg of prednisone a day gets treated — instead of being reassured that she does not technically have osteoporosis.
Who should be scanned
- All women aged 65 and over, and all men aged 70 and over
- Postmenopausal women under 65 with an added risk factor
- Anyone who has had a fragility fracture, at any age
- Anyone on long-term glucocorticoids or another bone-losing drug
- Anyone with a disease known to cause bone loss
Many DXA machines can also take a lateral spine image (vertebral fracture assessment) to look for the silent vertebral fractures that two-thirds of patients never knew they had. Finding one changes everything, because it converts "low bone density" into "established osteoporosis with a fracture" — and that is an unambiguous indication to treat.
Exercise, Calcium and Vitamin D — What Actually Works
This section needs to be honest, because the honest version is more useful than the reassuring one.
Exercise — the most reliable lever you control
Of everything you can do without a prescription, resistance and weight-bearing exercise has the best evidence. It works on both halves of the fracture equation at once: it puts load through bone, and it makes you less likely to fall over.
The loading has to be meaningful. Bone responds to strain, not to duration. Walking is good for you and is better than sitting, but it is a weak stimulus for a skeleton that already walks every day. The interventions that actually move bone density are progressive, heavy resistance training and impact loading. In the LIFTMOR trial, postmenopausal women with low bone mass performed supervised high-intensity resistance and impact training twice a week and improved bone density at the spine and hip, along with height, strength, and function — with a very low injury rate, in exactly the population usually told to avoid lifting anything heavy.
What this means in practice:
- Resistance training 2–3 times a week, working the hips, legs, and back extensors. It must get progressively harder over time or it stops working.
- Weight-bearing and impact activity — brisk walking, stair climbing, dancing, and where appropriate, hopping or jumping.
- Balance training, which is where the fall-prevention benefit lives.
- Swimming and cycling do not build bone. They are excellent for your heart and joints, and you should not stop, but they are not weight-bearing and will not do this job.
- With severe spinal osteoporosis, avoid loaded forward bending (sit-ups, toe-touches) and forceful twisting, which can compress already-fragile vertebrae. Get supervision rather than avoiding exercise altogether — deconditioning is its own risk.
The honest caveat: exercise produces modest gains in bone density, and no trial has ever been large enough to prove that exercise alone prevents hip fractures. Its proven, high-certainty benefit is that it reduces falls — and falls are what break bones. It is not a substitute for drug therapy in someone with established osteoporosis.
Calcium and vitamin D — necessary, but not treatments
This is where most osteoporosis advice quietly goes wrong. Calcium and vitamin D are adjuncts. They are the floor beneath treatment, not treatment itself.
Be clear about what the evidence shows:
- A JAMA meta-analysis of 33 randomised trials covering 51,145 community-dwelling older adults found no significant reduction in hip, vertebral, non-vertebral, or total fractures from calcium, vitamin D, or the two combined. This held regardless of dose, sex, fracture history, or baseline vitamin D level.
- The VITAL trial gave 2,000 IU of vitamin D3 daily to 25,871 generally healthy adults not selected for deficiency or low bone mass, and followed them for a median of 5.3 years. It did not reduce fractures (hazard ratio 0.98).
- Supplements do help where there is a genuine deficit. The classic Chapuy trial gave calcium and vitamin D3 to elderly women in French nursing homes — a population with poor intake and low vitamin D — and did reduce hip fractures.
- More is not better. A trial of a single annual 500,000 IU dose of vitamin D increased falls and fractures. High intermittent bolus dosing is a bad idea.
So: correct a deficiency, do not chase a megadose. Reasonable targets are around 1,000–1,200 mg of calcium a day, food first, and enough vitamin D to keep you replete (commonly 800–2,000 IU/day of D3, guided by your 25-hydroxyvitamin D level). Dairy, tinned sardines and salmon with the bones, fortified plant milks, tofu set with calcium, kale and bok choy are all good calcium sources. If you supplement, split doses of 500 mg or less absorb better; calcium citrate does not need stomach acid and is the right choice if you take a PPI or have had bariatric surgery. Very high supplemental calcium intakes have been linked in some studies to cardiovascular risk, which is another reason to meet the target from food and use supplements only to close a gap.
