Gut-Directed Hypnotherapy and CBT for IBS
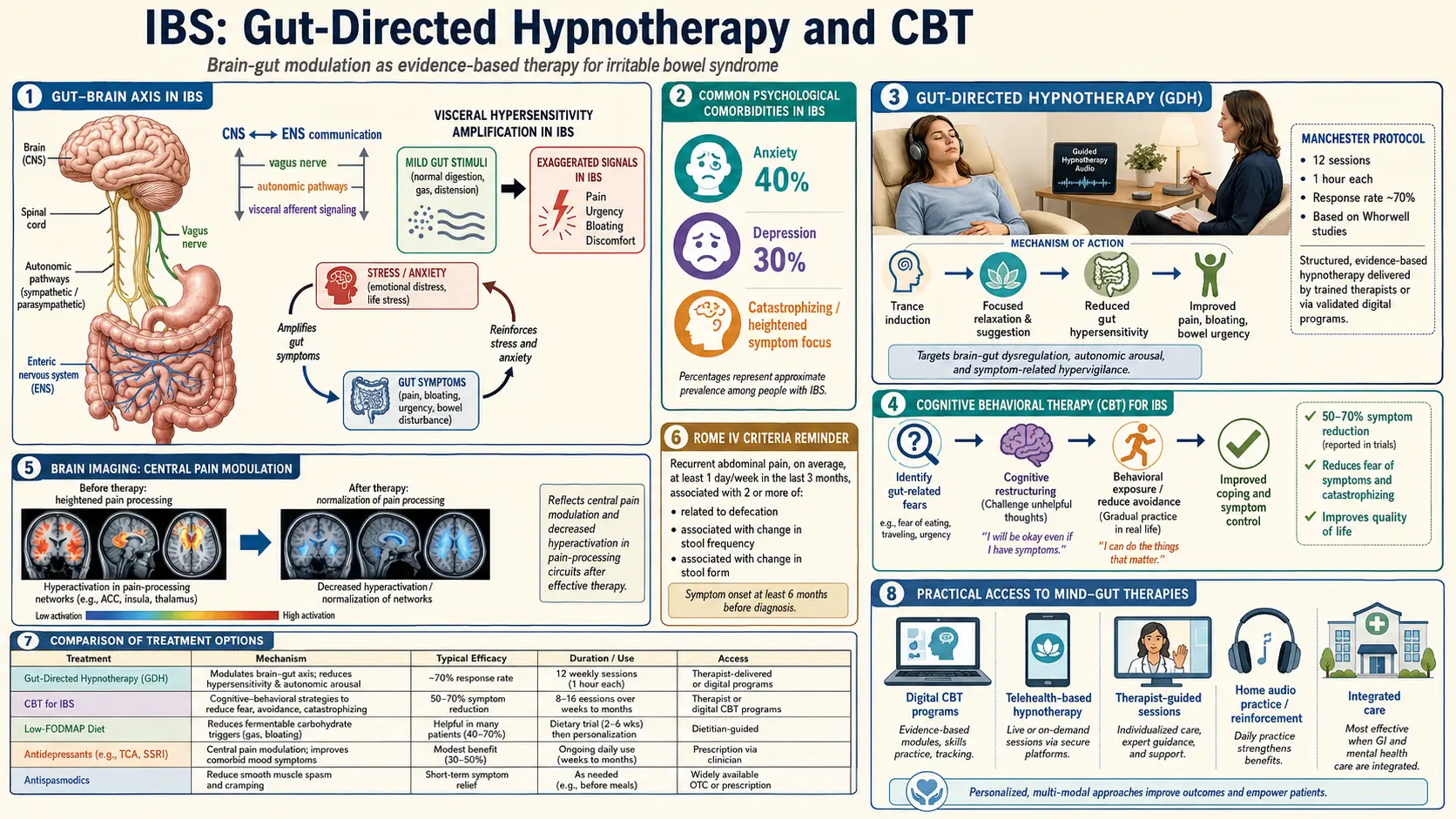
Table of Contents
- Why Mind-Body Therapies Actually Work for IBS
- The Manchester Protocol (Peter Whorwell)
- The North Carolina Protocol (Olafur Palsson)
- App-Based Delivery — Nerva, Mahana, Regulora, Zemedy
- Finding an In-Person Provider
- CBT for IBS — Not Generic Therapy
- Mindfulness-Based Stress Reduction and Yoga
- Low-Dose TCAs as Neuromodulators
- Insurance, HSA, and the Real Cost Picture
- Combining With Diet and Medication
- Realistic Expectations and Time Investment
- When It Doesn't Work — and Why
- Key Research Papers
- Connections
- Featured Videos
Why Mind-Body Therapies Actually Work for IBS
Hearing "it's stress" from a doctor is usually code for "I can't help you, now please leave." That is not what this article is about. Gut-directed hypnotherapy and cognitive behavioral therapy (CBT) are not generic relaxation. They are specific, evidence-based, outcome-measured treatments for the exact neurobiology that is broken in IBS, and in head-to-head trials they match or beat every prescription medication we have for this condition.
