Vitamin D Test (25-Hydroxyvitamin D)
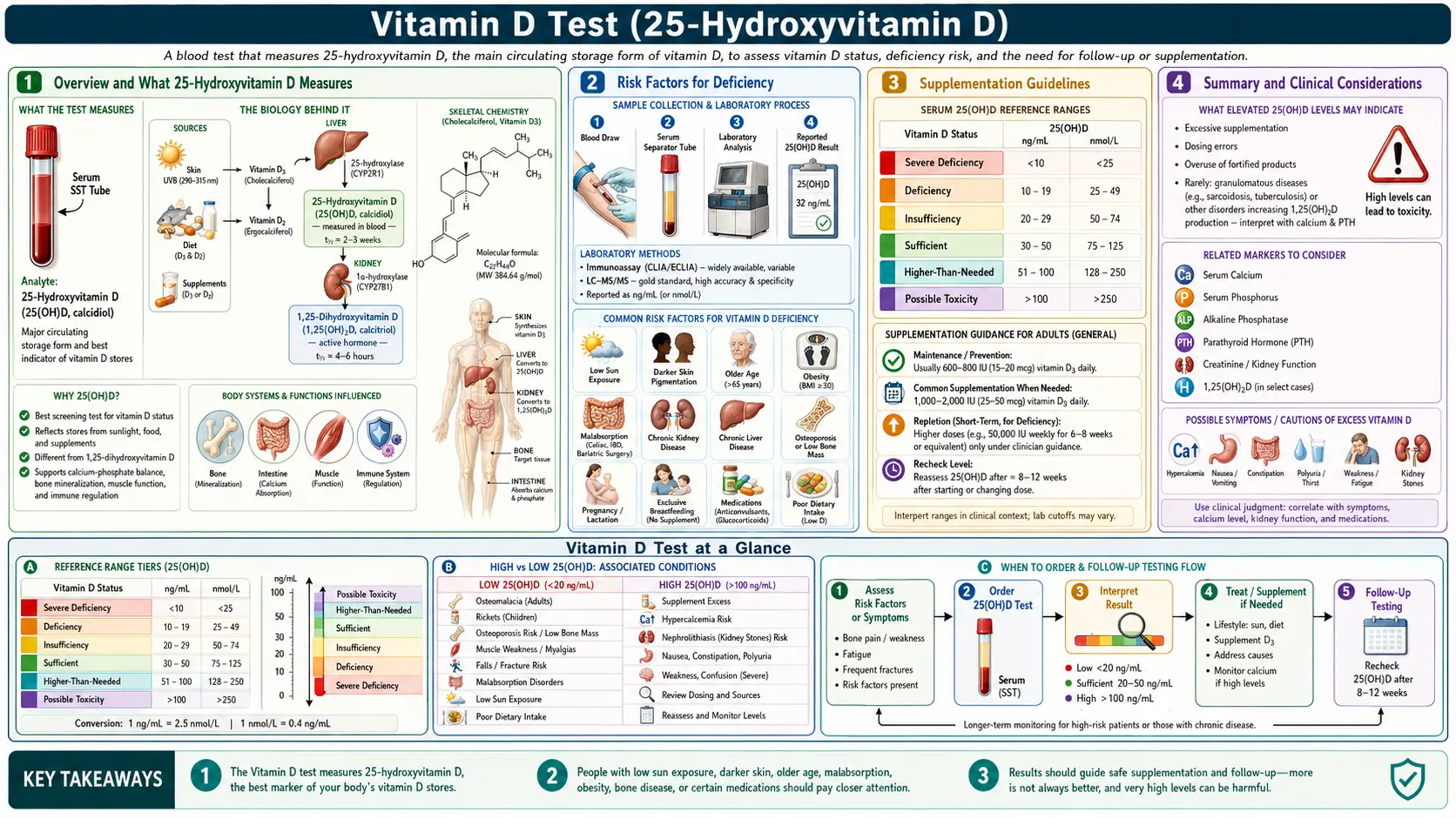
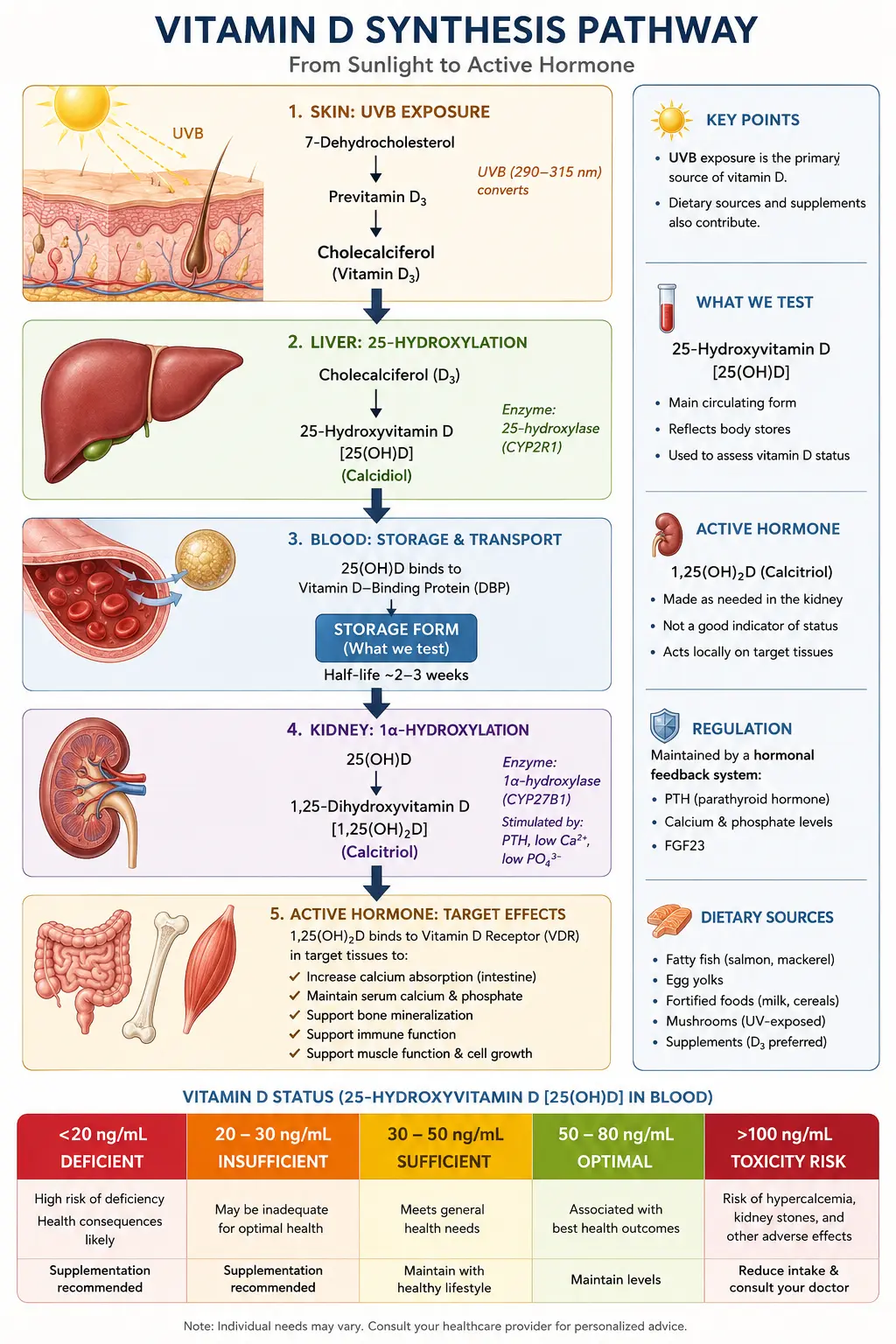
Table of Contents
- Overview and What 25-Hydroxyvitamin D Measures
- Why Vitamin D Is Tested
- How Vitamin D Works in the Body
- Conventional vs Functional Optimal Reference Ranges
- Deficiency Classification Levels
- Wide-Reaching Roles of Vitamin D
- Risk Factors for Deficiency
- Vitamin D3 vs Vitamin D2
- Essential Cofactors for Vitamin D Utilization
- Testing Frequency Recommendations
- Supplementation Guidelines
- Sun Exposure Recommendations
- Dietary Food Sources
- Toxicity Considerations
- Related Laboratory Tests
- Summary and Clinical Considerations
- Featured Videos
Overview and What 25-Hydroxyvitamin D Measures
The vitamin D test, formally known as the 25-hydroxyvitamin D (25(OH)D) test, is the single most important blood marker for assessing your vitamin D status. This test measures the storage form of vitamin D circulating in your bloodstream, which represents the cumulative result of sun exposure, dietary intake, and supplementation over the preceding two to three months.