Adequate protein matters too and is routinely neglected in older adults — bone is roughly a quarter protein by weight, and muscle mass protects against falls.
Here is the sentence that ties it together. In every pivotal osteoporosis drug trial — FIT, HORIZON, FREEDOM, the teriparatide trial, FRAME, ARCH — both the treatment group and the placebo group received calcium and vitamin D. The fracture reductions those drugs achieved were on top of calcium and vitamin D repletion. Calcium and vitamin D are the baseline on which the drugs work. In someone with established osteoporosis, taking them instead of a proven drug is not a conservative choice. It is an ineffective one.
Fall Prevention
Almost every fracture outside the spine needs two things: a weak bone and a fall. Drugs address the first. Nothing but deliberate effort addresses the second, and it is chronically under-emphasised.
The Cochrane review of exercise for fall prevention pooled 108 trials and 23,407 community-dwelling older people. The findings are unusually solid:
- Exercise of any kind reduced the rate of falls by 23% (high-certainty evidence).
- Balance and functional exercise reduced falls by 24%, and combining balance/functional work with resistance training reduced falls by 34% — the best result of any category.
- Tai chi reduced the rate of falls by about 19%. It is genuinely effective, and it is often over-sold; the real number is meaningful without being miraculous.
- Exercise probably also reduces fall-related fractures, though that evidence is weaker.
Beyond exercise, the highest-yield actions:
- Review every medication. This is the most overlooked intervention on the list. Benzodiazepines, "Z-drug" sleeping tablets, opioids, antipsychotics, anticholinergics (including many over-the-counter antihistamines), and blood pressure drugs that cause dizziness on standing all raise fall risk substantially. Deprescribing is a real treatment.
- Get vision checked — and be careful with new varifocals, which distort depth perception on stairs.
- Fix the house — loose rugs, trailing cables, dark stairways, no grab rails in the bathroom.
- Check for postural hypotension — a blood pressure drop on standing is a common and treatable cause of falls.
- Hip protectors can reduce hip fracture in high-risk people in care settings, but real-world compliance is poor, so the population-level evidence is mixed.
Finally, fracture liaison services — systematic programmes that catch every patient presenting with a fragility fracture and make sure they are assessed and treated before discharge — close the single widest gap in osteoporosis care. Without them, most people who fracture are never worked up at all, despite having just supplied definitive proof that their bones are failing.
Drug Treatment
Treatment is indicated for a fragility fracture of the hip or spine, a T-score of −2.5 or below, or a FRAX risk over threshold. The drugs below are not interchangeable, and the differences matter.
Bisphosphonates — the usual first choice
Bisphosphonates bind to bone mineral, get swallowed by osteoclasts as they chew through it, and poison them from the inside. Resorption slows and density recovers. They are cheap, oral options exist, and they have the longest safety record.
- Alendronate — 70 mg once weekly by mouth. In the Fracture Intervention Trial, in women who already had a vertebral fracture, alendronate cut new vertebral fractures by about 47% and hip fractures by about 51% over three years. (Worth knowing: in the companion arm of the same trial, in women with low bone density but no prior vertebral fracture, it did not significantly reduce clinical fractures overall — the benefit was concentrated in the higher-risk group. This is exactly why absolute risk, not just density, should drive the decision to treat.)
- Risedronate — 35 mg weekly; similar efficacy, sometimes better tolerated.
