Vitamin D3 and Bone Health
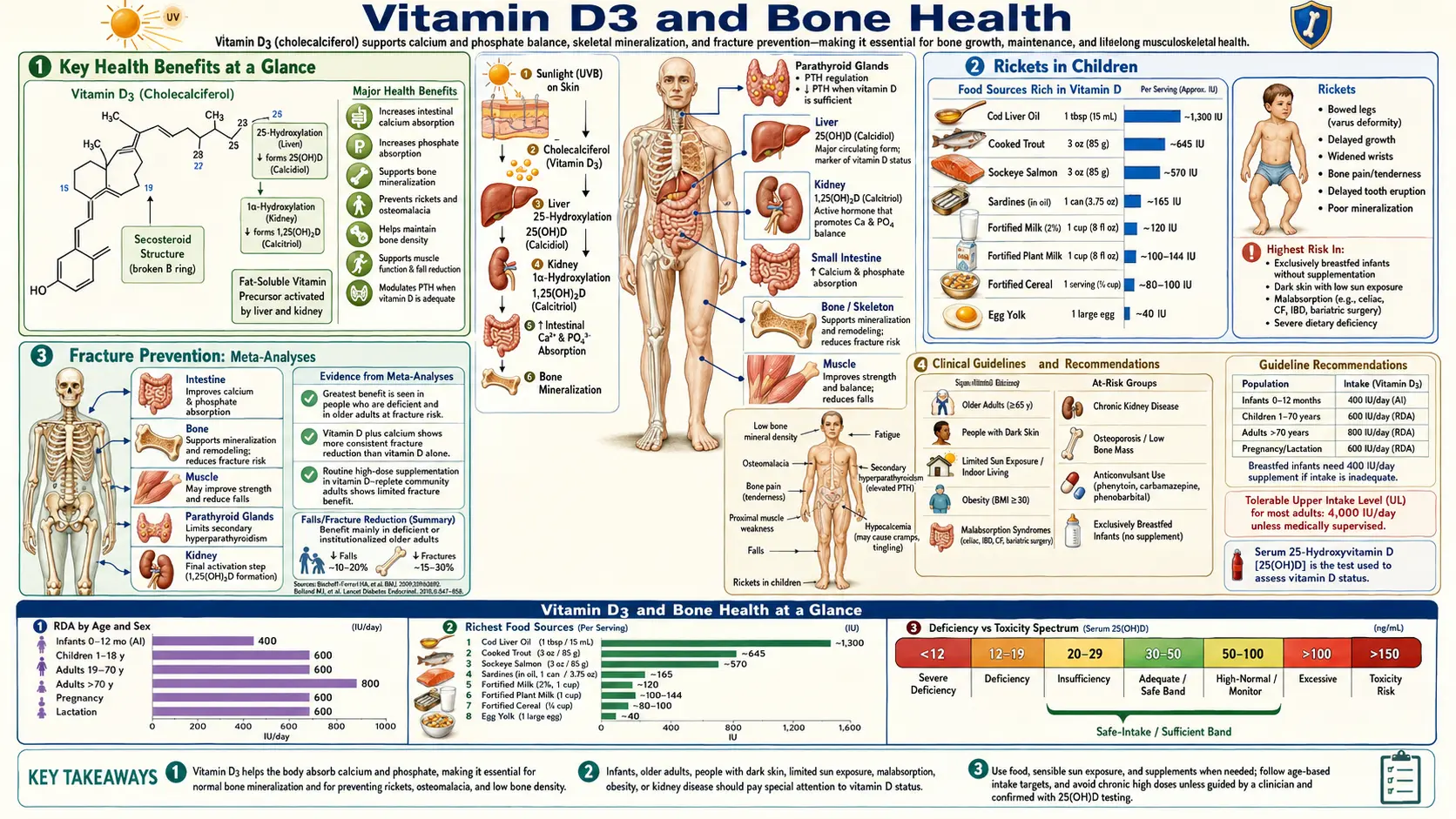
Vitamin D3 (cholecalciferol) is fundamental to skeletal health through its regulation of calcium and phosphorus homeostasis. The active hormonal form, calcitriol (1,25-dihydroxyvitamin D3), controls intestinal mineral absorption, bone mineralization, and parathyroid hormone secretion. Deficiency of vitamin D3 leads to rickets in children, osteomalacia in adults, and contributes to osteoporosis and fracture risk in the elderly. In the absence of adequate vitamin D, calcium absorption efficiency drops from 30–40% to a mere 10–15%, triggering the secondary hyperparathyroidism that drives progressive bone loss.
