Visceral Hypersensitivity and the Brain-Gut Axis in IBS
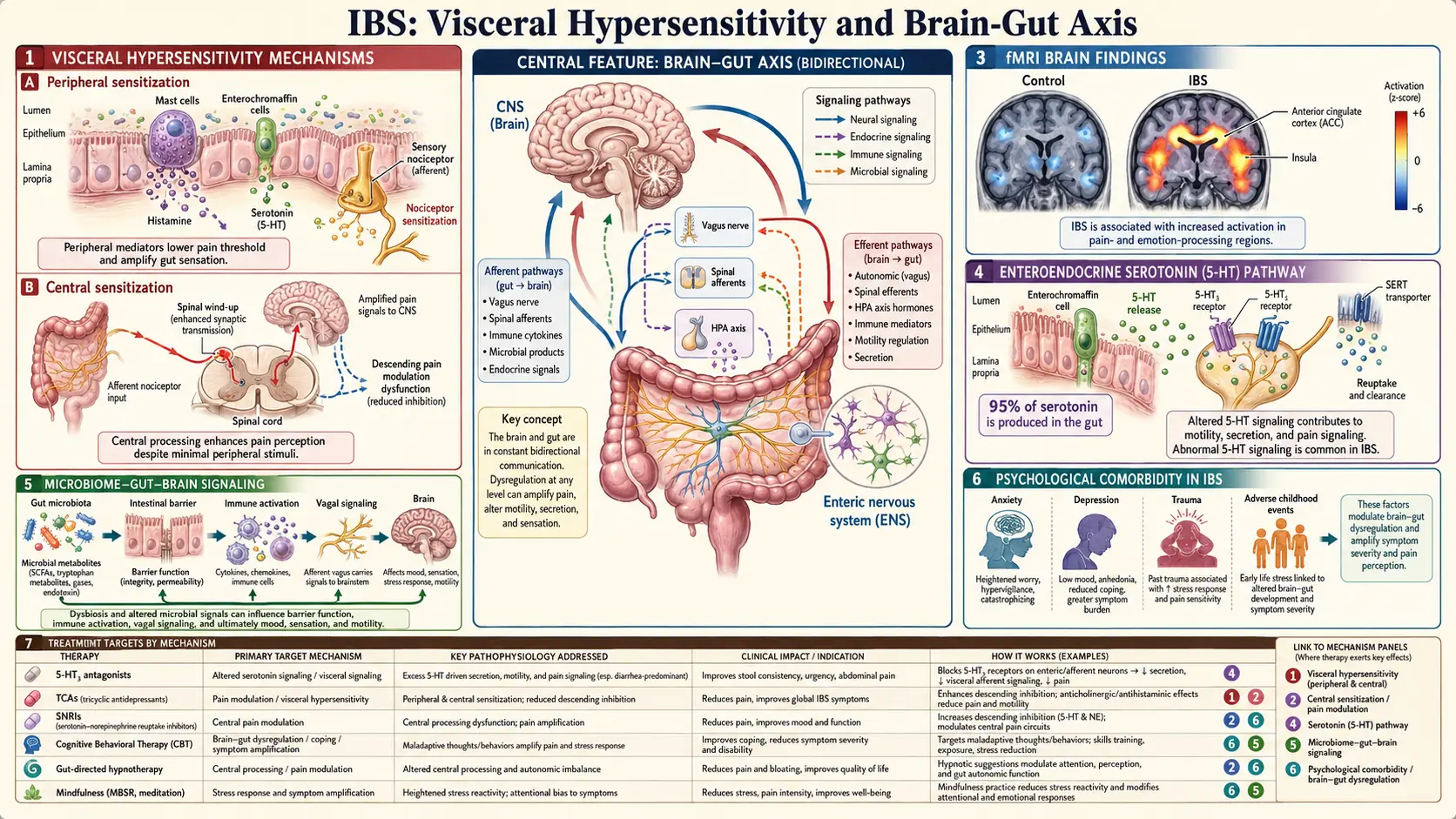
Table of Contents
- What Visceral Hypersensitivity Actually Is
- The Barostat Studies — Measuring a "Real" Pain Threshold
- The Biology: TRPV1, Mast Cells, and 5-HT3
- The Brain-Gut-Microbiome Axis
- The Enteric Nervous System — Your "Second Brain"
- How Stress Actually Triggers an IBS Flare
- Central Sensitization and the Overlap Conditions
- Why Low-Dose SSRIs and TCAs Help
- Gut-Directed Hypnotherapy — Why It Works
- Vagal Tone, HRV, and Polyvagal Theory
- Diet, Microbiome, and Upstream Signaling
- Early-Life Adversity and the ACE Connection
- The Post-Infectious Shift to Hyperalgesia
- Practical Interventions You Can Start This Week
- Both Things Are True
- Key Research Papers
- Connections
- Featured Videos
What Visceral Hypersensitivity Actually Is
Your gut is constantly doing things. Food moves through it. Gas bubbles form and migrate. The muscular wall contracts and relaxes. The colon stretches when stool arrives. In healthy digestion, almost none of this reaches conscious awareness — the nervous system filters out the noise and only speaks up when something genuinely needs your attention.