- Zoledronic acid — 5 mg by intravenous infusion once a year. It bypasses the stomach and the adherence problem entirely. In the HORIZON Pivotal Fracture Trial it reduced vertebral fractures by 70% and hip fractures by 41%. Separately — and this is a different trial, often confused with the first — the HORIZON Recurrent Fracture Trial gave zoledronic acid to patients after hip fracture surgery and found not only 35% fewer new clinical fractures but a 28% reduction in deaths (9.6% vs 13.3%). That mortality benefit belongs to the post-hip-fracture trial, not to the original pivotal trial, and it is one of the most striking results in the field.
How to take the oral ones: first thing in the morning, on an empty stomach, with a full glass of plain water, and stay upright for at least 30 minutes. Lying down lets the tablet reflux into the oesophagus and burn it. This is the main reason people abandon oral bisphosphonates, and it is almost entirely preventable by following the rules.
Denosumab — powerful, and you cannot simply stop it
Denosumab is an antibody against RANK-L. Block RANK-L and osteoclasts never mature. It is given as a 60 mg injection under the skin every 6 months. In the FREEDOM trial it cut vertebral fractures by 68%, hip fractures by 40%, and non-vertebral fractures by 20% over three years.
Two things about denosumab are critical, and both are frequently missed.
1. The rebound. Do not stop denosumab without a plan. Unlike bisphosphonates, denosumab is not retained in bone. When it wears off, the suppressed osteoclasts come back all at once. In the FREEDOM analysis, the vertebral fracture rate in people who stopped denosumab rose from 1.2 per 100 patient-years on treatment to 7.1 per 100 patient-years off it — essentially back to the untreated rate (8.5 in those who stopped placebo). So the overall rate returns to baseline rather than exceeding it. But the character of the fractures changes, and that is the real danger: among those who did fracture after stopping, 60.7% sustained multiple vertebral fractures, compared with 38.7% of those who stopped placebo. People with a prior vertebral fracture were nearly four times more likely to suffer a multiple-fracture event.
The practical rule is simple and important: if denosumab is stopped, for any reason, it must be followed promptly by a bisphosphonate to lock in the gains. This includes stopping because of a missed appointment, a house move, an insurance lapse, or a dental procedure. A late denosumab injection is not a minor administrative issue.
2. Severe hypocalcaemia in advanced kidney disease. Denosumab used to be recommended fairly freely in renal impairment because it is not cleared by the kidneys. That advice is now out of date. In January 2024 the FDA added a boxed warning for severe hypocalcaemia in patients with advanced CKD, particularly those on dialysis. The study behind it found severe hypocalcaemia within 12 weeks in 41.1% of dialysis-dependent women started on denosumab, versus 2.0% of those started on an oral bisphosphonate — with hospitalisations, life-threatening events, and deaths. Vitamin D must be repleted and calcium monitored before and after dosing in anyone with significant kidney disease.
Anabolic agents — for high risk, and they build bone rather than just preserving it
Everything above slows demolition. These drugs drive construction. They are reserved for severe or very-high-risk osteoporosis: very low T-scores, multiple vertebral fractures, or fracture despite an antiresorptive.
- Teriparatide — a fragment of parathyroid hormone (PTH 1-34), self-injected daily. The paradox is elegant: PTH continuously elevated (as in hyperparathyroidism) destroys bone, but delivered in brief daily pulses it stimulates osteoblasts to build it. In the pivotal trial it reduced vertebral fractures by 65% and non-vertebral fragility fractures by 53%.
An outdated claim worth correcting: teriparatide was long described as carrying a hard two-year lifetime limit and a boxed warning for osteosarcoma, based on a rat study. In November 2020 the FDA removed both — the boxed warning and the cumulative lifetime restriction — after 15+ years of surveillance found no increase in osteosarcoma in treated humans. Treatment beyond two years is now permissible where fracture risk remains high. A standard course is still usually about two years. - Abaloparatide — a related PTH-receptor agonist, also daily by injection. In the ACTIVE trial it reduced new vertebral fractures by 86% versus placebo. Its osteosarcoma boxed warning was likewise removed.