Table of Contents
- Key Health Benefits at a Glance
- Calcium Absorption Enhancement
- Phosphorus Absorption
- Bone Mineralization and Hydroxyapatite
- Rickets in Children
- Osteomalacia in Adults
- Osteoporosis and Secondary Hyperparathyroidism
- Fracture Prevention: Meta-Analyses
- Fall Prevention in the Elderly
- Optimal 25(OH)D Levels for Bone Health
- Vitamin D3 and Calcium Synergy
- Clinical Guidelines and Recommendations
- Research Papers and References
- Connections
- Featured Videos
Key Health Benefits at a Glance
The following summarizes the evidence-backed bone-health benefits of adequate vitamin D3 status. Each is explored in more depth below, and the supporting studies are linked in the Research Papers section.
- Triples calcium absorption – Calcitriol upregulates TRPV6, calbindin-D9k, and PMCA1b, boosting transcellular calcium uptake from ~10–15% (deficient) to 30–40% (sufficient).
- Prevents rickets and osteomalacia – Adequate vitamin D is required for mineralization of osteoid; deficiency produces classic bowed legs in children (rickets) and diffuse bone pain with proximal weakness in adults (osteomalacia).
- Reduces hip fracture risk by ~26% – Bischoff-Ferrari meta-analysis of 700–800 IU/day of D3 combined with calcium showed a consistent fracture reduction in older adults.
- Reduces falls by ~19–26% – Skeletal muscle expresses VDR; correction of deficiency improves balance, proximal strength, and fall prevention in community-dwelling and institutionalized elderly.
- Suppresses secondary hyperparathyroidism – Serum PTH plateaus at 25(OH)D levels above 30 ng/mL, preventing PTH-driven cortical bone loss.
- Activates calcium-binding osteocalcin – Calcitriol upregulates osteocalcin gene transcription in osteoblasts, a protein that then requires vitamin K2 carboxylation to anchor calcium to hydroxyapatite.
- Supports bone mineral density – Higher 25(OH)D levels correlate with greater BMD at the hip, spine, and total body, particularly in postmenopausal women.
- Essential during pregnancy and infancy – 400 IU/day from the first days of life prevents infantile rickets; maternal sufficiency supports fetal skeletal development.
Calcium Absorption Enhancement
The primary mechanism by which vitamin D3 supports bone health is through the enhancement of intestinal calcium absorption.
- TRPV6 (Transient Receptor Potential Vanilloid 6) – Calcitriol binds to the vitamin D receptor (VDR) in intestinal epithelial cells and upregulates the transcription of the TRPV6 calcium channel gene. TRPV6 channels are located on the apical (luminal) membrane of duodenal enterocytes and serve as the primary gateway for transcellular calcium absorption. In the absence of adequate vitamin D, TRPV6 expression falls dramatically, reducing active calcium transport by 50 to 70 percent.
- Calbindin-D9k – Once calcium enters the enterocyte through TRPV6, it must be shuttled across the cell to the basolateral membrane without triggering calcium-dependent signaling cascades or toxicity. Calbindin-D9k, a vitamin D-dependent calcium-binding protein, fulfills this role. Each calbindin molecule can bind two calcium ions and ferry them through the cytoplasm. Calcitriol upregulates calbindin-D9k expression by 10- to 100-fold, proportionally increasing the calcium transport capacity of the intestine.