In IBS, that filter is broken. The same volume of gas, the same stretch of the bowel wall, the same normal peristaltic contraction registers as pain, urgency, bloating, or cramping. Your gut is not doing anything abnormal. Your nervous system is reporting normal events as alarming ones. This is visceral hypersensitivity, and it is the single best-validated biological finding in IBS.
It matters because it reframes the entire illness. IBS is not "nothing wrong." It is not anxiety wearing digestive clothes. It is a real, measurable change in how the nerves of the gut and the pain-processing regions of the brain calibrate signals. The pain is real. The mechanism is real. And because the mechanism is neurological rather than structural, treatments aimed at the nervous system work — often better than anything aimed at the gut itself.
The Barostat Studies — Measuring a "Real" Pain Threshold
How do researchers prove that gut nerves are over-reactive rather than that patients are simply "complaining more"? The gold-standard tool is the rectal barostat. A small balloon is placed in the rectum and inflated in carefully controlled steps while the subject reports the volume at which they first feel the balloon, then discomfort, then pain.
The findings have been replicated across dozens of labs since the 1970s:
- IBS patients first perceive balloon distension at significantly lower volumes than healthy controls.
- The volume required to produce discomfort and pain is typically 30–60% lower in IBS than in matched controls.
- The effect is reproducible even when subjects are blinded to the inflation steps — ruling out simple suggestibility.
- Functional MRI during distension shows IBS brains activate pain-processing regions (anterior cingulate cortex, insula, thalamus) at distension levels that barely register in controls.
This is the key sentence to hold onto: your pain threshold for gut distension is lower, and it is measurable on a machine. No one with normal rectal pain thresholds gets a barostat study and is told they have IBS. The nervous-system change is not a metaphor.
The Biology: TRPV1, Mast Cells, and 5-HT3
Under the microscope, several mechanisms combine to lower the threshold.
TRPV1 channels are the same heat-and-capsaicin receptors that make chili peppers feel hot. They sit on sensory nerve endings in the gut wall. In IBS, TRPV1 expression is increased, and the channels open in response to milder stimuli. Biopsy studies of IBS colons consistently show elevated TRPV1-positive nerve fibers in the mucosa.
Mast cells are immune cells that live right next to visceral nerves. When they degranulate, they release histamine, tryptase, and prostaglandins directly onto nearby nerve endings, sensitizing them. IBS patients have more mast cells in the colonic mucosa, and the mast cells cluster closer to nerves than in healthy controls. This is part of why some IBS overlaps clinically with mast cell activation syndrome (MCAS).
Serotonin (5-HT) is the molecule most people associate with mood — but roughly 90% of the body's serotonin is made in the gut, not the brain. Enterochromaffin cells in the intestinal lining release serotonin in response to food and stretch, and this serotonin drives motility, secretion, and sensation through the 5-HT3 receptor on sensory nerves. IBS-D patients tend to have elevated postprandial serotonin; IBS-C patients may have reduced signaling. This is why a 5-HT3 antagonist (alosetron) reduces diarrhea and pain, and a 5-HT4 agonist (prucalopride, tegaserod) helps constipation. See the IBS medications guide.
The Brain-Gut-Microbiome Axis
Modern IBS research talks less about "the brain" and "the gut" as separate organs and more about a continuous brain-gut-microbiome axis — a bidirectional communication network with at least four lanes of traffic:
- The vagus nerve. The tenth cranial nerve wanders from the brainstem down through the neck, chest, and abdomen, reaching the colon. Roughly 80% of vagal fibers carry signals upward from gut to brain; only 20% carry instructions downward. Your gut talks to your brain far more than your brain talks to your gut.
- The enteric nervous system (ENS). A mesh of 200–600 million neurons embedded in the gut wall that can coordinate digestion without any brain input at all (see the next section).
- The HPA axis. The hypothalamic-pituitary-adrenal stress system releases cortisol, which modulates gut permeability, motility, and immune activity.