- Romosozumab — an antibody against sclerostin, the brake osteocytes put on bone formation. Releasing that brake both builds bone and reduces resorption at the same time, which no other drug does. Given as 210 mg monthly (two injections) for 12 months. In the FRAME trial it cut vertebral fractures sharply versus placebo. In the ARCH trial (2017 — the drug was approved in 2019, but the trial published in 2017), romosozumab followed by alendronate beat alendronate alone: new vertebral fractures 6.2% vs 11.9% (48% lower), hip fractures 2.0% vs 3.2% (38% lower).
The cardiovascular signal, honestly: in ARCH's first year, adjudicated serious cardiovascular events occurred in 2.5% (50/2,040) of the romosozumab group versus 1.9% (38/2,014) on alendronate — an absolute difference of about 0.6 percentage points. No such imbalance appeared against placebo in FRAME. It is a real signal and it carries a boxed warning; romosozumab should be avoided in anyone who has had a heart attack or stroke in the past year.
Sequence matters, and one order is actively wrong. Anabolic first, then antiresorptive, produces much bigger gains than the reverse. The DATA-Switch study showed that giving teriparatide after denosumab caused a transient loss of bone density, while giving denosumab after teriparatide produced large increases. Every anabolic must be followed by an antiresorptive when it ends, or the new bone is lost again.
Raloxifene
A selective oestrogen receptor modulator: it acts like oestrogen on bone without stimulating breast tissue. It reduces vertebral fractures by roughly 30–50% but has never been shown to reduce hip fractures. It also lowers invasive breast cancer risk, which makes it appealing for some women. It raises the risk of blood clots, so it is unsuitable for anyone with a clotting history.
Where HRT fits
Oestrogen genuinely works on bone. The Women's Health Initiative — still the only trial to test fracture outcomes in an unselected population — found combined oestrogen-plus-progestin reduced hip fractures by about a third and total fractures by about a quarter. That is a real effect, and it is often forgotten in the reaction against HRT.
The nuance is who and when. WHI enrolled women averaging 63 years old, many long past menopause, and found increases in breast cancer, stroke, and clots that shifted the risk-benefit against routine use in that group. Current guidance is:
- HRT is a reasonable way to protect bone in women who are under about 60, or within 10 years of menopause, and have menopausal symptoms — where the balance of risks is much more favourable.
- It is not first-line therapy for established osteoporosis in an older woman with no menopausal symptoms. A bone-specific drug is the better choice.
- Bone protection stops when HRT stops, and bone loss resumes. It is not a one-off intervention.
Drug Holidays, Jaw Osteonecrosis and Atypical Femoral Fractures
Two rare complications dominate patient fear about osteoporosis drugs, and fear of them keeps people off treatment who badly need it. Both are real. Both are also far rarer than the fractures they are being weighed against. The honest numbers are the best antidote to both dismissal and panic.
Osteonecrosis of the jaw (ONJ)
Exposed, non-healing bone in the jaw. At the doses used for osteoporosis, the international consensus estimate of incidence is 0.001% to 0.01% — roughly 1 in 10,000 to 1 in 100,000 — which is only marginally above the background rate in untreated people (under 0.001%).
The reason ONJ has such a fearsome reputation is that the figures people hear come from a different population: cancer patients, who receive these drugs intravenously at 10–12 times the osteoporosis dose and far more frequently. There the incidence is 1% to 15%. That is a genuinely serious risk — and it is not your risk if you are taking weekly alendronate for osteoporosis.
Sensible precautions: complete planned invasive dental work before starting, and keep up good oral hygiene. Routine dental care, cleanings, and fillings do not require stopping treatment.
Atypical femoral fracture (AFF)
A stress fracture through the outer side of the thigh bone, in a spot ordinary fractures do not occur. It is associated with long-duration bisphosphonate use, and the risk rises sharply the longer treatment continues — in a study of 196,129 women, the hazard ratio rose from about 8.9 after 3–5 years of use to 43.5 after 8 or more years, compared with less than 3 months of use.