- PMCA1b (Plasma Membrane Calcium ATPase) – At the basolateral membrane, calcium is extruded into the interstitial fluid and bloodstream by PMCA1b, an ATP-dependent calcium pump also upregulated by vitamin D. This completes the transcellular calcium absorption pathway: TRPV6 (entry) to calbindin (transport) to PMCA1b (export).
- Magnitude of Effect – In the vitamin D-sufficient state, approximately 30 to 40 percent of dietary calcium is absorbed. In vitamin D deficiency, absorption efficiency drops to 10 to 15 percent. This difference is the primary driver of the secondary hyperparathyroidism and bone loss seen in vitamin D-deficient individuals.
- Paracellular Absorption – In addition to the transcellular pathway, vitamin D may enhance paracellular calcium absorption (passive diffusion between cells) by modulating tight junction proteins such as claudin-2 and claudin-12. This pathway becomes significant when luminal calcium concentrations are high, as after consumption of a calcium-rich meal.
Phosphorus Absorption
- NaPi-IIb Transporter – Calcitriol upregulates the expression of the sodium-dependent phosphate transporter NaPi-IIb (SLC34A2) in the small intestine. This transporter is the primary mechanism for active phosphorus absorption. Vitamin D deficiency reduces phosphorus absorption efficiency, compounding the mineral deficit that impairs bone formation.
- Calcium-Phosphorus Balance – Both calcium and phosphorus are required in a specific ratio for hydroxyapatite crystal formation. Vitamin D ensures adequate supply of both minerals by simultaneously enhancing their intestinal absorption. The optimal serum calcium-phosphorus product for bone mineralization is maintained through coordinated vitamin D-dependent regulation of both minerals.
- FGF23 Interaction – Fibroblast growth factor 23 (FGF23), produced by osteocytes, acts as a counter-regulatory hormone that reduces phosphorus levels when they are too high. FGF23 suppresses renal 1-alpha-hydroxylase (reducing calcitriol production) and increases renal phosphorus excretion. The vitamin D-FGF23 axis maintains phosphorus within the narrow range required for safe and effective bone mineralization.
Bone Mineralization and Hydroxyapatite
- Hydroxyapatite Formation – Bone mineralization involves the deposition of hydroxyapatite crystals [Ca10(PO4)6(OH)2] onto the collagen matrix produced by osteoblasts. This process requires adequate local concentrations of calcium and phosphorus ions, which are maintained by vitamin D-dependent intestinal absorption and renal reabsorption.
- Osteoblast Function – Calcitriol acts directly on osteoblasts through the VDR, stimulating the production of osteocalcin (a calcium-binding protein that guides hydroxyapatite deposition) and alkaline phosphatase (which releases phosphate from organic substrates at the mineralization front). Vitamin D also induces RANKL expression on osteoblasts, which is essential for osteoclast differentiation and the coupled bone remodeling process.
- Mineralization Lag Time – In normal bone, newly formed osteoid (unmineralized collagen matrix) undergoes mineralization within 5 to 10 days. In vitamin D deficiency, the mineralization lag time increases dramatically as insufficient calcium and phosphorus are available, leading to accumulation of unmineralized osteoid, the defining feature of osteomalacia.
Rickets in Children
- Pathophysiology – Rickets occurs when vitamin D deficiency during childhood prevents adequate mineralization of growing bone and the cartilaginous growth plates. The growth plate widens as chondrocytes proliferate but fail to undergo normal calcification and apoptosis, producing the characteristic rachitic changes.
- Clinical Features – Classic signs include bowing of the legs (genu varum), widening of the wrists and ankles (metaphyseal flaring), frontal bossing of the skull, delayed closure of fontanelles, rachitic rosary (beading of the costochondral junctions), Harrison's sulcus (indentation of the lower rib cage), and delayed motor development. Severe cases may present with hypocalcemic seizures in infancy.