To understand why, start with the problem. In IBS, the nerves lining the gut are turned up too loud. Normal amounts of gas, normal stretch from a meal, normal peristalsis — sensations a healthy person never notices — register as pain, cramping, bloating, or urgency. This is called visceral hypersensitivity, and it is the subject of a sibling article (Visceral Hypersensitivity and the Brain-Gut Axis) that pairs with this one. The volume knob lives partly in the gut wall and partly in the spinal cord and brainstem, where signals from the gut are interpreted, amplified, or dampened before they ever reach conscious awareness. This amplifier is called central sensitization, and it is the same mechanism driving fibromyalgia, migraine, and chronic pelvic pain.
Gut-directed hypnotherapy works on that amplifier directly. Functional MRI studies show that hypnosis reduces activity in the anterior cingulate cortex and insula — the brain regions that convert gut signals into the conscious experience of pain. It increases vagal tone, the parasympathetic "rest and digest" signal that slows heart rate, relaxes gut smooth muscle, and down-regulates inflammatory cytokines. It shifts the autonomic nervous system out of the sympathetic "fight or flight" state that amplifies gut sensation and speeds or spasms motility. In measurable, repeatable, imaging-confirmed ways, it rewires the volume knob.
CBT works on a parallel axis. It does not claim the symptoms are imaginary. It targets the secondary layer of the disease — the fear of symptoms, the avoidance behaviors (skipping meals, canceling plans, mapping every bathroom), the catastrophic thoughts ("this pain means cancer, I need to leave") — that feed back into the nervous system and keep it sensitized. Calming those loops reliably reduces the primary symptoms too, because the gut and brain really are one circuit.
The Manchester Protocol (Peter Whorwell)
The entire modern field of gut-directed hypnotherapy traces back to one gastroenterologist: Peter Whorwell, who started treating IBS patients with hypnosis at the University of Manchester in the early 1980s because he was running out of options for the severely ill people on his ward. His 1984 paper in The Lancet was the first randomized controlled trial of hypnosis for any gastrointestinal condition, and the results were startling — nearly complete symptom resolution in the hypnosis group, essentially no improvement in controls.
The Manchester protocol is tight and reproducible:
- Seven sessions, each about 30 minutes, spaced one to two weeks apart over roughly three months.
- Each session begins with a progressive relaxation induction, then moves into gut-specific imagery. The most famous image is a gentle river flowing smoothly through the gut, warming, soothing, and normalizing its movement. Other sessions use hand-warmth imagery transferred to the abdomen, or the metaphor of a protective shield around hypersensitive nerves.
- Patients receive an audio recording of each session and practice daily self-hypnosis at home for 15 to 20 minutes between appointments. The home practice is where most of the work happens.
Manchester's published response rates run 70 to 80 percent for meaningful symptom improvement — at least a 50 percent reduction in pain, bloating, and bowel dysfunction. The most extraordinary finding came from a follow-up study by Lindfors and colleagues: at five years post-treatment, improvements were still intact in the majority of responders, with no booster sessions required. No IBS medication on the market can claim that durability.
The North Carolina Protocol (Olafur Palsson)
The Manchester approach was hard to export because it required training under Whorwell's team. In the early 2000s, Icelandic psychologist Olafur Palsson, working at the University of North Carolina, built a scripted, manualized version designed to be delivered by any trained clinician while preserving the same clinical results.
The North Carolina protocol is also seven sessions, also 30 to 40 minutes each, but it runs off written scripts. Any licensed mental health professional or certified hypnotherapist can follow the manual. This mattered enormously for access: suddenly a therapy that required flying to Manchester was available in clinics, hospitals, and eventually homes across the U.S. Trials of the Palsson scripts have replicated the Manchester-style response rates of around 70 percent, with benefits durable at one to three years.
The North Carolina protocol is also the backbone of every app-based hypnotherapy program on the market. When you use Nerva, Regulora, or similar products, you are hearing, in effect, a voice-acted and updated version of Palsson's scripts — lightly rewritten, professionally produced, and delivered on a phone instead of a clinician's couch.
