Peppermint, Probiotics & Herbals for IBS
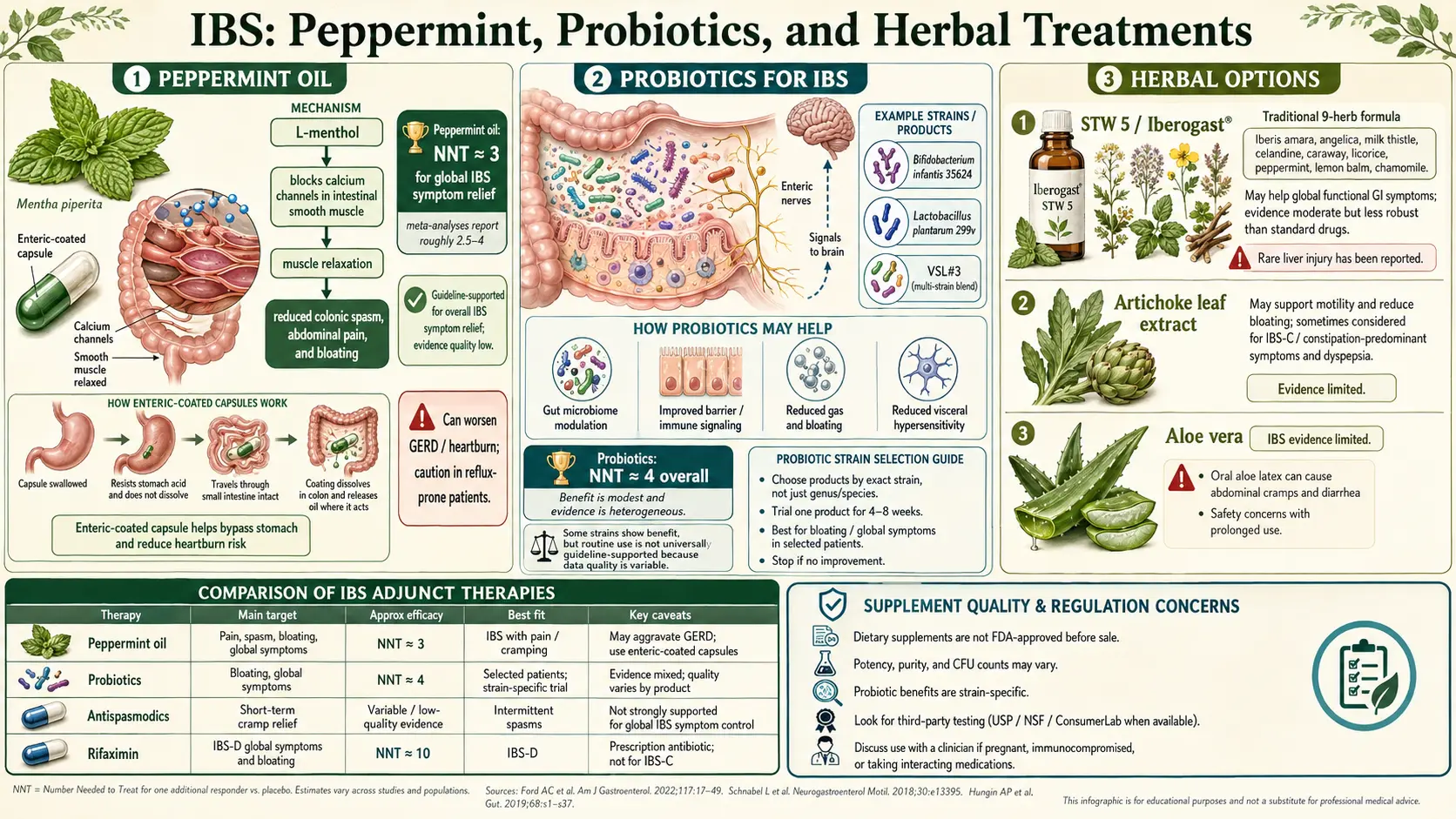
Table of Contents
- Why Patients Try the Natural Route First
- Enteric-Coated Peppermint Oil — The Best-Studied Herbal
- Peppermint Brands: IBgard, Pepogest, Mentharil
- Peppermint Side Effects & Interactions
- Probiotics — Strain Matters More Than Brand
- Bifidobacterium infantis 35624 (Align)
- VSL#3 / Visbiome: The High-Dose Multi-Strain
- Lactobacillus plantarum 299v & Symprove
- Saccharomyces boulardii & Soil-Based Bacillus
- When Probiotics Backfire: SIBO and Shelf Chaos
- Iberogast (STW 5) — The 9-Herb German Phytomedicine
- Triphala, Artichoke Leaf, Curcumin
- Slippery Elm, Marshmallow Root & the Mucilage Coaters
- Psyllium & PHGG (Sunfiber): Fiber That Actually Helps
- Prebiotics: Why FOS & Inulin Often Backfire
- Ginger, Chamomile & Fennel — Gentle Helpers
- Quality Sourcing: USP, NSF, and Avoiding Junk
- Pregnancy-Safe Options
- When Natural Isn't Enough
- Key Research Papers
- Connections
- Featured Videos
Why Patients Try the Natural Route First
If you have IBS, there is a very good chance the first thing you tried was not a prescription drug. You went to the health-food store, you asked a friend, you searched online. You came home with a bottle of peppermint capsules, or a probiotic with fifty billion CFU on the label, or a bitter German tincture your grandmother swore by. Some of these things have strong evidence behind them. Some do almost nothing. A few can actively make IBS worse. This article sorts them out.