- Resurgence – Despite being considered a disease of the past, rickets has resurged in developed countries due to increased sun avoidance, exclusive breastfeeding without vitamin D supplementation (breast milk contains only 20 to 80 IU per liter), darker skin pigmentation at northern latitudes, and obesity (vitamin D sequestration in adipose tissue).
- Prevention – The American Academy of Pediatrics recommends 400 IU of vitamin D daily for all breastfed infants, beginning within the first few days of life. Formula-fed infants receiving at least 1 liter of vitamin D-fortified formula daily do not require additional supplementation.
Osteomalacia in Adults
- Definition – Osteomalacia is the adult equivalent of rickets, characterized by defective mineralization of newly formed osteoid in mature bone. Unlike osteoporosis, which involves loss of both mineral and matrix, osteomalacia specifically involves adequate matrix production with inadequate mineralization.
- Symptoms – Diffuse bone pain (often mistaken for fibromyalgia or depression), proximal muscle weakness (difficulty climbing stairs, rising from chairs), waddling gait, and increased fracture susceptibility. Bone pain is characteristically worse with weight-bearing and may be elicited by pressing on the sternum or tibia.
- Diagnosis – Laboratory findings include low or low-normal calcium, low phosphorus, elevated alkaline phosphatase, elevated PTH, and very low 25(OH)D levels (typically below 10 ng/mL). Definitive diagnosis requires bone biopsy with tetracycline double-labeling showing increased osteoid thickness and prolonged mineralization lag time, though this is rarely performed clinically.
- Looser Zones – Radiographic pseudo-fractures (Looser zones or Milkman fractures) are bands of unmineralized osteoid that appear as radiolucent lines, typically in the femoral neck, pubic rami, scapulae, and ribs. These are pathognomonic for osteomalacia.
Osteoporosis and Secondary Hyperparathyroidism
- Mechanism – When vitamin D deficiency reduces intestinal calcium absorption, serum ionized calcium falls, triggering increased parathyroid hormone (PTH) secretion. Elevated PTH maintains serum calcium by stimulating osteoclastic bone resorption, releasing calcium from the skeleton. This secondary hyperparathyroidism accelerates bone loss, particularly from cortical bone, increasing fracture risk.
- PTH Threshold – Studies consistently show that PTH levels begin to rise when 25(OH)D falls below 30 ng/mL (75 nmol/L), and rise steeply below 20 ng/mL. This PTH-25(OH)D relationship is a key argument for defining vitamin D sufficiency at 30 ng/mL or above.
- Cortical vs. Trabecular Bone – PTH-driven bone resorption preferentially affects cortical bone (the dense outer shell of long bones), increasing the risk of appendicular fractures (hip, wrist). However, prolonged vitamin D deficiency also reduces trabecular bone density in the vertebral bodies, contributing to spinal compression fractures.
- Prevalence – Secondary hyperparathyroidism due to vitamin D deficiency is extremely common, particularly in the elderly. Studies of hip fracture patients consistently find that 50 to 80 percent have vitamin D deficiency, and the majority have biochemical evidence of secondary hyperparathyroidism.
Fracture Prevention: Meta-Analyses
- Hip Fracture Reduction – A meta-analysis by Bischoff-Ferrari et al. found that vitamin D supplementation at doses of 700 to 800 IU daily reduced hip fracture risk by 26 percent compared to placebo or calcium alone. Doses below 400 IU daily did not show significant fracture reduction, suggesting a threshold effect.
- Non-Vertebral Fractures – The same analysis found a 23 percent reduction in non-vertebral fractures with 700 to 800 IU daily of vitamin D. The achieved 25(OH)D level appeared more important than the dose itself, with fracture reduction greatest in those reaching levels above 30 ng/mL.