Those hazard ratios sound terrifying, so hold them next to the absolute numbers from the same study. Over three years of bisphosphonate treatment in white women, roughly 149 hip fractures were prevented for every 2 atypical femoral fractures caused. The benefit outweighs the harm by a wide margin. The margin is narrower — though still favourable — in Asian women, who have a substantially higher AFF risk (hazard ratio 4.84 versus white women). Risk also falls rapidly once the drug is stopped.
The warning sign is worth memorising: new, persistent, dull pain in the thigh or groin in someone on long-term bisphosphonates. It often precedes the complete fracture by weeks or months, and imaging at that point can catch it before the bone breaks all the way through. Report it; do not wait it out.
Drug holidays
Because bisphosphonates are retained in bone and keep working for a while after the last dose, they are the one drug class where a planned pause makes sense — reducing cumulative exposure and the small long-term risks above without immediately surrendering the protection.
- Reassess after 5 years of oral or 3 years of intravenous bisphosphonate.
- If risk is now moderate — T-score improved above −2.5, no new fractures — a holiday of 2–3 years is reasonable, with monitoring.
- If risk remains high — a prior hip or vertebral fracture, a T-score still at or below −2.5, ongoing steroids — continue. Guidelines support up to 10 years of oral or 6 years of intravenous therapy in this group.
- A holiday is a pause with a review date, not an exit. Risk must be reassessed and treatment restarted when it climbs.
Drug holidays apply to bisphosphonates only. Applying the same logic to denosumab is dangerous — see the rebound above. Anabolic agents likewise cannot simply be stopped; they must be followed by an antiresorptive.
Special Populations
Glucocorticoid-induced osteoporosis
The most common drug-induced cause, and the one where waiting is most costly. Steroids suppress osteoblasts directly, so bone is lost quickly — most of it in the first 6–12 months — and fracture risk rises before the DXA looks bad. Do not wait for the scan to deteriorate.
Anyone starting 3+ months of glucocorticoids should have a fracture-risk assessment at the outset, be ensured adequate calcium and vitamin D, and in most cases start a bisphosphonate concurrently with the steroid rather than after the damage is visible. Teriparatide is preferred in the highest-risk patients, since it directly counteracts the osteoblast suppression that steroids cause.
Men
Under-screened, under-diagnosed, and under-treated, with higher post-fracture mortality than women. Up to half have an identifiable secondary cause — most often hypogonadism, alcohol, glucocorticoids, or malabsorption — so a full secondary workup including testosterone is essential. The same T-score thresholds and the same drugs apply; bisphosphonates, denosumab, teriparatide, abaloparatide and romosozumab are all approved for men.
Premenopausal women
Genuinely uncommon, and almost always secondary — anorexia nervosa, exercise-associated amenorrhoea, coeliac disease, or glucocorticoids. Use the Z-score, not the T-score. Treatment is aimed at the underlying cause. Bisphosphonates persist in bone for years and cross the placenta, so they are used cautiously and with specialist input in anyone who may become pregnant.
After bariatric surgery
Gastric bypass and sleeve gastrectomy cause substantial bone loss — through impaired calcium and vitamin D absorption, secondary hyperparathyroidism, gut hormone changes, and the simple loss of skeletal loading that comes with losing weight. These patients need calcium citrate (which does not require stomach acid), generous vitamin D, and baseline plus follow-up DXA — often at an age when nobody would otherwise think to scan them.
Chronic kidney disease
Bone disease in advanced CKD is not ordinary osteoporosis, and the drugs behave differently. Bisphosphonates are generally avoided below an eGFR of about 30–35, and denosumab now carries a boxed warning for severe hypocalcaemia in this group. This is territory for a specialist, not a protocol.
Complications
- Fractures — the whole point of the disease. Hip and vertebral fractures carry the most consequence.
- Loss of independence — over half of hip fracture survivors never walk as well again, and many never return home.