The good news: for mild-to-moderate IBS, the best herbal and probiotic options are backed by real randomized trials, have favorable safety profiles, and often cost less than a month of prescription antispasmodics. The American Gastroenterological Association (AGA) formally endorses enteric-coated peppermint oil with a conditional recommendation, and specific probiotic strains have placebo-controlled data going back two decades.
The bad news: most products on a typical supplement shelf are unstudied, underdosed, or contain strains that have no IBS evidence at all. "Natural" is not a synonym for "works." Getting results means matching the right compound, in the right form, at the right dose, to your particular IBS subtype.
Enteric-Coated Peppermint Oil — The Best-Studied Herbal
Peppermint oil is the single most rigorously studied herbal therapy in all of IBS. The active compound is L-menthol, which blocks calcium channels in smooth muscle, relaxing gut spasm. It also has mild anti-inflammatory, antimicrobial, and visceral-pain-dulling effects. In plain language: it quiets a cramping gut and turns down the volume on pain signals traveling from bowel to brain.
The Khanna et al. 2014 meta-analysis in BMJ pooled nine randomized trials (726 patients) and found peppermint oil significantly superior to placebo for global IBS symptom improvement, with a number-needed-to-treat (NNT) of about 3. That is an extraordinary number. Most IBS drugs have NNTs of 7–12. An NNT of 3 means that for every three patients who take enteric-coated peppermint oil, one will get meaningful symptom relief they would not have gotten from placebo alone.
The AGA 2022 clinical practice guideline on pharmacological management of IBS issued a conditional recommendation in favor of peppermint oil for global IBS symptoms. The word "conditional" reflects modest evidence quality (small trials, short durations), not weak benefit.
Two details matter enormously:
- Enteric coating is non-negotiable. Uncoated peppermint oil (peppermint tea, peppermint candy, a drop of essential oil) dissolves in the stomach, where menthol relaxes the lower esophageal sphincter and worsens reflux. The enteric coat keeps the capsule intact through the stomach so it releases in the small intestine, where the spasm actually lives.
- Small-bowel-targeted release is even better. Some formulations (notably IBgard) use microsphere technology that disperses the oil gradually across the small and large intestine rather than dumping it all at once. This reduces heartburn and may improve efficacy.
The classic dose is 180–225 mg three times a day, taken 30–60 minutes before meals. Studies run 4–12 weeks, and most patients who respond notice benefit within 2–4 weeks. If nothing has changed after a month, it is probably not going to.
Peppermint Brands: IBgard, Pepogest, Mentharil
- IBgard. U.S.-market leader, uses patented Site-Specific Targeted Release (SST) microspheres. 90 mg per capsule, dosed as 2 capsules three times daily (540 mg/day total). Has the most placebo-controlled U.S. trial data (Cash et al. 2016, IBSREST trial). Available over-the-counter.
- Pepogest. Nature's Way, simple enteric-coated softgels, 0.2 mL peppermint oil per capsule. Cheaper than IBgard, dosed 1–2 capsules three times daily. Works well for most patients; the traditional coating means less small-bowel targeting.
- Mentharil. European formulation (common in Italy, Germany, UK), enteric-coated, often combined with caraway oil. Similar mechanism, similar dosing.
- Heather's Tummy Tamers. Enteric-coated capsules combining peppermint oil with fennel and ginger. A reasonable option if you want the three-herb synergy in one pill.