- Microbial metabolites. Gut bacteria ferment dietary fiber into short-chain fatty acids (SCFAs) — butyrate, propionate, acetate — that feed colon cells, reduce inflammation, and cross into circulation where they influence brain function. Microbes also produce neurotransmitters directly, including GABA, dopamine, and serotonin precursors.
The practical point for an IBS patient: a flare is not a one-direction event. Stress alters microbiome composition within hours. An altered microbiome changes what metabolites reach the brain. Those metabolites change mood and pain perception. Mood and pain perception change eating, sleeping, and vagal tone. And around it goes.
The Enteric Nervous System — Your "Second Brain"
The enteric nervous system contains more neurons than the entire spinal cord. It uses every major neurotransmitter the brain uses — serotonin, dopamine, acetylcholine, GABA, nitric oxide. It coordinates peristalsis, secretion, blood flow, and immune signaling locally. If the vagus nerve is severed, the gut continues to digest food on its own. This is why it earned the nickname the "second brain" (popularized by Michael Gershon's book of the same name).
In IBS, the ENS is hypersensitive and can become dysregulated in its own right. Inflammation from an infection or immune trigger can remodel enteric neurons, lowering their firing thresholds for years. This "peripheral sensitization" layer exists alongside the central (brain) sensitization, and together they sustain symptoms long after any original trigger is gone.
How Stress Actually Triggers an IBS Flare
"Stress makes it worse" is the most eye-rolling advice an IBS patient hears, because it usually comes with the implication that the problem is your failure to relax. The mechanism is not psychological. It is a chain of measurable physiological events:
- Stress activates the HPA axis. The hypothalamus releases CRH (corticotropin-releasing hormone), which triggers the adrenal glands to pump out cortisol and the locus coeruleus to release norepinephrine.
- Cortisol increases intestinal permeability. Tight junctions between gut epithelial cells loosen. Larger molecules slip through the barrier that should have stayed in the lumen.
- Those molecules activate mucosal mast cells. The mast cells degranulate, dumping histamine and tryptase onto nearby nerve endings.
- Sensitized nerves fire more. Normal gas and peristalsis now register as cramping and urgency.
- The brain hears the noise and amplifies it. Anxiety about the flare feeds back into step 1.
Stress is not "all in your head" because the cascade includes your adrenal glands, your gut lining, and your immune cells. But stress starts in the brain, which is why brain-directed treatments legitimately interrupt it.
Central Sensitization and the Overlap Conditions
The same pain-amplifying mechanism that affects the gut in IBS also affects the muscles in fibromyalgia, the pelvic floor in endometriosis, the bladder wall in interstitial cystitis, and the trigeminal nerve in chronic migraine. Rheumatologists and pain specialists call this pattern central sensitization — the central nervous system has turned up the gain on pain signals coming from many body regions at once.
This is why the same person so often has several of these diagnoses:
- IBS + fibromyalgia is one of the most-studied comorbidities in medicine (overlap roughly 30–70% depending on the cohort).
- Endometriosis and IBS coexist in a high fraction of pelvic-pain patients; the chronic pelvic pain may outlast adequate endometriosis surgery because pelvic nerves are centrally sensitized (see pelvic floor therapy and central sensitization).
- Chronic migraine, TMJ pain, and IBS cluster in the same patients.
- Autonomic overlap syndromes like POTS and ME/CFS share gut symptoms and sensitivity phenotypes.
For a detailed explanation of the underlying mechanism, see the fibromyalgia deep dive on central sensitization. Understanding this connection is useful because a treatment that calms central sensitization for one condition (low-dose TCAs, for example, or graded aerobic exercise) will often help the others, too.
Why Low-Dose SSRIs and TCAs Help
When a gastroenterologist suggests a low-dose tricyclic antidepressant (TCA) like amitriptyline 10–25 mg at bedtime, or a selective serotonin reuptake inhibitor (SSRI) like sertraline, the most common patient reaction is frustration: "So you think this is depression?"
No — the mechanism is different. These drugs are prescribed for IBS at doses too low to reliably treat depression (a TCA antidepressant dose is typically 75–150 mg). At low doses they work as central pain modulators: they raise descending inhibitory signals from the brainstem to the spinal cord, essentially turning down the volume knob on visceral pain inputs. TCAs also have direct anticholinergic effects that slow gut transit, helpful in IBS-D.
The American College of Gastroenterology gives a strong recommendation for TCAs in IBS, with an effect size comparable to or larger than many gut-directed drugs. SSRIs help a subset — particularly those with prominent constipation and anxiety — and SNRIs (duloxetine) are useful when fibromyalgia or chronic pain coexists. The medications guide covers dosing, side effects, and how to choose among them.