- Chronic pain and deformity — from accumulated vertebral collapse.
- Restricted breathing and early satiety — when severe kyphosis compresses the chest and abdomen.
- Increased mortality — roughly one in five dies within a year of a hip fracture, and vertebral fractures also carry excess mortality.
- The fracture cascade — one fragility fracture sharply raises the odds of the next, with the risk concentrated in the following 1–2 years. This is the moment to intervene, and it is the moment most often missed.
Key Research Papers
Every citation below has been checked against PubMed. Each links to the paper's PubMed record.
Definition, diagnosis and risk assessment
- NIH Consensus Development Panel on Osteoporosis Prevention, Diagnosis, and Therapy. Osteoporosis prevention, diagnosis, and therapy. JAMA. 2001;285(6):785–795. PMID: 11176917 — the consensus that redefined osteoporosis as compromised bone strength, not just low density.
- Compston JE, McClung MR, Leslie WD. Osteoporosis. Lancet. 2019;393(10169):364–376. PMID: 30696576 — comprehensive modern review.
- Siris ES, Chen YT, Abbott TA, et al. Bone mineral density thresholds for pharmacological intervention to prevent fractures. Arch Intern Med. 2004;164(10):1108–1112. PMID: 15159268 — the NORA study: only 6.4% of women had osteoporosis by T-score, yet they accounted for just 18% of fractures.
- Pasco JA, Seeman E, Henry MJ, et al. The population burden of fractures originates in women with osteopenia, not osteoporosis. Osteoporos Int. 2006;17(9):1404–1409. PMID: 16699736
- Kanis JA, Johnell O, Oden A, et al. FRAX and the assessment of fracture probability in men and women from the UK. Osteoporos Int. 2008;19(4):385–397. PMID: 18292978
- Kanis JA, Johnell O, Oden A, et al. Smoking and fracture risk: a meta-analysis. Osteoporos Int. 2005;16(2):155–162. PMID: 15175845
- Shoback D, Rosen CJ, Black DM, et al. Pharmacological management of osteoporosis in postmenopausal women: an Endocrine Society guideline update. J Clin Endocrinol Metab. 2020;105(3):587–594. PMID: 32068863
Bisphosphonates
- Black DM, Cummings SR, Karpf DB, et al. Randomised trial of effect of alendronate on risk of fracture in women with existing vertebral fractures (Fracture Intervention Trial). Lancet. 1996;348(9041):1535–1541. PMID: 8950879 — the trial that launched the bisphosphonate era. Note the population: women who already had a vertebral fracture.
- Cummings SR, Black DM, Thompson DE, et al. Effect of alendronate on risk of fracture in women with low bone density but without vertebral fractures (FIT). JAMA. 1998;280(24):2077–2082. PMID: 9875874 — the companion arm, and the reason absolute risk matters more than density alone.
- Black DM, Delmas PD, Eastell R, et al. Once-yearly zoledronic acid for treatment of postmenopausal osteoporosis (HORIZON Pivotal Fracture Trial). N Engl J Med. 2007;356(18):1809–1822. PMID: 17476007 — 70% fewer vertebral and 41% fewer hip fractures.
- Lyles KW, Colón-Emeric CS, Magaziner JS, et al. Zoledronic acid and clinical fractures and mortality after hip fracture (HORIZON Recurrent Fracture Trial). N Engl J Med. 2007;357(18):1799–1809. PMID: 17878149 — this is the trial that found a 28% reduction in deaths (9.6% vs 13.3%), not the pivotal trial above.
- Adler RA, El-Hajj Fuleihan G, Bauer DC, et al. Managing osteoporosis in patients on long-term bisphosphonate treatment: report of a task force of the ASBMR. J Bone Miner Res. 2016;31(1):16–35. PMID: 26350171 — the basis for drug-holiday practice.