Generic enteric-coated peppermint oil capsules from reputable brands (NOW Foods, Solaray) are also fine and considerably cheaper. What matters is enteric coating and adequate dose, not the brand name.
Peppermint Side Effects & Interactions
Peppermint oil is well tolerated by most people, but the side effects are worth knowing before you start:
- Heartburn. Even with enteric coating, some capsules release early. If you have pre-existing GERD or a hiatal hernia, peppermint oil can make reflux worse and is generally not recommended.
- Anal burning. Undigested menthol that reaches the rectum can cause a disconcerting but harmless burning sensation during defecation. If this happens, try a different brand with better small-bowel targeting (IBgard) or lower the dose.
- Allergic contact mouth irritation. Rare.
- Drug interactions. Peppermint oil inhibits CYP3A4 in gut and liver, which can raise blood levels of several important drugs. The best-documented interactions are with cyclosporine (transplant immunosuppressant) and felodipine (calcium-channel blocker). Peppermint oil can also modestly increase levels of statins metabolized by 3A4 (simvastatin, lovastatin). If you take any of these, run peppermint by your pharmacist first.
- Iron absorption. Peppermint may reduce non-heme iron absorption when taken with meals — minor, but worth spacing from iron supplements.
Probiotics — Strain Matters More Than Brand
The single most important thing to understand about probiotics is that evidence applies to specific strains, not to "probiotics" in general. Bifidobacterium infantis 35624 has been tested in IBS. Your friend's "50 billion CFU multi-strain blend" with a dozen unlabeled species has not. The labels look similar. The evidence is not.
A useful rule: if the product label does not tell you the exact strain (the numbers or letters after the species name, e.g., "Lactobacillus plantarum 299v" or "Bifidobacterium lactis BB-12"), assume there is no clinical trial data supporting it for IBS. Big CFU counts are marketing. A well-studied strain at 1 billion CFU beats a random blend at 100 billion.
Bifidobacterium infantis 35624 (Align)
The most-studied single probiotic strain in all of IBS. The landmark trial was O'Mahony et al. 2005 in Gastroenterology, which randomized 77 IBS patients to B. infantis 35624 at 1 × 108 CFU per day, Lactobacillus salivarius UCC4331, or placebo for eight weeks. B. infantis produced statistically significant improvements in abdominal pain, bloating, bowel-habit difficulty, and composite symptom score. The L. salivarius arm did not separate from placebo.
Mechanistically, B. infantis 35624 modulates the gut's innate immune system, reduces pro-inflammatory cytokines (notably IL-6 and TNF-alpha), and appears to reinforce epithelial barrier function. This is the rare strain with plausible mechanism, replicated clinical benefit, and broad symptom coverage across IBS subtypes.
It is sold in the U.S. as Align Daily Probiotic (Procter & Gamble), one capsule a day. Outside the U.S. the same strain appears in the Bifantis line and some generics. Give it 4–6 weeks before judging. It does not need refrigeration.
VSL#3 / Visbiome: The High-Dose Multi-Strain
VSL#3 was the original high-potency 8-strain formulation developed by Prof. Claudio De Simone. In 2016 a manufacturing dispute split the product: the original formula now ships as Visbiome (containing the De Simone Formulation), while "VSL#3" is a reformulated version sold by the original licensee. For trial evidence matching the published literature, choose Visbiome.
The blend contains four Lactobacillus strains, three Bifidobacterium strains, and Streptococcus thermophilus, at 450 billion CFU per sachet. It has stronger evidence in ulcerative colitis and pouchitis than in IBS, but small trials do support modest benefit in IBS-D with bloating. It is expensive (~$50–$100/month), requires refrigeration, and is overkill for mild IBS. Reserve it for refractory patients, patients with overlapping IBD, or those who have tried simpler options without success.
Lactobacillus plantarum 299v & Symprove
If pain is your dominant IBS symptom, Lactobacillus plantarum 299v deserves a look. Niedzielin et al. 2001 and Ducrotté et al. 2012 both showed significant reductions in abdominal pain and bloating with 10 billion CFU daily over four weeks. It is sold as Jarrow Ideal Bowel Support in the U.S. and ProViva in Scandinavia.
Symprove is a UK liquid multi-strain probiotic (four strains in a barley-based solution) with a positive 2014 King's College London trial in IBS and a growing user base. It is delivered in liquid form specifically to bypass stomach acid without entering spore dormancy. Pricey and mostly a UK/EU product, but well-reviewed by patients who have failed capsule products.