Gut-Directed Hypnotherapy — Why It Works
Gut-directed hypnotherapy is not stage hypnosis, and it is not a placebo handwave. It is a structured protocol (typically 7–12 sessions following the Manchester or North Carolina scripts) that uses guided imagery and suggestion to change how the brain processes visceral signals. Brain imaging studies show measurable changes in anterior cingulate cortex and insula activation after a completed course — the same regions that light up abnormally during barostat distension.
Response rates in randomized trials run around 50–75%, with benefits that persist for years after treatment ends. For severe, refractory IBS it is one of the most effective interventions ever studied, comparable to the best drug therapies and with no side effects. The sibling article on gut-directed hypnotherapy and CBT covers protocols, app options (Nerva, Mahana IBS), and how to find a qualified practitioner.
Vagal Tone, HRV, and Polyvagal Theory
Heart rate naturally speeds up slightly on each inhale and slows on each exhale. The size of that beat-to-beat variation is called heart rate variability (HRV), and it is the best non-invasive proxy for vagal tone — the moment-to-moment strength of your parasympathetic nervous system.
IBS patients, on average, have lower HRV than controls. Low HRV correlates with worse symptom severity, more post-meal pain, and more anxiety. This is not definitive proof of causation, but it dovetails with everything else: if your parasympathetic tone is low, your gut's natural "rest and digest" brake is weak, and your sympathetic stress response dominates.
The good news is that HRV is trainable. Slow breathing at roughly five to six breaths per minute (inhale for five to six seconds, exhale for five to six seconds) maximally increases vagal output and raises HRV over weeks of practice. Consumer biofeedback tools — Elite HRV, HeartMath Inner Balance, Oura, Apple Watch HRV — let you measure progress.
Polyvagal theory, proposed by Stephen Porges, is the most popular framing of vagal tone in the patient community: the idea that the vagus has two branches (a primitive "freeze" branch and a newer "social engagement" branch) and that trauma shifts you into the freeze state. It is a compelling and often helpful way to think about the body, but be aware that polyvagal theory's specific anatomical claims are contested in peer-reviewed neuroanatomy. The clinical practices that come out of it — slow breathing, humming, cold exposure to the face, safe social connection — are well supported even though the theoretical scaffolding is debated. Use the practices; hold the theory loosely.
Diet, Microbiome, and Upstream Signaling
Changing what you eat changes which microbes flourish. Which microbes flourish changes which metabolites reach your bloodstream and brain. Diet is therefore not just "fuel" — it is an upstream lever on the entire brain-gut axis.
- Low-FODMAP, done properly as a 2–6 week elimination followed by structured reintroduction, reduces fermentation, gas, and distension — lowering the mechanical signal that sensitized nerves amplify. See the low-FODMAP guide.
- Fiber matters for SCFA production. Butyrate from microbial fermentation of soluble fiber nourishes colonocytes and has direct anti-inflammatory effects. Chronically low-fiber diets starve the microbes that keep the gut lining healthy.
- Specific probiotics have been studied in IBS (Bifidobacterium infantis 35624, for example) with modest benefit. This is not a universal prescription — see the peppermint and herbals page.
Diet is a partial, upstream lever. It does not replace nervous-system treatment, but it reduces the load on an already overreactive system.
Early-Life Adversity and the ACE Connection
Adverse Childhood Experiences (ACEs) — abuse, neglect, household dysfunction before age 18 — correlate with adult IBS at roughly 2–4 times the rate of controls in multiple large cohort studies. The mechanism plausibly involves long-term calibration of the HPA stress axis during development: a child in a chronically unsafe environment grows up with a stress response set to higher baseline activity and a gut that has matured in that hormonal bath.
This is not a claim that every IBS patient has trauma, and it is not a claim that if you had a happy childhood your IBS is not "real." It is simply that ACEs are one identifiable risk factor among many, and for patients whose IBS began in childhood or alongside chronic anxiety, trauma-informed therapy (not just symptom-focused CBT) can be a legitimate piece of treatment.
The Post-Infectious Shift to Hyperalgesia
Roughly 10% of people who get a significant bout of food poisoning or gastroenteritis develop post-infectious IBS. The infection is long gone, but the gut nerves never re-calibrate. Mast cell density stays elevated for months to years. Sensory nerve fibers that sprouted during the inflammation remain. Anti-vinculin antibodies (produced in response to bacterial cytolethal distending toxin) cross-react with gut nerves and impair motility.
This is visceral hypersensitivity in its clearest causal form: a defined trigger, a measurable immunological fingerprint, and a persistent change in gut-nerve behavior. It is worth knowing about because the treatment priorities shift — mast-cell stabilizers, prokinetics, and sometimes rifaximin if SIBO has emerged — and the prognosis is better than people fear. See the post-infectious IBS article for the full workup.
