IBS Medications Guide
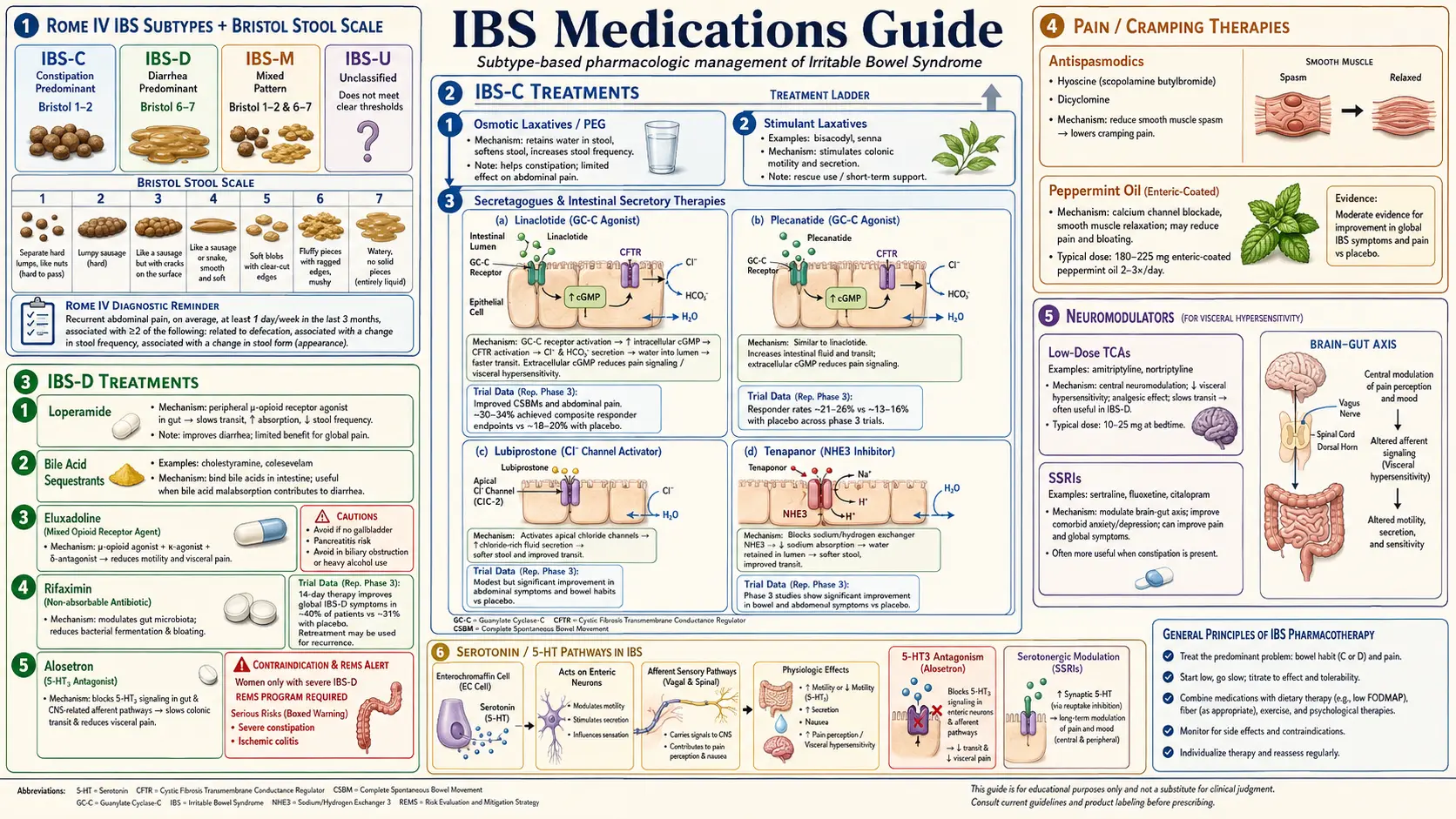
Table of Contents
- How to Use This Guide
- IBS-C Drugs — Constipation-Predominant
- IBS-D Drugs — Diarrhea-Predominant
- Antispasmodics — For Any Subtype
- Central Neuromodulators
- Experimental and Off-Label Options
- Practical Sequencing — How to Stack These Drugs
- De-Escalation — When to Pull Drugs Back
- Insurance Reality and Prior Authorizations
- Key Research Papers
- Connections
- Featured Videos
How to Use This Guide
Irritable bowel syndrome is not one disease — it is a symptom cluster with at least three clinically distinct flavors (IBS-C, IBS-D, IBS-M) and several important overlap syndromes (post-infectious IBS, SIBO, bile-acid malabsorption). The medication you need depends on which flavor you have, which mechanisms are driving your symptoms, and how much your insurance is willing to pay for.