Saccharomyces boulardii & Soil-Based Bacillus
Saccharomyces boulardii is a non-pathogenic yeast, not a bacterium, which means antibiotics do not kill it. That makes it the probiotic of choice for post-antibiotic diarrhea and Clostridioides difficile prevention, and a reasonable adjunct for IBS-D patients who get worse after every antibiotic course. Typical dose: 250–500 mg twice daily. Brands: Florastor, Jarrow S. boulardii + MOS.
Soil-based organisms (SBOs), typically Bacillus species packaged as spores (MegaSporeBiotic, Just Thrive, HU58), are a newer category. Because the spores are heat- and acid-stable, they survive transit and germinate in the colon. A 2019 pilot study (McFarlin et al.) showed reductions in endotoxemia after a high-fat meal, and a 2021 trial in IBS-D suggested symptom benefit. Evidence is promising but not yet at the level of Align or L. plantarum 299v. Worth trying if mainstream probiotics have failed.
When Probiotics Backfire: SIBO and Shelf Chaos
Two important cautions:
- Active SIBO. If you have untreated small intestinal bacterial overgrowth, loading more bacteria into an already overgrown small bowel can worsen bloating and gas. The typical pattern: the patient takes a multi-strain Lactobacillus probiotic and reports feeling "eight months pregnant" within a week. Treat the SIBO first (see herbal antimicrobials for SIBO), then add probiotics. Spore-based Bacillus and S. boulardii tend to be better tolerated during active SIBO than Lactobacillus-heavy products.
- Shelf chaos. The probiotic section of a typical American pharmacy contains perhaps 50 products. Of those, five have IBS-specific randomized trial data. The rest are wishful thinking. Skip CFU-count bragging, multi-strain megablends with no named strain numbers, and anything marketed as "immune support" rather than digestive.
Iberogast (STW 5) — The 9-Herb German Phytomedicine
Iberogast is a liquid herbal extract combining nine plants: bitter candytuft (Iberis amara), angelica root, chamomile flower, caraway fruit, milk thistle fruit, lemon balm, peppermint leaf, greater celandine, and licorice root. It was developed in Germany in the 1960s and is now sold over-the-counter across Europe, Canada, and online in the U.S.
The reference trial is Rösch et al. 1995, a multicenter double-blind RCT comparing Iberogast with metoclopramide and placebo in functional dyspepsia. Later trials extended the evidence into IBS. A 2007 meta-analysis (Melzer et al.) pooled four randomized trials and found significant benefit over placebo for abdominal pain and overall GI symptoms.
Mechanistically, Iberogast is interesting because it is region-selective: it relaxes the fundus of the stomach (helping fullness and bloating) while tonifying the antrum and small bowel (improving motility and reducing cramping). It is not simply an antispasmodic.
Dose: 20 drops in water, three times a day with meals. Taste: intensely bitter. A rare hepatotoxicity signal was flagged in European pharmacovigilance around 2018, leading to the removal of greater celandine from the formulation in some markets — check the label. Avoid if you have liver disease. Avoid in pregnancy because of the licorice component.
Triphala, Artichoke Leaf, Curcumin
Triphala is an Ayurvedic combination of three fruits — amalaki (Emblica officinalis), bibhitaki (Terminalia bellirica), and haritaki (Terminalia chebula). In IBS it is most useful for the IBS-C pattern: gentle stool softening, mild prokinetic effect, and antioxidant/anti-inflammatory properties in the gut lining. Typical dose: 500 mg to 1 g twice daily, taken with water on an empty stomach. A 2017 RCT in functional constipation showed meaningful improvement in stool frequency. Start low; higher doses loosen stool noticeably.
Artichoke leaf extract (Cynara scolymus) is a choleretic: it stimulates bile flow. In IBS, it has small positive trials (Bundy et al. 2004 and others) for reducing overall symptoms, particularly when the patient's pattern includes fat intolerance, post-meal heaviness, or overlapping functional dyspepsia. Dose: 320–640 mg of standardized extract twice daily with meals. Avoid if you have gallstones or biliary obstruction.
Curcumin, the active polyphenol in turmeric, has mild anti-inflammatory effects in the gut. Human IBS trial data are mixed — some positive small trials, some null. It is not a primary therapy but can be added if there is an inflammatory flavor to the symptoms (overlapping post-infectious IBS, low-grade colonic inflammation). Use a bioavailability-enhanced form (Meriva, Theracurmin, or curcumin with piperine) at 500–1000 mg daily. See turmeric.