App-Based Delivery — Nerva, Mahana, Regulora, Zemedy
If you cannot find a trained gut-directed hypnotherapist within 200 miles of home — and most Americans cannot — apps have closed the gap. Four programs dominate:
Nerva
Developed in Australia by Mindset Health in partnership with researchers at Monash University (the same team that created the Low-FODMAP diet). Twelve-week program, daily 15-minute hypnosis session, education modules, and a simple symptom tracker. Cost is roughly $100 to $200 for the full program depending on promotional pricing, available on iOS and Android. Peters and colleagues published an open trial in Neurogastroenterology & Motility in 2015 showing response rates in the same range as in-person Manchester hypnotherapy, which is the single most-cited validation for app-delivered gut-directed hypnotherapy.
Mahana IBS
A CBT program, not hypnotherapy. Three-month structured course built around cognitive restructuring, behavioral experiments, and symptom-exposure work. FDA De Novo cleared in 2020 as a prescription digital therapeutic, meaning your doctor writes a script and the app is regulated as a medical device. Cash price is high without insurance (hundreds of dollars), but a growing number of plans cover it and the company runs patient-assistance pricing.
Regulora
The dedicated app counterpart to Mahana — FDA-cleared, prescription-only, gut-directed hypnotherapy (not CBT). Three-month program built on the Palsson North Carolina scripts, delivered through a voice-guided mobile interface. Also covered by a growing, still-limited set of commercial insurers.
Zemedy
Another CBT-based app, available direct-to-consumer without a prescription. Broader stress-and-IBS curriculum, lower price point, somewhat lighter evidence base than Mahana but a reasonable starting point for people whose insurance will not pay for the prescription options.
Practical advice: if cost is the main barrier, start with Nerva — you can usually find a discount code, and twelve weeks of daily 15-minute sessions is the best evidence-based intervention you can self-administer for IBS. If you have decent insurance or an HSA, ask your gastroenterologist to prescribe Mahana or Regulora and fight for coverage.
Finding an In-Person Provider
Some people need a human. If you do, two directories are worth bookmarking:
- American College of Gastroenterology (ACG) patient resources — a provider finder for GI behavioral health clinicians, most of whom are Ph.D. psychologists trained in both CBT-for-IBS and gut-directed hypnotherapy.
- IBS Impact registry — a patient-run list of clinicians across the U.S., U.K., and Australia with specific gut-directed hypnotherapy training.
- The American Society of Clinical Hypnosis (ASCH) member directory will turn up certified hypnotherapists, but most are not gut-specialized. Ask two questions before booking: "Do you use the Palsson North Carolina IBS protocol?" and "Roughly how many IBS patients have you treated?" You want a three-figure answer to the second.
Expect session cost in the range of $150 to $250 per visit for a Ph.D. psychologist in a major U.S. city, less in smaller markets. The full seven-session course runs roughly $1,000 to $1,800 out of pocket — comparable to one month of rifaximin (Xifaxan) without insurance and with durability measured in years rather than weeks.
CBT for IBS — Not Generic Therapy
"I tried therapy and it didn't help my gut" is a sentence I hear constantly. Usually what the person tried was generic supportive talk therapy, which is a fine thing but is not the same intervention as CBT for IBS. The protocols differ in three specific ways.
Cognitive restructuring around symptom catastrophizing. IBS patients often run automatic thoughts like "this cramp means I'm about to have an accident in public" or "if I eat at the restaurant I will be sick for three days." CBT-for-IBS identifies these thoughts, tests them against actual evidence from the patient's own symptom diary, and teaches more accurate replacements. Over weeks, the catastrophic framing fades, and the autonomic arousal that was feeding the symptoms fades with it.
Behavioral experiments to test feared outcomes. A patient who has been avoiding restaurants for eight years believes, deep down, that restaurants cause flares. The therapist designs a graded test — first a coffee at a cafe, then a small snack, then a planned meal with a safe menu item — and the patient collects data. Most of the predicted disasters do not happen. The brain learns this, slowly, through lived experience. Reassurance alone does not accomplish this; the data collection does.
Gradual exposure to avoided foods and situations. Many IBS patients develop progressively restrictive diets and shrinking social lives that they recognize are disproportionate but cannot override alone. Exposure work reintroduces tolerable items one at a time, in a planned, paced way, while the hypersensitivity and anxiety are being treated in parallel. This layer is critical in the subset of patients whose IBS has blurred into avoidant/restrictive food intake disorder (ARFID).