This guide walks through the drugs in the order a sensible gastroenterologist would try them: cheapest and safest first, prescription-specific agents second, neuromodulators for pain or refractory cases, and experimental options last. Every drug is described with its real-world dose, typical U.S. cash and insurance cost, the side effects that actually make patients stop taking it, and the contraindications that matter. Nothing on this page replaces a conversation with your prescriber — but it should let you walk into that conversation knowing the landscape.
One ground rule: give every new drug a four-to-eight-week trial before declaring it a failure. IBS drugs rarely work on day one. They also rarely work on everyone. A 30–50% response rate is typical, which means several trial-and-error rounds are normal before you find a working combination.
IBS-C Drugs — Constipation-Predominant
IBS-C is defined by hard, infrequent, or straining-dependent stools plus abdominal pain. The medications below fall into three mechanistic buckets: secretagogues that pour fluid into the lumen, osmotic laxatives that hold water, and prokinetics that speed transit.
Linaclotide (Linzess) — 145 or 290 mcg daily
Linaclotide is a guanylate cyclase-C (GC-C) agonist. It binds receptors on the luminal surface of intestinal cells and triggers chloride and bicarbonate secretion, which draws water into the gut and accelerates transit. It also reduces visceral pain signaling, which is why many patients notice their cramping improves before their stools do.
Dose: 145 mcg once daily on an empty stomach, at least 30 minutes before the first meal of the day. The 290 mcg dose is approved for chronic idiopathic constipation but is sometimes used off-label for stubborn IBS-C. A 72 mcg dose exists for CIC only.
Cost: ~$550/month cash. Insurance usually covers it after failure of OTC laxatives, often with a copay of $25–$90. A manufacturer savings card can bring the copay to zero for commercially insured patients.
Side effects: Diarrhea is the dose-limiting issue — roughly 20% of patients get it, and 5% stop the drug for it. Taking it on an empty stomach is not optional; taken with food, you get unpredictable bursts of diarrhea an hour later.
Contraindications: Pediatric patients under age 2 (FDA black box for fatal dehydration in young children). Caution in known mechanical obstruction.
Plecanatide (Trulance) — 3 mg daily
Same mechanism as linaclotide (GC-C agonist), but engineered to be more pH-selective, which the manufacturer argues produces less diarrhea. In head-to-head comparison trials the difference is modest. Can be taken with or without food, which is a practical advantage for people who cannot reliably swallow a pill on an empty stomach.
Cost: ~$500/month cash, similar insurance pattern to linaclotide. If linaclotide causes too much diarrhea, this is the natural switch.
Lubiprostone (Amitiza) — 8 or 24 mcg twice daily with food
Lubiprostone activates chloride channel type 2 (ClC-2) on the luminal surface, also driving fluid into the gut. 8 mcg twice daily is the IBS-C dose (approved only in women); 24 mcg twice daily is the chronic constipation dose. Must be taken with food and water to blunt the main side effect, which is nausea.
Cost: ~$400/month cash. Older drug, more generic-friendly prior-authorization pathways.
Side effects: Nausea in roughly 30% of patients, which is why many people cannot tolerate it despite good efficacy. Headache and diarrhea are next.
Contraindications: Mechanical obstruction; pregnancy (category C, some teratogenic signal in animal studies).
Tenapanor (Ibsrela) — 50 mg twice daily
A newer, minimally absorbed NHE3 (sodium-hydrogen exchanger 3) inhibitor that blocks sodium absorption in the gut. Without sodium pulling water with it, fluid stays in the lumen and stool softens. Tenapanor is almost entirely gut-restricted, which gives it a clean systemic side-effect profile.
Dose: 50 mg twice daily, 5–10 minutes before breakfast and dinner. The timing matters.
Cost: ~$1,100/month cash — the most expensive IBS-C option. Insurance coverage has improved since launch but still requires a prior authorization documenting failure of linaclotide or plecanatide.