Slippery Elm, Marshmallow Root & the Mucilage Coaters
Mucilage-rich herbs swell in water into a soothing gel that coats the intestinal lining. They are particularly helpful for IBS-D with burning, tenderness, or rawness — the sensation of an irritated bowel that reacts to every meal.
- Slippery elm (Ulmus rubra) — 1 teaspoon powder stirred into warm water, twice daily; or 400–500 mg capsules two to three times daily. Mild, safe, and traditional for gut irritation.
- Marshmallow root (Althaea officinalis) — cold-water infusion: 1 tablespoon dried root in a cup of cold water overnight, strained in the morning, sipped throughout the day. Very soothing.
- DGL (deglycyrrhizinated licorice) — more often used for reflux and gastritis than IBS, but helps patients with overlapping upper-GI irritation.
Mucilage herbs can delay absorption of medications taken at the same time. Space by at least two hours from any prescription.
Psyllium & PHGG (Sunfiber): Fiber That Actually Helps
Fiber is the most misunderstood intervention in IBS. The wrong kind makes IBS worse. The right kind is one of the most evidence-based remedies we have.
Soluble fiber is helpful. Insoluble fiber is often harmful. Bran, the most commonly recommended "IBS fiber" for decades, is insoluble and routinely worsens pain and bloating. Soluble fiber — psyllium, PHGG, oat beta-glucan — gels in the gut, normalizes transit in both directions (helps IBS-C and IBS-D), and feeds beneficial bacteria gently.
- Psyllium (ispaghula husk, Metamucil, Konsyl). Start 1 teaspoon in 8 oz of water once daily and increase over 2–3 weeks to 1–2 tablespoons daily as tolerated. Expect a brief increase in gas during the first week; push through or lower the dose. Multiple RCTs show benefit in global IBS symptoms. Choose plain psyllium powder over flavored capsules for cost and dose flexibility.
- Partially hydrolyzed guar gum (PHGG), sold as Sunfiber, Regular Girl, or similar. Tasteless, nearly invisible in water, and exceptionally well-tolerated. PHGG is a prebiotic but, unlike inulin and FOS, it ferments slowly and does not cause the bloat-and-gas cascade. 5–10 g/day in water, juice, or food. Strong evidence in both IBS-C and IBS-D, and it is the one prebiotic most SIBO-prone patients can actually take.
Prebiotics: Why FOS & Inulin Often Backfire
Prebiotics are fibers that feed gut bacteria. In theory, that sounds wonderful. In IBS, many of them are disastrous. Fructo-oligosaccharides (FOS) and inulin — the most common commercial prebiotics, added to everything from protein bars to yogurt — ferment rapidly in the small bowel. In an IBS patient, especially one with SIBO overlap, this produces exactly the gas and bloating the patient is trying to escape.
If you need a prebiotic, use PHGG (Sunfiber). It is the slowest-fermenting option in the category and the only one routinely tolerated by IBS patients. Start low and titrate.
Ginger, Chamomile & Fennel — Gentle Helpers
- Ginger. Excellent for nausea and upper-GI dysmotility, less for lower-bowel pain. Useful in IBS-C with bloating or nausea. Fresh ginger tea (1-inch slice steeped 10 minutes), capsules 500–1000 mg, or candied ginger all work. Mild blood-thinning effect — be cautious if on anticoagulants.
- Chamomile. Gentle antispasmodic, mild anxiolytic, and anti-inflammatory. Helpful at bedtime for patients whose IBS flares with stress. A ragweed-allergic patient can occasionally react. Strong tea 2–3 times daily.
- Fennel seed. Chewing a teaspoon of fennel seeds after a meal is a 3000-year-old remedy for bloat and gas, and there is modest modern trial data behind it. A fennel-curcumin combination showed benefit in a 2016 IBS RCT (Portincasa et al.) Fennel seed tea is also pleasant and safe.
Quality Sourcing: USP, NSF, and Avoiding Junk
Supplements are not regulated as drugs. Independent testing has repeatedly shown products that contain less active ingredient than labeled, different ingredients than labeled, or contamination with heavy metals, pesticides, and mystery fillers. The way to manage this is third-party certification:
- USP Verified — the strictest pharmaceutical-grade standard.
- NSF Certified for Sport — tests for banned substances and contaminants; slightly different scope but excellent quality floor.
- ConsumerLab and Labdoor — independent subscription testing services that publish brand-by-brand analyses.
- TrustedSource / GMP-certified — minimum baseline for manufacturing hygiene, not potency.