When vitamin D enters the body, whether produced in the skin from sunlight or consumed through food and supplements, it first travels to the liver where it is converted into 25-hydroxyvitamin D. This is the predominant circulating form and has a half-life of approximately two to three weeks, making it the most reliable indicator of overall vitamin D stores. It is important to distinguish this from the active hormonal form, 1,25-dihydroxyvitamin D (calcitriol), which is produced in the kidneys and has a much shorter half-life of only a few hours. While calcitriol is the biologically active form, testing it does not accurately reflect total body vitamin D status because the body tightly regulates its production, and levels may appear normal even when stores are severely depleted.
From a functional medicine perspective, we consider vitamin D not merely a vitamin but a prohormone with receptors found in virtually every tissue of the body. This distinction is critical because it underscores why adequate vitamin D levels influence far more than just calcium absorption and bone health.
Why Vitamin D Is Tested
Vitamin D deficiency is widely regarded as the most common nutritional deficiency worldwide. Studies estimate that approximately one billion people globally have inadequate vitamin D levels, with some researchers suggesting that up to 40-50% of the general population in industrialized nations is deficient. This pandemic of deficiency is driven by modern indoor lifestyles, widespread sunscreen use, geographic latitude, and dietary patterns that provide insufficient amounts of this critical nutrient.
Testing is recommended for a wide range of clinical scenarios, including:
- Unexplained fatigue and low energy that does not respond to adequate sleep
- Bone pain, muscle weakness, or frequent fractures
- Depression, seasonal affective disorder, or mood disturbances
- Frequent infections or prolonged illness recovery suggesting immune compromise
- Autoimmune conditions such as multiple sclerosis, rheumatoid arthritis, lupus, or Hashimoto thyroiditis
- Cardiovascular concerns including hypertension and heart disease risk
- Cancer screening and prevention protocols
- Osteoporosis or osteopenia, particularly in postmenopausal women
- Chronic pain syndromes including fibromyalgia
- Insulin resistance, metabolic syndrome, or type 2 diabetes
In functional medicine practice, we consider the 25(OH)D test to be a foundational lab marker that should be included in every comprehensive wellness panel, regardless of whether symptoms are present. Given the ubiquity of deficiency and the profound consequences of suboptimal levels, screening is both cost-effective and clinically prudent.
How Vitamin D Works in the Body
Understanding the biochemistry of vitamin D helps explain why deficiency has such far-reaching consequences. Vitamin D metabolism occurs in a three-step process involving the skin, liver, and kidneys.
Step 1: Sunlight Conversion in the Skin
When ultraviolet B (UVB) radiation from sunlight strikes the skin, it converts a cholesterol precursor called 7-dehydrocholesterol into previtamin D3, which is then thermally isomerized into cholecalciferol (vitamin D3). This is the body's primary natural mechanism for obtaining vitamin D. The efficiency of this process depends on the angle of the sun, skin pigmentation, age, and the amount of skin exposed. Importantly, the body has a built-in regulatory mechanism: excessive sun exposure does not cause vitamin D toxicity because previtamin D3 is also photodegraded into inactive compounds.
Step 2: Liver Hydroxylation
Whether obtained from sunlight, food, or supplements, vitamin D3 (or D2 from plant sources) travels via the bloodstream to the liver, where the enzyme 25-hydroxylase converts it into 25-hydroxyvitamin D (calcidiol). This is the form measured by the standard blood test and represents the body's stored reserve of vitamin D. This conversion is largely substrate-driven, meaning the more vitamin D entering the liver, the more 25(OH)D is produced.
Step 3: Kidney Activation
The final activation step occurs primarily in the kidneys, where the enzyme 1-alpha-hydroxylase converts 25(OH)D into 1,25-dihydroxyvitamin D (calcitriol), the biologically active hormonal form. This step is tightly regulated by parathyroid hormone (PTH), calcium levels, and phosphorus levels. However, many other tissues throughout the body, including immune cells, breast tissue, prostate cells, and colon cells, also possess 1-alpha-hydroxylase and can produce calcitriol locally for autocrine and paracrine functions, which is why adequate circulating 25(OH)D is essential for whole-body health.
Conventional vs Functional Optimal Reference Ranges
One of the most significant areas of disagreement between conventional and functional medicine lies in what constitutes an adequate vitamin D level. The standard laboratory reference range and the functional optimal range differ substantially.
Conventional Reference Ranges
- Deficient: Below 20 ng/mL (50 nmol/L)
- Insufficient: 20-29 ng/mL (50-72 nmol/L)
- Sufficient: 30-100 ng/mL (75-250 nmol/L)
These conventional ranges are primarily based on the level needed to prevent rickets in children and osteomalacia in adults, representing the bare minimum for skeletal health rather than the level associated with optimal overall wellness.