Side effects: Diarrhea (up to 16%), abdominal distension, flatulence. No meaningful systemic absorption, so drug interactions are minimal.
PEG 3350 (Miralax) — OTC, 17 g in 8 oz liquid once daily
The workhorse. Polyethylene glycol 3350 is an inert, non-absorbed polymer that holds water in the stool. It is cheap (~$15 for a month's supply), non-cramping, and safe enough to use daily for years. Most gastroenterologists try it before any prescription IBS-C drug.
Dose: One 17 g capful dissolved in 8 oz of liquid, once daily. Titrate up to twice daily or down to every other day based on response.
Side effects: Bloating, especially in the first week. Rarely electrolyte shifts at very high doses.
Magnesium Oxide or Citrate — 400–1,200 mg at bedtime
Magnesium draws water into the gut by osmosis. Cheap, widely available, and often used in patients who also have migraines or leg cramps (where magnesium has independent benefit). Citrate is better absorbed and easier on the stomach; oxide is cheaper and more laxative per milligram.
Cautions: Avoid in chronic kidney disease (risk of magnesium accumulation and cardiac toxicity). Can cause loose stools or diarrhea at higher doses — use that as the titration signal.
Prucalopride (Motegrity) — 2 mg once daily
A highly selective 5-HT4 receptor agonist that stimulates colonic motility. FDA-approved for chronic idiopathic constipation, used off-label for IBS-C, particularly when secretagogues have failed or when slow colonic transit is documented. Earlier 5-HT4 drugs (cisapride, tegaserod) were pulled for cardiac issues; prucalopride's receptor selectivity eliminates most of that risk.
Cost: ~$500/month cash. Prior authorization often rejects IBS-C indication; appeal with documentation of failed secretagogues.
Side effects: Headache (common, usually first week only), nausea, transient diarrhea.
IBS-D Drugs — Diarrhea-Predominant
IBS-D usually responds to one of three strategies: resetting the small-bowel microbiome (rifaximin), slowing motility (eluxadoline, alosetron), or blocking serotonin signals that trigger gut urgency (ondansetron, alosetron). Bile-acid binders are a fourth bucket for the subset with bile-acid malabsorption.
Rifaximin (Xifaxan) — 550 mg three times daily for 14 days
The most studied IBS-D drug in the last fifteen years. Rifaximin is a minimally absorbed (<0.4%) oral antibiotic that acts locally on gut bacteria. The pivotal TARGET 1 and 2 trials (Pimentel 2011) showed roughly a 10-percentage-point absolute response advantage over placebo — modest but real, especially for the SIBO-overlap subset. If symptoms return, the drug can be repeated up to two additional times (TARGET 3).
Dose: 550 mg three times daily for 14 days. Total course: 42 tablets.
Cost: ~$2,200 per 14-day course cash. Insurance coverage for IBS-D is now routine since the 2015 FDA approval, though prior authorizations are the rule and documentation of IBS-D (not just “diarrhea”) is mandatory. See Rifaximin Protocols for dosing variations, retreatment criteria, and combined regimens for methane-predominant cases.
Side effects: Remarkably clean — the minimal systemic absorption means headache and nausea are the most common complaints, and C. difficile risk is lower than with systemic antibiotics.
Eluxadoline (Viberzi) — 75 or 100 mg twice daily with food
A mixed mu-opioid agonist/delta-opioid antagonist that slows gut motility without the central effects of traditional opioids. Trials (Lembo 2016) showed real benefit for IBS-D with pain. The catch: a significant minority of patients developed pancreatitis or sphincter-of-Oddi spasm, and the FDA issued a contraindication.
Do not use if: You have no gallbladder (post-cholecystectomy), known biliary disease, alcohol use exceeding 3 drinks/day, history of pancreatitis, or severe hepatic impairment. The no-gallbladder contraindication catches many patients off-guard — confirm this before the first dose.
Cost: ~$1,400/month cash.
Side effects beyond the contraindications: Constipation (expected, often signals dose is too high), nausea, abdominal pain.
Alosetron (Lotronex) — 0.5–1 mg twice daily
A 5-HT3 receptor antagonist that reduces visceral hypersensitivity and slows colonic transit. Highly effective for a narrow subset: women with severe, chronic IBS-D who have failed other therapies. The drug was briefly withdrawn in 2000 after reports of ischemic colitis and severe constipation; it was reintroduced under a restricted REMS (Risk Evaluation and Mitigation Strategy) program that requires prescriber enrollment and patient counseling.