- VITAL Study Bone Substudy – The large VITAL randomized trial (25,871 participants, Manson et al. 2019) found that supplementation with 2,000 IU daily of vitamin D3 did not reduce fracture risk in the overall population of generally vitamin D-replete adults. This finding underscored that fracture prevention benefits are concentrated in those who are vitamin D deficient at baseline.
- Dose Considerations – Very high intermittent doses (annual bolus of 500,000 IU or monthly doses of 60,000 IU) have paradoxically increased fall and fracture risk in some trials, possibly through rapid fluctuations in calcitriol and its effects on muscle function. Current evidence favors moderate daily dosing (800 to 2,000 IU) over infrequent large boluses.
- Weaver Meta-Analysis – The Weaver et al. (2016) updated meta-analysis of calcium-plus-vitamin D trials reported a 15% reduction in total fractures and a 30% reduction in hip fractures with combined supplementation versus placebo, reinforcing the importance of combining both nutrients.
Fall Prevention in the Elderly
- Muscle VDR Expression – Skeletal muscle cells express the VDR, and calcitriol directly influences muscle protein synthesis, muscle fiber composition, and neuromuscular coordination. Vitamin D deficiency is associated with type II (fast-twitch) muscle fiber atrophy, which impairs balance and the ability to prevent falls.
- Meta-Analysis Evidence – A Cochrane review and subsequent meta-analyses have found that vitamin D supplementation (700 to 1,000 IU daily) reduces fall risk by approximately 19 to 26 percent in community-dwelling older adults and institutionalized elderly. The benefit is most pronounced in those with baseline 25(OH)D levels below 20 ng/mL.
- Combined with Exercise – The fall prevention benefit of vitamin D is enhanced when combined with exercise programs (particularly balance and strength training). Multifactorial fall prevention programs that include vitamin D supplementation show the greatest reductions in fall rates.
- Institutionalized Populations – Nursing home residents are at particularly high risk for both vitamin D deficiency and falls. Supplementation with vitamin D3 (800 IU daily) plus calcium (1,000 to 1,200 mg daily) is considered standard of care in many geriatric guidelines.
Optimal 25(OH)D Levels for Bone Health
- Deficiency – 25(OH)D levels below 12 ng/mL (30 nmol/L) are associated with rickets, osteomalacia, and severely impaired calcium absorption. This represents frank vitamin D deficiency requiring treatment.
- Insufficiency – Levels between 12 and 20 ng/mL (30 to 50 nmol/L) are considered insufficient by most guidelines. Secondary hyperparathyroidism is common in this range, and bone mineral density is suboptimal.
- Sufficiency – The Institute of Medicine defines sufficiency as 20 ng/mL or above, while the Endocrine Society recommends 30 ng/mL or above. The latter target is based on the observation that PTH levels plateau and calcium absorption is maximized at 25(OH)D levels above 30 ng/mL.
- Optimal Range – Many bone health experts recommend maintaining 25(OH)D between 30 and 50 ng/mL (75 to 125 nmol/L) for optimal skeletal outcomes. Levels above 50 ng/mL have not shown additional bone benefits and may be associated with increased risk at levels exceeding 60 to 80 ng/mL.
- Testing – The 25(OH)D blood test is the standard measure of vitamin D status, reflecting both dietary intake and cutaneous synthesis. It should be measured by reliable assay methods (LC-MS/MS is the gold standard) and interpreted in the context of PTH, calcium, and phosphorus levels.
Vitamin D3 and Calcium Synergy
- Combined Supplementation – The strongest evidence for fracture prevention comes from trials using vitamin D combined with calcium, rather than either nutrient alone. The combination ensures both adequate mineral supply and the vitamin D-dependent transport mechanisms needed to absorb and utilize that calcium.
- Recommended Calcium Intake – Adults aged 19 to 50 require 1,000 mg of calcium daily; women over 50 and men over 70 require 1,200 mg daily. Dietary sources (dairy products, fortified plant milks, leafy greens, canned fish with bones) are preferred over supplements when possible.