Denosumab, anabolic agents and sequencing
- Cummings SR, San Martin J, McClung MR, et al. Denosumab for prevention of fractures in postmenopausal women with osteoporosis (FREEDOM). N Engl J Med. 2009;361(8):756–765. PMID: 19671655
- Cummings SR, Ferrari S, Eastell R, et al. Vertebral fractures after discontinuation of denosumab: a post hoc analysis of the FREEDOM trial and its extension. J Bone Miner Res. 2018;33(2):190–198. PMID: 29105841 — the rebound. Off-treatment vertebral fracture rate 7.1 vs 1.2 per 100 patient-years; 60.7% of those who fractured had multiple vertebral fractures.
- Tsourdi E, Zillikens MC, Meier C, et al. Fracture risk and management of discontinuation of denosumab therapy: a systematic review and position statement by ECTS. J Clin Endocrinol Metab. 2021;106(1):264–281. PMID: 33103722
- Bird ST, Smith ER, Gelperin K, et al. Severe hypocalcemia with denosumab among older female dialysis-dependent patients. JAMA. 2024;331(6):491–499. PMID: 38241060 — the study behind the FDA's January 2024 boxed warning.
- Neer RM, Arnaud CD, Zanchetta JR, et al. Effect of parathyroid hormone (1-34) on fractures and bone mineral density in postmenopausal women with osteoporosis. N Engl J Med. 2001;344(19):1434–1441. PMID: 11346808 — teriparatide: 65% fewer vertebral, 53% fewer non-vertebral fractures.
- Krege JH, Gilsenan AW, Komacko JL, Kellier-Steele N. Teriparatide and osteosarcoma risk: history, science, elimination of boxed warning, and other label updates. JBMR Plus. 2022;6(9):e10665. PMID: 36111201 — why the two-year lifetime limit and osteosarcoma boxed warning were removed in 2020.
- Miller PD, Hattersley G, Riis BJ, et al. Effect of abaloparatide vs placebo on new vertebral fractures in postmenopausal women with osteoporosis (ACTIVE). JAMA. 2016;316(7):722–733. PMID: 27533157
- Cosman F, Crittenden DB, Adachi JD, et al. Romosozumab treatment in postmenopausal women with osteoporosis (FRAME). N Engl J Med. 2016;375(16):1532–1543. PMID: 27641143
- Saag KG, Petersen J, Brandi ML, et al. Romosozumab or alendronate for fracture prevention in women with osteoporosis (ARCH). N Engl J Med. 2017;377(15):1417–1427. PMID: 28892457 — 48% fewer vertebral and 38% fewer hip fractures than alendronate; serious cardiovascular events 2.5% vs 1.9% in year one.
- Leder BZ, Tsai JN, Uihlein AV, et al. Denosumab and teriparatide transitions in postmenopausal osteoporosis (DATA-Switch). Lancet. 2015;386(9999):1147–1155. PMID: 26144908 — why anabolic-first, antiresorptive-second is the right order.
- Ettinger B, Black DM, Mitlak BH, et al. Reduction of vertebral fracture risk in postmenopausal women with osteoporosis treated with raloxifene (MORE). JAMA. 1999;282(7):637–645. PMID: 10517716
- Cauley JA, Robbins J, Chen Z, et al. Effects of estrogen plus progestin on risk of fracture and bone mineral density: the Women's Health Initiative randomized trial. JAMA. 2003;290(13):1729–1738. PMID: 14519707
Safety: jaw osteonecrosis and atypical femoral fracture
- Khan AA, Morrison A, Hanley DA, et al. Diagnosis and management of osteonecrosis of the jaw: a systematic review and international consensus. J Bone Miner Res. 2015;30(1):3–23. PMID: 25414052 — ONJ incidence 0.001–0.01% at osteoporosis doses vs 1–15% at oncology doses.