Laird and colleagues published a 2016 meta-analysis in Annals of Behavioral Medicine pooling 41 CBT-for-IBS trials and found a medium-to-large effect size on symptom severity, durable at 6- to 12-month follow-up. The effect is comparable to, and in some head-to-head comparisons superior to, low-FODMAP dietary treatment alone.
Mindfulness-Based Stress Reduction and Yoga
Mindfulness-Based Stress Reduction (MBSR), the eight-week program developed by Jon Kabat-Zinn, has modest but real evidence in IBS. Trials generally show roughly 30 to 40 percent improvement in symptom severity scores — smaller than gut-directed hypnotherapy, but meaningful, and MBSR courses are widely available through hospital wellness programs, often for $200 to $400 or sometimes free through insurance wellness benefits. It is a reasonable first-line mind-body option if the specialized IBS protocols are not accessible.
Yoga has a surprisingly respectable IBS evidence base. Kavuri and colleagues (2015) reviewed the literature and found that regular Iyengar or general hatha yoga practice improved IBS symptoms roughly on par with a standard exercise program, with additional benefit in anxiety and quality of life. The mechanism is presumed to overlap with MBSR — vagal-tone elevation, parasympathetic shift, interoceptive awareness. Two to three sessions per week for eight to twelve weeks is the dosing used in most trials.
Neither MBSR nor yoga replace gut-directed hypnotherapy as the evidence leader, but both are cheap, side-effect-free, and stack well with everything else.
Low-Dose TCAs as Neuromodulators
Low-dose tricyclic antidepressants — amitriptyline, nortriptyline, desipramine at doses of 10 to 50 mg at bedtime — are among the most effective pharmacologic treatments for IBS, and they operate on the same central-sensitization target as hypnotherapy and CBT. The dose used is well below the antidepressant range; the mechanism here is pure neuromodulation of visceral pain signaling in the spinal cord and brainstem.
Clinically, TCAs pair well with behavioral therapy rather than competing with it. A reasonable sequence for a patient with painful IBS-D is: start low-dose nortriptyline or amitriptyline for faster symptom relief (within two to four weeks), simultaneously begin gut-directed hypnotherapy (which takes 8 to 12 weeks to show full effect), then taper the TCA slowly once hypnotherapy gains consolidate. Full dosing details and side-effect trade-offs are covered in the sibling article IBS Medications Guide.
Insurance, HSA, and the Real Cost Picture
The infuriating truth: insurance coverage for gut-directed hypnotherapy and CBT-for-IBS is spotty and varies wildly by plan. Commercial insurance sometimes covers sessions with a Ph.D. psychologist if coded under a mental health diagnosis (common codes: F45.8 somatic symptom disorder, F41.1 generalized anxiety disorder). Medicare covers psychotherapy but not always hypnotherapy specifically. Mahana and Regulora are increasingly reimbursed since they carry FDA device clearance, but still denied by many plans.
Two workarounds that consistently help:
- HSA and FSA accounts. App-based programs (Nerva, Zemedy, prescribed Mahana/Regulora) are reliably HSA/FSA-eligible. You can pay with pre-tax dollars even if your insurer is refusing. For a $150 Nerva subscription at a 30 percent marginal tax rate, the effective cost drops to about $105.
- Superbilling. Many GI psychologists do not take insurance directly but will provide a detailed receipt (superbill) that you submit to your plan for out-of-network reimbursement. A patient with 40 percent out-of-network coverage can often recover several hundred dollars of a seven-session course.
It is also worth doing the math on what you are already spending. A year of rifaximin rescue courses, hyoscyamine, probiotics, missed workdays, and peppermint capsules can easily exceed the cost of a full in-person hypnotherapy course that durably reduces symptoms for five-plus years.
Combining With Diet and Medication
The best-studied combination is low-FODMAP diet plus gut-directed hypnotherapy. Peters and colleagues ran a trial directly comparing the two: both produced about 70 percent response rates as monotherapy, and patients who did both did slightly better than either alone, with better quality-of-life improvement. The takeaway is they are additive, not redundant. See the sibling article Low-FODMAP Diet for IBS for the full protocol.
Combining with medication is also reasonable. Linaclotide, lubiprostone, or low-dose TCAs paired with hypnotherapy or CBT often allow medication doses to drop over time, and some patients ultimately taper off the drug entirely once the behavioral gains consolidate. Peppermint oil capsules (see Peppermint, Probiotics, and Herbals) layer in without any known interaction.