For probiotics specifically, check the label for guaranteed CFU at expiration, not at manufacture — live organisms die on the shelf, and "50 billion CFU at manufacture" may be 10 billion by the time you buy it.
Pregnancy-Safe Options
Most IBS herbals have not been formally tested in pregnancy, so the conservative default is to avoid. A few options are generally considered safe; always confirm with your obstetrician.
- Ginger — well-studied and considered safe at food-level doses; helps both nausea and IBS cramping. Avoid high-dose ginger supplements.
- Psyllium — safe and often recommended in pregnancy.
- PHGG (Sunfiber) — considered safe.
- Align (B. infantis 35624) — probiotics broadly have excellent pregnancy safety data.
Avoid during pregnancy: Iberogast (contains licorice), triphala, high-dose curcumin, senna-based laxatives, greater celandine, and large-dose peppermint oil (small culinary amounts fine). Essential oils used internally are generally discouraged.
When Natural Isn't Enough
Herbals and probiotics are first-line for mild to moderate IBS. They are not enough, and waiting on them is actively harmful, when any of the following are present:
- Red-flag symptoms: unintentional weight loss, rectal bleeding, nocturnal diarrhea that wakes you from sleep, iron-deficiency anemia, fever, a family history of colorectal cancer or IBD, new-onset symptoms after age 50. These require prompt gastroenterology evaluation — colonoscopy, imaging, calprotectin testing — before anything else.
- Severe IBS-D with accidents, housebound behavior, or inability to work. Natural therapies can help long-term but short-term you may need rifaximin, eluxadoline, or a bile-acid sequestrant. See the medications guide.
- IBS-IBD overlap. Elevated fecal calprotectin, abnormal imaging, or iron deficiency all point toward inflammatory bowel disease hiding behind an IBS label. Peppermint oil will not treat Crohn's disease or ulcerative colitis.
- Severe depression or anxiety driving IBS symptoms. Gut-directed hypnotherapy and CBT plus, where needed, prescription neuromodulators outperform any herbal in this subset.
A reasonable workflow: if you have clean labs, no red flags, and mild-to-moderate IBS, give an evidence-based herbal + probiotic stack (peppermint oil + Align + PHGG) a full 6–8 week trial. Layer in Iberogast or triphala if needed. If you are not meaningfully better by week eight, escalate to the medication guide and consider workup for SIBO overlap or post-infectious triggers.
Key Research Papers
- Khanna R, MacDonald JK, Levesque BG. Peppermint oil for the treatment of irritable bowel syndrome: a systematic review and meta-analysis. BMJ. 2014.
- O'Mahony L, et al. Lactobacillus and Bifidobacterium in irritable bowel syndrome: symptom responses and relationship to cytokine profiles. Gastroenterology. 2005.
- Whorwell PJ, et al. Efficacy of an encapsulated probiotic Bifidobacterium infantis 35624 in women with irritable bowel syndrome. Am J Gastroenterol. 2006. (Also covers L. plantarum 299v comparisons in related trials.)
- Rösch W, et al. A multicenter, randomized, double-blind, placebo-controlled study of the efficacy of STW 5 (Iberogast) in patients with functional dyspepsia. Z Gastroenterol. 1995. (Foundational Iberogast trial; no DOI assigned.)
Live PubMed Searches
For further reading, the following PubMed topic searches return current peer-reviewed work on herbal and probiotic therapy for IBS:
- Peppermint oil RCTs in IBS
- Bifidobacterium infantis 35624 and IBS
- Lactobacillus plantarum 299v and IBS
- Iberogast (STW 5) functional GI trials
- Psyllium in IBS
- Partially hydrolyzed guar gum (PHGG/Sunfiber) in IBS
- Triphala and functional constipation
- Saccharomyces boulardii in IBS and antibiotic-associated diarrhea
- Soil-based Bacillus spore probiotics in IBS
- Artichoke leaf extract in IBS and functional dyspepsia
Connections
- The Gut Barrier & Your Microbiome — interactive animation
- Irritable Bowel Syndrome
- SIBO
- Herbal Antimicrobials
- Peppermint
- Ginger
- Turmeric
- Fennel
- Chamomile
- Probiotics
- Post-Infectious IBS
- IBS and SIBO Overlap
- IBS Medications Guide
- Low-FODMAP Diet for IBS
- Visceral Hypersensitivity and Brain-Gut Axis
- Gut-Directed Hypnotherapy and CBT
- Ulcerative Colitis
- Crohn's Disease
- Bloating