Dose: Start at 0.5 mg twice daily for four weeks; titrate to 1 mg twice daily only if needed and tolerated.
Cost: ~$900/month cash. Insurance coverage exists but requires REMS documentation.
Warnings: Ischemic colitis risk is roughly 1 in 1,000 patient-years — uncommon but potentially serious. Stop immediately for any new rectal bleeding or severe constipation.
Ondansetron — 4–8 mg up to three times daily (off-label)
A generic 5-HT3 antagonist originally developed for chemotherapy nausea. Small randomized trials show it meaningfully reduces stool frequency and urgency in IBS-D at a fraction of alosetron's cost. Cheap, widely available, and does not require a REMS program — which is why many gastroenterologists reach for it first.
Dose: 4 mg once daily as a starting point, titrate up to 8 mg three times daily if needed. Oral dissolving tablets are convenient but expensive; standard tablets are <$20/month generic.
Side effects: Constipation (titrate down if severe), headache, QT prolongation at high doses — get a baseline ECG if you have known cardiac issues or are on other QT-prolonging medications.
Cholestyramine or Colesevelam — For Bile-Acid Malabsorption
Roughly one-quarter to one-third of “IBS-D” patients actually have bile-acid malabsorption — excess bile acids reaching the colon and triggering secretory diarrhea. A bile-acid sequestrant (cholestyramine 4 g 1–4 times daily, or colesevelam 625 mg 3–6 tablets daily) binds the excess bile acids and resolves the diarrhea within days in responders. Colesevelam is better tolerated (tablet vs. gritty powder) but more expensive.
For diagnosis and workup, see the bile-acid malabsorption article. A short empiric trial is reasonable even without formal testing — response within 5–7 days is both diagnostic and therapeutic.
Antispasmodics — For Any Subtype
Antispasmodics are symptomatic tools for cramping and postprandial urgency. They do not change the underlying disease, but they reliably take the edge off an acute flare and can be taken as needed (20–30 minutes before a meal that usually causes trouble) or on a standing schedule.
Hyoscyamine (Levsin) — 0.125–0.25 mg up to four times daily
A sublingual or oral anticholinergic that blocks muscarinic receptors in gut smooth muscle. Fast onset (10–20 minutes sublingual). Useful for as-needed symptom control before meals.
Dicyclomine (Bentyl) — 10–20 mg four times daily
Similar mechanism, longer-acting, available as a generic tablet. Classic anticholinergic side-effect profile: dry mouth, blurred vision, urinary hesitancy, sedation, constipation. Avoid in glaucoma, benign prostatic hyperplasia, or frail elderly patients where falls are a concern.
Peppermint Oil, Enteric-Coated (IBgard) — 1–2 capsules three times daily
L-menthol is a natural calcium-channel blocker in gut smooth muscle. Enteric coating is essential — uncoated peppermint releases in the stomach, causing heartburn without reaching the colon. IBgard uses microspheres designed to release in the small bowel. Trial data show modest but consistent benefit; it is safe, cheap, and a reasonable early trial before prescription drugs. See the peppermint and probiotics article for dosing details and brand comparisons.
Cautions on anticholinergics: Dry mouth is nearly universal. Constipation can be a feature (helpful in IBS-D) or a bug (problematic in IBS-M). Avoid stacking multiple anticholinergics (e.g., hyoscyamine plus a tricyclic plus an antihistamine) — cumulative anticholinergic burden causes cognitive impairment, especially in older patients.
Central Neuromodulators
IBS is fundamentally a disorder of gut-brain signaling. Low-dose antidepressants, used at doses well below those required for depression, modulate visceral pain perception and gut motility through descending serotonin and norepinephrine pathways. Calling them “gut-brain neuromodulators” rather than “antidepressants” is accurate and usually reduces patient resistance.
Tricyclic Antidepressants (TCAs) — IBS-D and Pain-Dominant
Low-dose TCAs are one of the most reliably effective IBS drug classes, especially for patients whose pain is the worst symptom. The anticholinergic side profile also slows transit, which helps IBS-D and hurts IBS-C.
- Amitriptyline — 10 mg at bedtime to start, titrate to 25–50 mg. Most sedating and most anticholinergic; best if insomnia coexists.