Realistic Expectations and Time Investment
Selling these therapies honestly means being clear about what they do and do not deliver.
- Meaningful improvement, not cure. Roughly 60 to 70 percent of patients who complete a full course experience at least 50 percent symptom reduction. A smaller fraction (maybe 20 to 30 percent) experience near-complete remission. A stubborn minority get little or no benefit.
- Time investment is real. Expect 6 to 12 weeks before you notice durable change, and daily practice of 15 to 30 minutes during that window. Unlike a pill, you cannot shortcut the dosing.
- Durability is the single biggest advantage. At two and five years, hypnotherapy responders retain their gains without boosters. Most drugs fade within weeks of stopping.
- The placebo response in IBS is high (around 30 to 40 percent), but hypnotherapy trials consistently beat that baseline by a wide margin. Skepticism is healthy; the evidence is strong enough to overrule it.
When It Doesn't Work — and Why
A subset of patients go through the full protocol and get little benefit. In almost every case, one of four specific situations is in play:
- Severe untreated SIBO. Small intestinal bacterial overgrowth generates real, ongoing gas, bloating, and motility dysfunction that no amount of nervous-system calming will fix until the bacterial load is reduced. If bloating is the dominant symptom, work up SIBO first (see IBS and SIBO Overlap).
- Missed IBD. Crohn's and ulcerative colitis can masquerade as IBS for years. If you have blood in the stool, nocturnal diarrhea, unexplained weight loss, iron-deficiency anemia, or an elevated fecal calprotectin, this is not IBS and the behavioral therapies will not touch it. Colonoscopy first.
- Untreated pelvic floor dysfunction. A tight, uncoordinated pelvic floor produces constipation, incomplete evacuation, and a sensation of obstruction that hypnotherapy does not treat. Anorectal manometry and pelvic-floor physical therapy come before mind-body work for this subgroup.
- Severe untreated anxiety, depression, or trauma. IBS-specific CBT is not a substitute for primary mental health treatment when a patient is in a major depressive episode, has active PTSD, or has untreated panic disorder. The correct sequence is to treat the primary psychiatric condition first (medication, trauma-focused therapy, psychiatric care), and then add the gut-directed layer once the baseline is stabilized. See Anxiety and Depression.
If none of these apply and the therapy still does not work, that is a small but real group — roughly 20 to 30 percent of IBS patients — for whom medication and diet remain the mainstays. That is not a failure of the patient; it is biological variability in a disease we still do not fully understand.
Key Research Papers
- Whorwell PJ, Prior A, Faragher EB. Controlled trial of hypnotherapy in the treatment of severe refractory irritable-bowel syndrome. Lancet. 1984.
- Lindfors P, et al. Long-term effects of hypnotherapy in patients with refractory irritable bowel syndrome — five-year follow-up. Scand J Gastroenterol. 2012.
- Peters SL, Yao CK, Philpott H, et al. Randomised clinical trial: the efficacy of gut-directed hypnotherapy is similar to that of the low FODMAP diet for the treatment of irritable bowel syndrome. Neurogastroenterol Motil. 2015.
- Laird KT, et al. Short-term and long-term efficacy of psychological therapies for irritable bowel syndrome: a systematic review and meta-analysis. Ann Behav Med. 2016.
Live PubMed Searches
For further reading, the following PubMed topic searches return current peer-reviewed work on gut-directed behavioral therapies for IBS:
- Gut-directed hypnotherapy for IBS
- Manchester protocol and the Whorwell trials
- Palsson North Carolina hypnotherapy scripts
- Cognitive behavioral therapy for IBS
- App-delivered hypnotherapy (Nerva) for IBS
- Mindfulness-Based Stress Reduction and IBS
- Yoga for IBS
- Central sensitization and visceral pain in IBS
- Vagal tone and the brain-gut axis
- Low-dose tricyclic antidepressants in IBS
Connections
- The Gut Barrier & Your Microbiome — interactive animation
- Irritable Bowel Syndrome
- IBS and SIBO Overlap
- IBS Medications Guide
- Low-FODMAP Diet for IBS
- Visceral Hypersensitivity and Brain-Gut Axis
- Peppermint, Probiotics, and Herbals
- Post-Infectious IBS
- Rome IV Subtypes
- Bile Acid Malabsorption
- Anxiety
- Depression
- Fibromyalgia
- Central Sensitization
- Chronic Pain
- Stress Management
- Gut-Brain Axis
- SIBO
- Bloating