Practical Interventions You Can Start This Week
Do not wait for a specialist to start working on the nervous-system side of IBS. These are cheap, low-risk, and backed by real evidence:
- Diaphragmatic breathing, twice daily. Five minutes morning and evening. One hand on chest, one on belly; only the belly hand moves. Inhale for a count of five, exhale for six. This alone meaningfully raises vagal tone in weeks.
- HRV biofeedback. Free apps (Elite HRV, Welltory) pair with a chest strap or a phone camera. HeartMath Inner Balance is the most polished paid option. Aim for 10–20 minutes a day of paced breathing with live feedback.
- Yoga, tai chi, or qigong. Slow movement, extended exhales, and parasympathetic activation. IBS-specific yoga trials show symptom improvement comparable to low-FODMAP.
- Walking after meals. Ten to twenty minutes. Improves gastric emptying, reduces postprandial bloat, and modestly raises HRV.
- Sleep. Sleep deprivation lowers pain thresholds across every chronic-pain condition ever studied. Protect seven to eight hours as ruthlessly as you protect your diet.
- Cold water on the face. Splashing cold water on the forehead and cheeks triggers the mammalian dive reflex and a sharp vagal pulse. Useful for interrupting an acute anxiety-flare cascade.
- Dedicated gut-directed apps or therapy. See the hypnotherapy and CBT page for Nerva, Mahana IBS, and how to find a GI-psychology clinician.
Both Things Are True
If you take nothing else from this page, take this:
It is not in your head — meaning your pain is real, your gut nerves are measurably hyperreactive, your mast cells are measurably more abundant, and your pain thresholds are measurably lower on a machine that does not care whether you believe in them.
And your brain is part of the treatment — meaning the nervous-system side of this illness is a legitimate target. Hypnotherapy, CBT, low-dose neuromodulators, HRV training, breathing practice, and sleep are not consolation prizes for people whose "real" treatment failed. They are mechanistically appropriate first-line interventions for a mechanistically neurological condition.
Patients who grasp both halves of that sentence at the same time tend to do best. The ones who fight off any suggestion of a brain component spend years chasing structural explanations that are not there. The ones who accept "it's all anxiety" stop pursuing legitimate pharmacologic and dietary help. The truth is both, at once, without apology.
Key Research Papers
- Mayer EA. Gut feelings: the emerging biology of gut-brain communication. Nat Rev Neurosci. 2011;12(8):453–466.
- Drossman DA. Functional gastrointestinal disorders: history, pathophysiology, clinical features, and Rome IV. Gastroenterology. 2016;150(6):1262–1279.
- Enck P, Aziz Q, Barbara G, et al. Irritable bowel syndrome. Nat Rev Dis Primers. 2016;2:16014.
- Farmer AD, Aziz Q. Visceral pain hypersensitivity in functional gastrointestinal disorders. Br Med Bull. 2009;91:123–136. (Review on central mechanisms of visceral pain.)
- Ritchie J. Pain from distension of the pelvic colon by inflating a balloon in the irritable colon syndrome. Gut. 1973;14(2):125–132. (Foundational barostat study demonstrating lowered pain thresholds in IBS.)
Live PubMed Searches
For further reading, the following PubMed topic searches return current peer-reviewed work on visceral hypersensitivity, the brain-gut axis, and related IBS neuroscience:
- Visceral hypersensitivity in IBS
- Brain-gut axis and irritable bowel syndrome
- Rectal barostat and IBS pain thresholds
- TRPV1, mast cells, and IBS
- Serotonin, 5-HT3, and IBS
- Gut-directed hypnotherapy for IBS
- Heart rate variability and vagal tone in IBS
- Central sensitization, fibromyalgia, and IBS overlap
- Adverse childhood experiences and IBS
- Tricyclic antidepressants as neuromodulators in IBS
Connections
- The Gut Barrier & Your Microbiome — interactive animation
- Irritable Bowel Syndrome
- Post-Infectious IBS
- Gut-Directed Hypnotherapy and CBT
- Low-FODMAP Diet for IBS
- IBS Medications Guide
- Peppermint, Probiotics, and Herbals
- IBS and SIBO Overlap
- Rome IV Subtypes
- Fibromyalgia
- Central Sensitization
- Chronic Pain
- POTS
- MCAS
- Chronic Fatigue Syndrome
- Endometriosis
- Pelvic Floor Therapy and Central Sensitization
- Gut-Brain Axis
- Anxiety