- Black DM, Geiger EJ, Eastell R, et al. Atypical femur fracture risk versus fragility fracture prevention with bisphosphonates. N Engl J Med. 2020;383(8):743–753. PMID: 32813950 — 196,129 women: risk rises with duration and falls rapidly on stopping; ~149 hip fractures prevented per 2 atypical fractures caused in white women.
Exercise, calcium and vitamin D
- Watson SL, Weeks BK, Weis LJ, et al. High-intensity resistance and impact training improves bone mineral density and physical function in postmenopausal women with osteopenia and osteoporosis: the LIFTMOR randomized controlled trial. J Bone Miner Res. 2018;33(2):211–220. PMID: 28975661
- Sherrington C, Fairhall NJ, Wallbank GK, et al. Exercise for preventing falls in older people living in the community. Cochrane Database Syst Rev. 2019;1(1):CD012424. PMID: 30703272 — 108 trials: exercise cuts falls 23%; balance + resistance 34%; tai chi 19%.
- Zhao JG, Zeng XT, Wang J, Liu L. Association between calcium or vitamin D supplementation and fracture incidence in community-dwelling older adults: a systematic review and meta-analysis. JAMA. 2017;318(24):2466–2482. PMID: 29279934 — 33 trials, 51,145 people: no significant fracture reduction.
- LeBoff MS, Chou SH, Ratliff KA, et al. Supplemental vitamin D and incident fractures in midlife and older adults (VITAL). N Engl J Med. 2022;387(4):299–309. PMID: 35939577 — 2,000 IU/day did not reduce fractures in replete adults.
- Chapuy MC, Arlot ME, Duboeuf F, et al. Vitamin D3 and calcium to prevent hip fractures in elderly women. N Engl J Med. 1992;327(23):1637–1642. PMID: 1331788 — the counterpoint: supplementation does work where there is real deficiency.
- Sanders KM, Stuart AL, Williamson EJ, et al. Annual high-dose oral vitamin D and falls and fractures in older women: a randomized controlled trial. JAMA. 2010;303(18):1815–1822. PMID: 20460620 — high intermittent dosing increased falls and fractures.
Live PubMed searches
These links open live PubMed queries, so the result set stays current as new studies are indexed.
- Osteoporosis review
- DEXA bone density diagnosis
- FRAX fracture risk assessment
- Osteopenia fracture burden
- Bisphosphonate osteoporosis trials
- Denosumab rebound after discontinuation
- Romosozumab cardiovascular safety
- Anabolic therapy for osteoporosis
- Atypical femoral fracture
- Osteonecrosis of the jaw incidence
- Glucocorticoid-induced osteoporosis
- Secondary osteoporosis screening
- Resistance exercise and bone density
- Fall prevention in older adults
- Calcium and vitamin D for fracture prevention
- Osteoporosis in men
Connections
- Rheumatology
- Menopause: Why the Hormones Fall and What Changes — interactive animation
- Bone Remodeling & Calcium Balance — interactive animation
- Bisphosphonates
- DEXA Scan: T-Score and Z-Score
- Calcium, Vitamin D and Protein Intake
- FRAX Risk Assessment
- Fracture Prevention and Fall Risk
- Secondary Osteoporosis Causes
- Denosumab, Romosozumab and Teriparatide
- Weight-Bearing and Resistance Exercise
- Postmenopausal Osteoporosis and Hormone Therapy
- History of Osteoporosis
- Hip Fracture
- Stress Fracture
- Paget's Disease of Bone
- Osteonecrosis
- Low Back Pain
- Scoliosis
- Tai Chi (Fall Prevention)
- Prunes (Bone Health)
- Prunes for Bone Health
- Calcium
- Magnesium
- Vitamin D3
- Vitamin K
- Vitamin K2 for Bone Health
- Arthritis
- Menopause and HRT
- Celiac Disease
- Hyperparathyroidism
- Kidney Disease
- Osteoarthritis
- Rheumatoid Arthritis
- Black Cohosh for Bone Health — what the actein and triterpene-glycoside bone data does and does not show.