- Nortriptyline — 10–25 mg at bedtime, titrate to 50 mg. Metabolite of amitriptyline, somewhat less sedating and less anticholinergic.
- Desipramine — 25–50 mg, titrate to 100 mg. Least sedating, least anticholinergic — best choice in daytime-dosed patients or when morning grogginess is unacceptable.
Cost: All are generic; $4–$15/month. Get a baseline ECG in patients over 50 or with known cardiac disease (QT prolongation). Avoid in IBS-C (they worsen constipation).
SSRIs — IBS-C
Selective serotonin reuptake inhibitors tend to increase gut transit, making them the neuromodulator of choice in IBS-C with comorbid anxiety or depression. Paroxetine (10–40 mg) and citalopram (10–40 mg) have the most IBS data. Fluoxetine works too but is the most activating. Start low, titrate slowly, expect 4–8 weeks to gauge response.
Cost: Generic, $4–$15/month.
SNRIs — Overlap With Fibromyalgia
Duloxetine (30–60 mg daily) is particularly useful when IBS overlaps with fibromyalgia, chronic pelvic pain, or widespread musculoskeletal pain. It treats both conditions with a single drug. Nausea on initiation is common but usually resolves within two weeks.
Mirtazapine — Nausea, Insomnia, Weight Loss
A tetracyclic with strong anti-nausea and sleep-promoting properties. Useful in the subset of IBS patients who have early satiety, unintentional weight loss, or insomnia. Doses of 7.5–15 mg at bedtime are usually sufficient for gut symptoms. Weight gain is the main downside — an asset in an underweight patient, a liability in others.
Experimental and Off-Label Options
Low-Dose Naltrexone (LDN) — 1.5–4.5 mg at bedtime
At ultra-low doses, naltrexone briefly blocks opioid receptors and upregulates endogenous endorphin production. The result is modulation of immune and pain signaling that appears particularly useful in pain-dominant IBS and in IBS overlapping with fibromyalgia or chronic fatigue. Evidence is still mostly observational and small-trial, but the safety profile is excellent and the cost (through compounding pharmacies) is modest (~$30–$60/month). See the LDN article for full dosing and titration schedules.
Cannabidiol (CBD)
Evidence is genuinely limited. A few small trials suggest CBD may reduce visceral pain, but dosing, purity, and product variability make generalization impossible. If you try it, use a COA-verified (certificate-of-analysis) isolate from a reputable vendor, start with 10–25 mg at bedtime, and be honest with yourself about whether it is helping after six weeks. Check drug interactions — CBD inhibits CYP2C19 and CYP3A4.
Gabapentin and Pregabalin
Gabapentinoids reduce visceral hypersensitivity in small IBS trials, but the side-effect burden (sedation, dizziness, weight gain, dependence potential) limits their usefulness. Consider in patients whose pain is the dominant problem and who have failed TCAs and SNRIs, or who have coexisting neuropathic pain. Doses: gabapentin 300 mg at bedtime titrated to 300–900 mg three times daily; pregabalin 25–75 mg twice daily titrated to 150 mg twice daily.
Practical Sequencing — How to Stack These Drugs
A sensible stepwise approach for each subtype, assuming no red-flag symptoms and a confirmed IBS diagnosis:
IBS-C sequence:
- Fiber optimization (soluble: psyllium 5–10 g/day) + PEG 3350 + magnesium oxide/citrate. Four-week trial.
- Add enteric-coated peppermint oil if cramping persists.
- If inadequate, start linaclotide 145 mcg or plecanatide 3 mg. Eight-week trial.
- If inadequate or not tolerated, switch to tenapanor 50 mg BID or trial lubiprostone 8 mcg BID.
- Add an SSRI (paroxetine or citalopram) if anxiety or mood is a parallel driver, or if visceral pain persists.
- Add prucalopride 2 mg daily for refractory slow-transit cases.
IBS-D sequence:
- Dietary trial (low-FODMAP) + loperamide 2–4 mg as needed (cap at 16 mg/day).
- Empiric trial of cholestyramine 4 g daily for 1–2 weeks. Rapid response confirms bile-acid malabsorption.
- Add peppermint oil and/or ondansetron 4 mg up to three times daily for urgency.
- If postinfectious pattern or SIBO overlap suspected, rifaximin 550 mg TID x 14 days.
- If inadequate, low-dose TCA (nortriptyline 10–25 mg at bedtime) titrated over 4–6 weeks.