- Safety of Calcium Supplements – Some meta-analyses have raised concerns about cardiovascular risk with calcium supplementation (particularly without vitamin D). Current guidelines generally recommend meeting calcium needs through diet when possible and limiting supplemental calcium to 500 to 600 mg per dose for optimal absorption.
Clinical Guidelines and Recommendations
- Daily Supplementation Doses – The IOM recommends 600 IU daily for adults aged 1 to 70 and 800 IU daily for adults over 70. The Endocrine Society recommends 1,500 to 2,000 IU daily for adults at risk of deficiency. Many clinical experts recommend 1,000 to 2,000 IU daily as a safe and effective maintenance dose for most adults.
- Treatment of Deficiency – For documented vitamin D deficiency (25(OH)D below 20 ng/mL), a common treatment protocol is 50,000 IU of vitamin D2 or D3 weekly for 8 to 12 weeks, followed by a maintenance dose of 1,000 to 2,000 IU daily. Vitamin D3 is preferred over D2 for its superior potency and longer duration of action.
- Tolerable Upper Intake – The IOM sets the tolerable upper intake level at 4,000 IU daily for adults, while the Endocrine Society considers up to 10,000 IU daily safe for short-term use. Vitamin D toxicity (hypercalcemia) is rare at doses below 10,000 IU daily and typically occurs only with sustained intake exceeding 40,000 IU daily or with 25(OH)D levels above 150 ng/mL.
- High-Risk Groups – Individuals at greatest risk for vitamin D deficiency include the elderly (reduced skin synthesis capacity), those with dark skin pigmentation (melanin reduces UVB absorption), obese individuals (sequestration in adipose tissue), those with malabsorption syndromes (celiac disease, inflammatory bowel disease, bariatric surgery), and people living at high latitudes or with minimal sun exposure.
This content is provided for informational purposes only and does not constitute medical advice. Consult a qualified healthcare provider before beginning any supplementation regimen, especially if you have kidney disease, granulomatous disease, or are taking thiazide diuretics.
Research Papers and References
The following are landmark and frequently cited research papers underpinning the claims on this page. Links resolve to the publisher DOI or PubMed record.
Foundational Reviews
- Holick MF. Vitamin D deficiency. New England Journal of Medicine. 2007;357(3):266-281.
- Bikle DD. Vitamin D metabolism, mechanism of action, and clinical applications. Chemistry & Biology. 2014;21(3):319-329.
Fracture Prevention and Bone Density
- Weaver CM, Alexander DD, Boushey CJ, et al. Calcium plus vitamin D supplementation and risk of fractures: an updated meta-analysis from the National Osteoporosis Foundation. Osteoporosis International. 2016;27(1):367-376.
- Manson JE, Cook NR, Lee IM, et al. Vitamin D supplements and prevention of cancer and cardiovascular disease (VITAL). New England Journal of Medicine. 2019;380(1):33-44.
- Bischoff-Ferrari HA et al. Fracture prevention with vitamin D supplementation: meta-analysis of randomized controlled trials. PubMed search.
Rickets, Osteomalacia, and Mineralization
- PubMed topic search – Rickets and vitamin D deficiency in children.
- PubMed topic search – Osteomalacia and vitamin D in adults.
Falls and Muscle Function
External Authoritative Resources
- NIH Office of Dietary Supplements — Vitamin D Fact Sheet for Health Professionals
- Linus Pauling Institute — Vitamin D
- Harvard T.H. Chan School of Public Health — The Nutrition Source: Vitamin D
Connections
- All Vitamins
- Vitamin D3
- Calcium
- Phosphorus
- Osteoporosis
- Vitamin D3 and Immune System
- Vitamin D3 and Cancer Prevention
- Magnesium
- Vitamin D Test
- Vitamin K2 and Bone Health
- Vitamin K2 and Arterial Calcification
- Vitamin K
- Collagen
- Hyperparathyroidism
- Milk