Functional Optimal Ranges
- Suboptimal: Below 50 ng/mL (125 nmol/L)
- Optimal: 50-80 ng/mL (125-200 nmol/L)
- Acceptable upper range: 80-100 ng/mL (200-250 nmol/L)
Most functional medicine and naturopathic practitioners target a range of 50-80 ng/mL for their patients. This target is based on extensive research showing that populations with abundant sun exposure, such as outdoor workers in equatorial regions and the Maasai of East Africa, naturally maintain levels in the 40-80 ng/mL range. Furthermore, the preponderance of research on cancer prevention, immune optimization, cardiovascular protection, and autoimmune disease risk reduction shows the most benefit at levels above 50 ng/mL.
It is worth noting that a patient with a level of 31 ng/mL would be considered "sufficient" by conventional standards yet would be regarded as significantly suboptimal by functional medicine criteria. This discrepancy has profound clinical implications for patient outcomes.
Deficiency Classification Levels
A more detailed stratification of vitamin D status, incorporating both conventional and functional perspectives, is as follows:
- Severe Deficiency: Below 20 ng/mL - Associated with rickets in children, osteomalacia in adults, significant immune suppression, increased infection susceptibility, elevated cancer risk, and markedly increased all-cause mortality. This level demands immediate and aggressive repletion.
- Insufficiency: 20-30 ng/mL - Frequently seen in clinical practice. Patients often present with fatigue, bone pain, muscle weakness, mood disturbances, and frequent respiratory infections. Supplementation is warranted with follow-up testing in 8-12 weeks.
- Conventional Sufficiency but Functional Suboptimal: 30-50 ng/mL - While conventional labs may flag this as "normal," from a functional perspective, the body is not receiving adequate vitamin D for optimal immune function, cancer prevention, and chronic disease protection. Moderate supplementation is recommended to reach the 50-80 ng/mL target.
- Functional Optimal: 50-80 ng/mL - This is the therapeutic target. Research consistently demonstrates that this range is associated with the lowest risk of cancer, autoimmune disease, cardiovascular events, infections, depression, and all-cause mortality.
- Excess: Above 100 ng/mL - While not immediately dangerous, levels above 100 ng/mL warrant investigation and potential dose reduction. Clinical toxicity typically does not manifest until levels exceed 150 ng/mL, but sustained levels above 100 ng/mL may increase calcium-related complications.
Wide-Reaching Roles of Vitamin D
Vitamin D receptors (VDRs) have been identified in nearly every cell type in the human body, and vitamin D influences the expression of over 1,000 genes. This broad influence explains why deficiency is linked to such a diverse array of health conditions.
Immune Function
Vitamin D is a critical modulator of both the innate and adaptive immune systems. It enhances the production of antimicrobial peptides such as cathelicidin and defensins, which are the body's first line of defense against bacterial, viral, and fungal pathogens. Vitamin D also regulates T-cell and B-cell function, promoting immune tolerance and reducing the risk of autoimmune activation. Research has demonstrated that individuals with optimal vitamin D levels experience significantly fewer respiratory tract infections, including influenza and pneumonia.
Bone Health
The classical role of vitamin D is facilitating calcium and phosphorus absorption from the intestines, which is essential for bone mineralization. Without adequate vitamin D, the body absorbs only 10-15% of dietary calcium compared to 30-40% when vitamin D is sufficient. Chronic deficiency leads to secondary hyperparathyroidism, accelerated bone resorption, and ultimately osteoporosis and fracture risk.
Cancer Prevention
A substantial body of evidence links vitamin D sufficiency to reduced risk of several cancers, including colorectal, breast, prostate, pancreatic, and ovarian cancers. Vitamin D promotes cellular differentiation, inhibits uncontrolled proliferation, stimulates apoptosis (programmed cell death) in damaged cells, and reduces angiogenesis (new blood vessel formation in tumors). The Grassroots Health research consortium has shown that maintaining a level of 60 ng/mL or above is associated with an 80% reduction in breast cancer incidence compared to levels below 20 ng/mL.
Mood and Mental Health
Vitamin D receptors are abundant in brain regions associated with mood regulation, including the hippocampus, prefrontal cortex, and hypothalamus. Deficiency is strongly correlated with depression, seasonal affective disorder (SAD), anxiety, and cognitive decline. Vitamin D influences serotonin synthesis, and supplementation has been shown to improve depressive symptoms in deficient individuals.