- If still inadequate and pain-dominant, eluxadoline 75–100 mg BID (confirm gallbladder present). Or alosetron in severe, refractory women under REMS.
- Consider LDN trial for pain-dominant refractory cases, especially with fibromyalgia overlap.
IBS-M (mixed) is the hardest subtype to medicate because the same drug can flip stools in the wrong direction. The safest anchors are antispasmodics and low-dose TCAs (for pain), with on-demand loperamide for diarrhea episodes and on-demand PEG 3350 for constipation episodes. Avoid stacking strong motility-slowing and motility-speeding agents simultaneously — the result is unpredictable.
Rule: stack one drug at a time. If you start two new drugs in the same week and something changes, you cannot tell which drug caused it. Add one, wait at least four weeks, then add the next.
De-Escalation — When to Pull Drugs Back
IBS is a chronic but fluctuating condition. Symptoms often improve with lifestyle changes, aging, or reduced stress, and patients can end up on a polypharmacy regimen they no longer need. A deliberate de-escalation trial every 6–12 months is reasonable.
- Peel drugs back one at a time, in reverse order of the order they were added.
- Taper slowly — over 2–4 weeks for neuromodulators, faster for PRN drugs.
- If symptoms return within a month, restart the last dropped drug. If they do not, keep tapering.
- Rifaximin is a special case — it is a pulse-dosed drug, not a daily one. If you respond to a course, you do not stay on it. You repeat only if symptoms recur.
Insurance Reality and Prior Authorizations
The branded IBS drugs (linaclotide, plecanatide, tenapanor, eluxadoline, rifaximin) almost always require prior authorization. The appeal process is usually winnable but requires documentation of:
- An ICD-10 code for the correct IBS subtype (not just K58.9 “IBS unspecified” — use K58.1 IBS-D or K58.2 IBS-C).
- Failure of at least one and often two less-expensive alternatives, with duration and reason for failure documented in the chart.
- For alosetron, enrollment of both prescriber and patient in the REMS program.
- For rifaximin, documentation that the patient has IBS-D, not chronic diarrhea of another cause.
Manufacturer savings cards (for commercially insured patients, not Medicare/Medicaid) can reduce copays to $0–$25 on most branded agents. Patient assistance programs cover uninsured patients who meet income thresholds. Ask your gastroenterologist's office whether they have a dedicated prior-authorization specialist — the larger practices do, and it dramatically improves approval rates.
Key Research Papers
- Chey WD, et al. Linaclotide for irritable bowel syndrome with constipation: a 26-week, randomized, double-blind, placebo-controlled trial. Am J Gastroenterol. 2015.
- Pimentel M, et al. Rifaximin therapy for patients with irritable bowel syndrome without constipation (TARGET 1 and 2). N Engl J Med. 2011.
- Lembo AJ, et al. Eluxadoline for irritable bowel syndrome with diarrhea. N Engl J Med. 2016.
- Lacy BE, et al. ACG clinical guideline: management of irritable bowel syndrome. Am J Gastroenterol. 2020.
Live PubMed Searches
For further reading, the following PubMed topic searches return current peer-reviewed work on each drug class discussed above:
- Linaclotide and IBS-C randomized trials
- Plecanatide for IBS-C
- Tenapanor and NHE3 inhibition in IBS-C
- Rifaximin and IBS-D TARGET trials
- Eluxadoline safety and pancreatitis risk
- Alosetron REMS and severe IBS-D
- Ondansetron off-label use in IBS-D
- Tricyclic antidepressants and visceral pain in IBS
- Duloxetine in IBS and fibromyalgia overlap
- Low-dose naltrexone and visceral pain
- Bile-acid malabsorption, cholestyramine, and IBS-D
- Enteric-coated peppermint oil in IBS meta-analyses
Connections
- The Gut Barrier & Your Microbiome — interactive animation
- Irritable Bowel Syndrome
- SIBO
- Rifaximin Protocols
- Fibromyalgia
- Low-Dose Naltrexone
- Peppermint, Probiotics, and Herbals
- Low-FODMAP Diet for IBS
- Gut-Directed Hypnotherapy and CBT
- Post-Infectious IBS
- Rome IV Subtypes
- IBS and SIBO Overlap
- Chronic Pain
- Constipation
- Bloating
- Magnesium
- Depression
- Anxiety
- Peppermint