Cardiovascular Health
Vitamin D plays a role in regulating blood pressure through its influence on the renin-angiotensin-aldosterone system. Deficiency is associated with hypertension, endothelial dysfunction, arterial stiffness, and increased risk of heart attack and stroke. Optimal levels support vascular smooth muscle function and help reduce systemic inflammation, a key driver of atherosclerosis.
Autoimmune Disease
Vitamin D is one of the most powerful natural immunomodulators available. It promotes regulatory T-cell development, which is essential for preventing the immune system from attacking the body's own tissues. Low vitamin D levels are consistently observed in patients with multiple sclerosis, type 1 diabetes, rheumatoid arthritis, lupus, inflammatory bowel disease, and Hashimoto thyroiditis. Supplementation to optimal levels is a cornerstone of autoimmune management protocols in functional medicine.
Risk Factors for Deficiency
Understanding who is at greatest risk for vitamin D deficiency is essential for targeted screening and prevention. The following factors significantly increase the likelihood of inadequate vitamin D levels:
- Geographic Latitude: Individuals living above the 37th parallel north (or below the 37th parallel south) cannot produce sufficient vitamin D from sunlight during the winter months because UVB rays are too weak at steep angles. In many northern regions, the "vitamin D winter" can last from October through April.
- Skin Pigmentation: Melanin, the pigment responsible for darker skin tones, acts as a natural sunscreen that reduces UVB penetration. Individuals with darker skin may require 3-10 times more sun exposure to produce the same amount of vitamin D as those with lighter skin. This is a significant contributor to the higher rates of vitamin D deficiency observed in Black and Hispanic populations.
- Aging: The skin's capacity to synthesize vitamin D decreases substantially with age. A 70-year-old produces approximately 75% less vitamin D from the same sun exposure as a 20-year-old. Additionally, kidney function declines with age, reducing the conversion of 25(OH)D to the active form.
- Obesity: Vitamin D is fat-soluble and becomes sequestered in adipose tissue, effectively reducing its bioavailability. Obese individuals (BMI above 30) typically require 2-3 times the standard supplementation dose to achieve optimal levels.
- Indoor Lifestyle: The modern tendency to spend the vast majority of time indoors, whether for work, school, or recreation, dramatically limits UVB exposure. Office workers, students, and those with sedentary lifestyles are at particularly high risk.
- Sunscreen Use: While sunscreen protects against skin damage, SPF 30 reduces the skin's vitamin D production by approximately 97%. The blanket recommendation to always wear sunscreen has inadvertently contributed to the vitamin D deficiency epidemic.
- Gut Malabsorption: Conditions such as celiac disease, Crohn disease, ulcerative colitis, and small intestinal bacterial overgrowth (SIBO) impair fat absorption and consequently vitamin D absorption.
- Medications: Certain drugs including glucocorticoids, anticonvulsants, antifungals, and cholestyramine can interfere with vitamin D metabolism or absorption.
- Kidney and Liver Disease: Impaired organ function reduces the body's ability to convert vitamin D into its active forms.
Vitamin D3 vs Vitamin D2
Not all forms of supplemental vitamin D are created equal. Understanding the difference between D3 and D2 is essential for effective repletion.
Vitamin D3 (Cholecalciferol)
Vitamin D3 is the form naturally produced in human skin upon UVB exposure and is also found in animal-based food sources such as fatty fish, egg yolks, and cod liver oil. It is the preferred form for supplementation because research consistently demonstrates that D3 is approximately 87% more effective at raising and maintaining serum 25(OH)D levels compared to D2. Vitamin D3 also has a longer duration of action and produces a more stable, sustained rise in blood levels.
Vitamin D2 (Ergocalciferol)
Vitamin D2 is derived from plant and fungal sources, produced when ergosterol in fungi is exposed to UVB radiation. It is commonly found in prescription vitamin D supplements and fortified foods. While D2 can raise 25(OH)D levels, it does so less effectively than D3, has a shorter shelf life, is metabolized differently, and produces metabolites that may be less biologically active. Most naturopathic and functional medicine practitioners do not recommend D2 except for patients who require a strictly plant-based form.
For vegan patients who prefer a non-animal source, vitamin D3 derived from lichen is now widely available and provides the superior D3 form without animal-sourced ingredients.
Essential Cofactors for Vitamin D Utilization
Vitamin D does not work in isolation. Several key nutrients are required as cofactors for vitamin D to be properly metabolized and to exert its biological effects safely and effectively. Supplementing vitamin D without attention to these cofactors can lead to suboptimal results or even adverse effects.
Vitamin K2
Vitamin K2 is arguably the most critical cofactor for vitamin D supplementation. Vitamin D increases calcium absorption from the gut, but it is vitamin K2 that directs where that calcium goes. K2 activates osteocalcin, which deposits calcium into bones and teeth, and activates matrix Gla protein (MGP), which prevents calcium from depositing in arteries, kidneys, and soft tissues. Without adequate K2, higher vitamin D levels may paradoxically increase the risk of arterial calcification. The recommended form is MK-7 (menaquinone-7) at a dose of 100-200 mcg daily alongside vitamin D supplementation.
Magnesium
Magnesium is required at multiple steps of vitamin D metabolism. It is a necessary cofactor for the enzymes that convert vitamin D to 25(OH)D in the liver and to 1,25(OH)2D in the kidneys. Without sufficient magnesium, vitamin D remains stored and inactive. Studies have shown that magnesium supplementation alone can raise 25(OH)D levels in deficient individuals, even without additional vitamin D. Common forms include magnesium glycinate, threonate, or malate at doses of 200-400 mg elemental magnesium daily.
Boron
The trace mineral boron extends the half-life of 25(OH)D in the blood, effectively making your vitamin D last longer. Boron also supports the conversion of vitamin D to its active form and enhances the beneficial effects of vitamin D on calcium and magnesium metabolism. A typical supplemental dose is 3-6 mg daily.
Zinc
Zinc is involved in the function of the vitamin D receptor. Without adequate zinc, vitamin D cannot properly bind to its receptor and activate gene transcription. Zinc deficiency is common and may contribute to apparent vitamin D resistance in some patients.
Testing Frequency Recommendations
The frequency of vitamin D testing depends on the clinical context, baseline levels, and whether the patient is actively repleting a deficiency or maintaining optimal levels.
- Initial Baseline Testing: Every new patient should have a baseline 25(OH)D level drawn as part of their initial comprehensive evaluation.
- During Active Repletion: When correcting a deficiency, recheck levels every 8-12 weeks. It takes approximately 2-3 months for supplementation to fully reflect in serum levels due to the half-life of 25(OH)D.
- After Reaching Optimal Levels: Once a patient achieves the target range of 50-80 ng/mL, testing every 6 months is generally sufficient to confirm maintenance.
- Annual Monitoring: For stable patients on a consistent maintenance dose, annual testing is reasonable, ideally measured in late winter (February-March) when levels are at their nadir and again in late summer (August-September) when they peak.
- Seasonal Considerations: Levels can fluctuate significantly between summer and winter, sometimes by 20-30 ng/mL or more. Patients should understand that their summer maintenance dose may need to be increased during winter months.
Supplementation Guidelines
Supplementation protocols should be individualized based on current serum levels, body weight, absorption capacity, and the specific health goals of the patient. The following are general guidelines used in naturopathic and functional medicine practice.
Repletion Dosing for Deficiency (below 30 ng/mL)
- Adults: 5,000-10,000 IU of vitamin D3 daily for 8-12 weeks, then retest
- Some protocols use a loading dose: 50,000 IU once weekly for 8 weeks
- Obese individuals: May require 2-3 times the standard dose due to sequestration in adipose tissue
Maintenance Dosing (levels 50-80 ng/mL)
- Adults: 2,000-5,000 IU daily, adjusted based on individual response and seasonal variation
- A general rule of thumb: Every 1,000 IU of vitamin D3 supplementation raises serum 25(OH)D by approximately 10 ng/mL in a normal-weight individual, though individual responses vary considerably
Pediatric Dosing
- Infants (0-12 months): 400-1,000 IU daily
- Children (1-12 years): 1,000-2,000 IU daily
- Adolescents: 2,000-4,000 IU daily
Best Practices for Supplementation
- Take vitamin D3 with a fat-containing meal to enhance absorption, as it is a fat-soluble vitamin
- Always co-supplement with vitamin K2 (MK-7) and ensure adequate magnesium intake
- Choose vitamin D3 in an oil-based softgel or liquid form for superior absorption over dry tablets
- Take in the morning or midday rather than evening, as some evidence suggests evening dosing may interfere with melatonin production
- For patients with malabsorption issues, consider sublingual or emulsified forms that bypass gut absorption
Sun Exposure Recommendations
Sunlight remains the most natural and effective way to maintain vitamin D levels. From a naturopathic perspective, sensible sun exposure is encouraged as a primary strategy, with supplementation serving as an adjunct when sun exposure is insufficient.
- Duration: Aim for 10-30 minutes of midday sun exposure (between 10 AM and 3 PM) on a large area of skin (arms, legs, back) without sunscreen, several times per week. Lighter-skinned individuals need less time; darker-skinned individuals need more.
- Skin Area: The more skin exposed, the more vitamin D produced. Exposing only the face and hands is generally insufficient. Aim to expose at least 40% of body surface area for meaningful production.
- Angle of the Sun: The UVB rays necessary for vitamin D synthesis are only available when the sun is at an angle greater than approximately 50 degrees above the horizon. A practical rule: if your shadow is shorter than your height, you are producing vitamin D.
- Season and Latitude: At latitudes above 37 degrees north, meaningful vitamin D production from sunlight is not possible from approximately November through February regardless of exposure time.
- Glass and Clothing: UVB rays do not penetrate glass or clothing. Sitting by a sunny window does not produce vitamin D.
- Avoid Burning: The goal is never to burn. Once a mild pinkness appears (indicating approximately half the minimal erythemal dose), cover up or apply sunscreen. Sunburn causes DNA damage and increases skin cancer risk without producing additional vitamin D.
Dietary Food Sources
While diet alone is rarely sufficient to maintain optimal vitamin D levels, certain foods contribute meaningfully to intake and should be included as part of a comprehensive strategy.
Best Animal-Based Sources
- Cod liver oil: 1 tablespoon provides approximately 1,360 IU (the single richest dietary source)
- Wild-caught salmon: 3.5 oz provides 600-1,000 IU (farmed salmon contains significantly less)
- Sardines: 3.5 oz provides approximately 270 IU
- Mackerel: 3.5 oz provides approximately 360 IU
- Herring: 3.5 oz provides approximately 215 IU
- Egg yolks: 1 large egg provides approximately 40 IU (pasture-raised eggs contain more)
- Beef liver: 3.5 oz provides approximately 50 IU
Plant-Based Sources
- UV-exposed mushrooms: Shiitake, maitake, and other mushrooms exposed to sunlight or UV light can provide significant amounts of vitamin D2 (up to 1,000 IU per serving for UV-treated mushrooms)
- Fortified plant milks: Typically provide 100-120 IU per cup (vitamin D2 or D3 depending on brand)
- Lichen-derived D3 supplements: While not a food, this is the best plant-based source of the preferred D3 form
It is important to emphasize that even with an excellent diet rich in these foods, most people will not achieve optimal 25(OH)D levels of 50-80 ng/mL without supplementation and/or regular sun exposure.
Toxicity Considerations
Vitamin D toxicity, while rare, is a legitimate concern that must be addressed to ensure safe supplementation practices.
When Does Toxicity Occur?
True vitamin D toxicity (hypervitaminosis D) typically does not occur until serum 25(OH)D levels exceed 150 ng/mL, and clinically significant toxicity is usually associated with levels above 200 ng/mL. This generally requires sustained daily intake of 40,000 IU or more for extended periods without monitoring. Toxicity from sunlight exposure is not possible because the body self-regulates cutaneous production.
Signs and Symptoms of Toxicity
- Hypercalcemia: Elevated blood calcium is the primary concern, manifesting as nausea, vomiting, poor appetite, constipation, and abdominal pain
- Polyuria and polydipsia: Excessive urination and thirst due to calcium-induced kidney effects
- Kidney damage: Calcium deposition in the kidneys (nephrocalcinosis) and kidney stones
- Soft tissue calcification: Calcium deposition in blood vessels and organs, particularly if vitamin K2 is not co-supplemented
- Confusion and disorientation: Neurological effects of severe hypercalcemia
Safety Considerations
- The Endocrine Society considers up to 10,000 IU daily to be the safe upper limit for adults, though routine doses in this range should be monitored with periodic blood testing
- Always co-supplement with vitamin K2 when using higher doses of vitamin D to prevent inappropriate calcium deposition
- Monitor serum calcium along with 25(OH)D when supplementing at higher doses
- Patients with granulomatous diseases (sarcoidosis, tuberculosis, certain lymphomas) are at higher risk for toxicity because their granulomas produce unregulated 1,25(OH)2D
- Regular testing every 3-6 months during high-dose supplementation is the best safeguard against toxicity
Related Laboratory Tests
To fully assess vitamin D status and its downstream effects, several complementary laboratory markers should be considered alongside the 25(OH)D test.
Serum Calcium (Total and Ionized)
Calcium levels help assess whether vitamin D is adequately performing its primary classical function of promoting calcium absorption. Low calcium with low vitamin D suggests deficiency-driven malabsorption. High calcium with high vitamin D may indicate toxicity or excessive supplementation. Ionized (free) calcium is the more physiologically relevant marker.
Parathyroid Hormone (PTH)
PTH and vitamin D exist in an inverse relationship. When vitamin D levels fall, PTH rises to compensate by pulling calcium from bones and increasing renal calcium retention. Elevated PTH in the presence of low vitamin D confirms secondary hyperparathyroidism due to vitamin D deficiency and signals active bone loss. A functional target for PTH is the lower half of the reference range.
Serum Magnesium (RBC Magnesium Preferred)
As discussed, magnesium is essential for vitamin D metabolism. Serum magnesium is commonly tested but is a poor marker, as only 1% of body magnesium resides in the blood. RBC magnesium is a far more accurate assessment of intracellular and total body magnesium status and should be ordered when possible.
Additional Complementary Tests
- Serum Phosphorus: Works in concert with calcium and vitamin D for bone mineralization
- Alkaline Phosphatase (ALP): Elevated ALP, particularly the bone-specific isoform, can indicate vitamin D deficiency-related bone turnover
- 1,25-Dihydroxyvitamin D: The active form, not routinely needed but useful in cases of granulomatous disease, kidney disease, or when 25(OH)D levels do not correlate with clinical presentation
- C-Reactive Protein (CRP) and ESR: Markers of systemic inflammation that often improve as vitamin D levels are optimized
- Complete Metabolic Panel: To assess kidney and liver function, both of which are critical for vitamin D metabolism
Summary and Clinical Considerations
The 25-hydroxyvitamin D test is one of the most valuable and actionable laboratory tests available in clinical practice. Vitamin D deficiency is a global epidemic with consequences that extend far beyond bone health, affecting immune function, cancer risk, cardiovascular health, mental health, and autoimmune disease susceptibility.
From a naturopathic and functional medicine perspective, the key clinical takeaways are:
- Test every patient at baseline and monitor regularly, with a target range of 50-80 ng/mL
- Prioritize sensible sun exposure as the primary source of vitamin D when feasible
- Supplement with vitamin D3 (not D2) in an oil-based form taken with a fat-containing meal
- Always co-supplement with vitamin K2 (MK-7), magnesium, and boron
- Individualize dosing based on current levels, body weight, absorption capacity, and clinical goals
- Monitor calcium and PTH alongside vitamin D to ensure safe and effective repletion
- Recognize that conventional "normal" ranges represent the minimum for disease prevention, not the optimum for health promotion
- Address underlying risk factors including indoor lifestyle, obesity, gut health, and medication effects
Optimizing vitamin D status is one of the most impactful, cost-effective, and evidence-based interventions available for improving patient outcomes across a wide spectrum of chronic and acute health conditions.
Research Papers and References
The following are curated PubMed literature searches covering the evidence base for 25-hydroxyvitamin D testing, interpretation, and clinical management. Each link opens a live, filtered PubMed query so the results stay current as new studies are indexed.
- 25-hydroxyvitamin D — PubMed literature search
- Vitamin D and bone health — PubMed literature search
- Vitamin D and immunity — PubMed literature search
- Vitamin D and cardiovascular disease — PubMed literature search
- Vitamin D and depression — PubMed literature search
- Vitamin D and cancer prevention — PubMed literature search
- Vitamin D supplementation meta-analysis — PubMed literature search
- Vitamin D and autoimmune disease — PubMed literature search
- Vitamin D toxicity — PubMed literature search
- Vitamin D and magnesium cofactor — PubMed literature search
- Vitamin K2 and vitamin D synergy — PubMed literature search
- Endocrine Society vitamin D guidelines — PubMed literature search
External Authoritative Resources
- MedlinePlus — Laboratory Tests Reference
- Lab Tests Online — Patient-Oriented Lab Test Reference (AACC)
- StatPearls / NCBI Bookshelf — Clinical Laboratory Reference
Connections
- How Your Skin Makes Vitamin D — interactive animation
- Bone Remodeling & Calcium Balance — interactive animation
- Vitamin D3
- Vitamin K
- Magnesium
- Calcium
- Boron
- Zinc
- Phosphorus
- Osteoporosis
- Hypertension
- Multiple Sclerosis
- Lupus
- Depression
- Hyperparathyroidism
- Cancer
- Immune Boosting
- Vitamin D3 and Immune System
- Vitamin D3 and Bone Health
- Vitamin D Controversy