Vitamin B9 (Folate): The Methylation, Cell Division, and Life-Building Vitamin
Vitamin B9, known naturally as folate (from the Latin "folium" meaning "leaf"), is a water-soluble B vitamin that plays an absolutely central role in some of the most fundamental processes of life — DNA synthesis, cellular division, methylation, and the development of new life itself. In natural medicine, folate is regarded as one of the most critical and commonly deficient nutrients, with far-reaching consequences that extend from the earliest moments of embryonic development to cardiovascular health, mental well-being, cancer prevention, and healthy aging. It is essential to distinguish between natural folate (found in whole foods and as the supplement forms 5-MTHF and folinic acid) and synthetic folic acid (the oxidized, man-made form added to fortified foods and many cheap supplements), as these behave very differently in the body — a distinction of paramount importance to natural practitioners.
Interactive Visualization The Methylation Cycle — hand off a methyl group Watch folate and B12 recycle homocysteine into methionine — then knock out B12 and see the folate trap slam shut. Launch →Table of Contents
- DNA Synthesis, Repair, and Cell Division
- Methylation — The Master Biochemical Switch
- Pregnancy, Neural Tube Defects, and Fetal Development
- Cardiovascular Health — Homocysteine Management
- Mental Health — Depression, Anxiety, and Cognitive Function
- Red Blood Cell Formation and Megaloblastic Anemia
- Cancer Prevention
- The MTHFR Gene — A Critical Genetic Consideration
- Folate vs. Folic Acid — A Critical Distinction
- Immune System Support
- Liver Health and Detoxification
- Gut Health
- Bone Health
- Natural Food Sources
- Recommended Daily Intake
- Supplemental Forms
- Synergistic Nutrients
- Populations at Higher Risk of Deficiency
- Signs of Deficiency
- Special Therapeutic Applications
- Connections
- Featured Videos
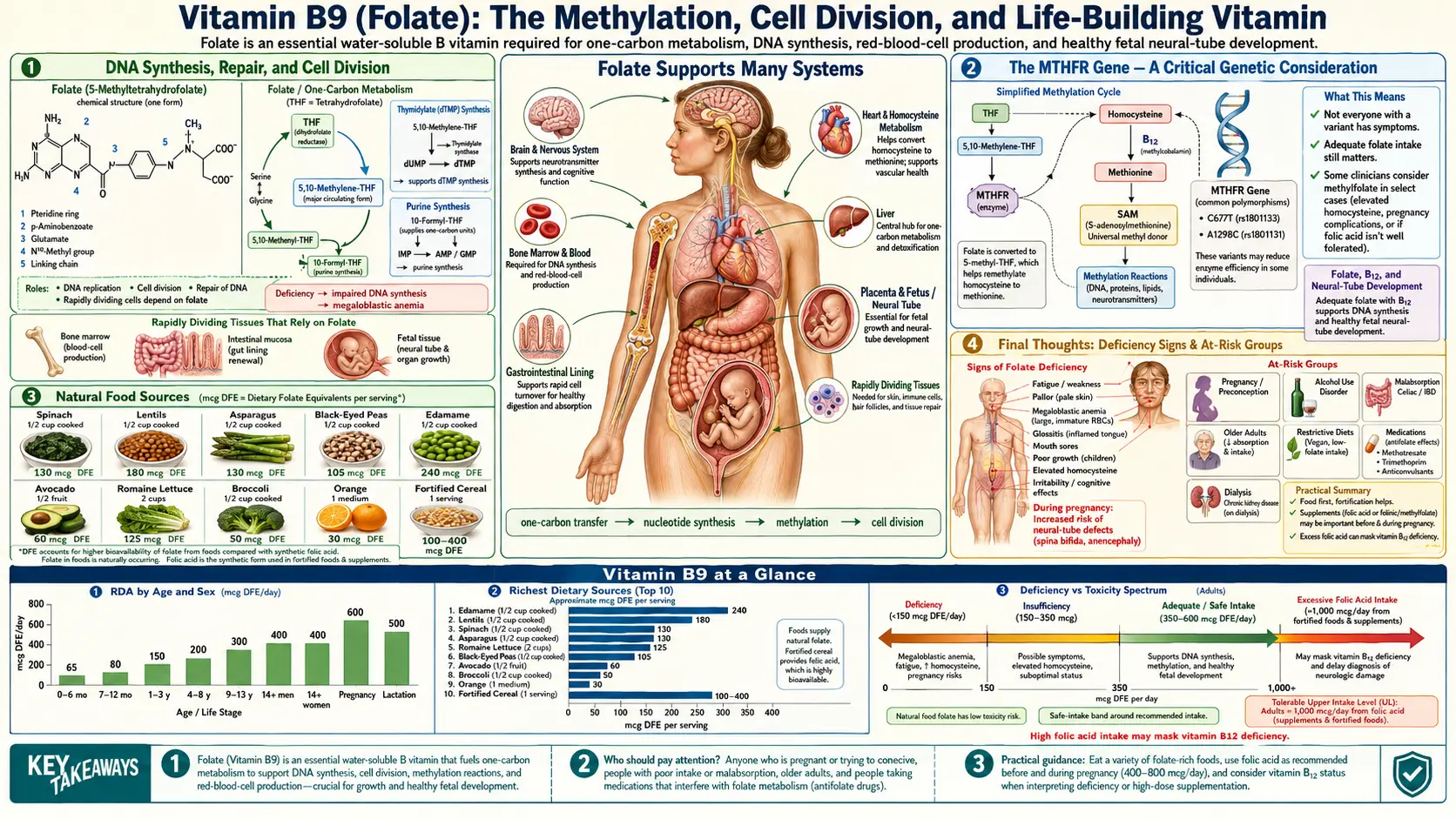
1. DNA Synthesis, Repair, and Cell Division
Folate is indispensable for the creation and maintenance of the genetic blueprint of every cell in the body.
- Thymidylate Synthesis: Folate, in the form of 5,10-methylenetetrahydrofolate, is the essential cofactor for thymidylate synthase, the enzyme that produces thymidine — one of the four nucleotide bases of DNA. Without folate, the body literally cannot build new DNA strands.
- Purine Synthesis: Folate coenzymes are required for two separate steps in the de novo synthesis of purines (adenine and guanine) — the other two DNA bases. Together, this means that folate is required for the production of three of the four building blocks of DNA.
- RNA Synthesis: The same pathways that produce DNA precursors also generate the nucleotides needed for RNA synthesis, making folate essential for protein production and gene expression throughout the body.
- Cell Division: Every cell that divides — whether it is an immune cell responding to infection, a red blood cell forming in the bone marrow, a gut epithelial cell renewing the intestinal lining, or an embryonic cell building a new human being — requires folate. Tissues with rapid turnover are the most vulnerable to folate deficiency.
- DNA Repair: Folate supports the repair of damaged DNA, helping to maintain genomic stability and prevent the accumulation of mutations that can lead to cellular dysfunction and malignant transformation.
- Uracil Misincorporation: When folate is deficient, the cell cannot produce sufficient thymidine, and uracil (an RNA base) is mistakenly incorporated into DNA in its place. This causes DNA strand breaks, chromosomal instability, and increased mutation rates — a direct mechanism linking folate deficiency to cancer risk.
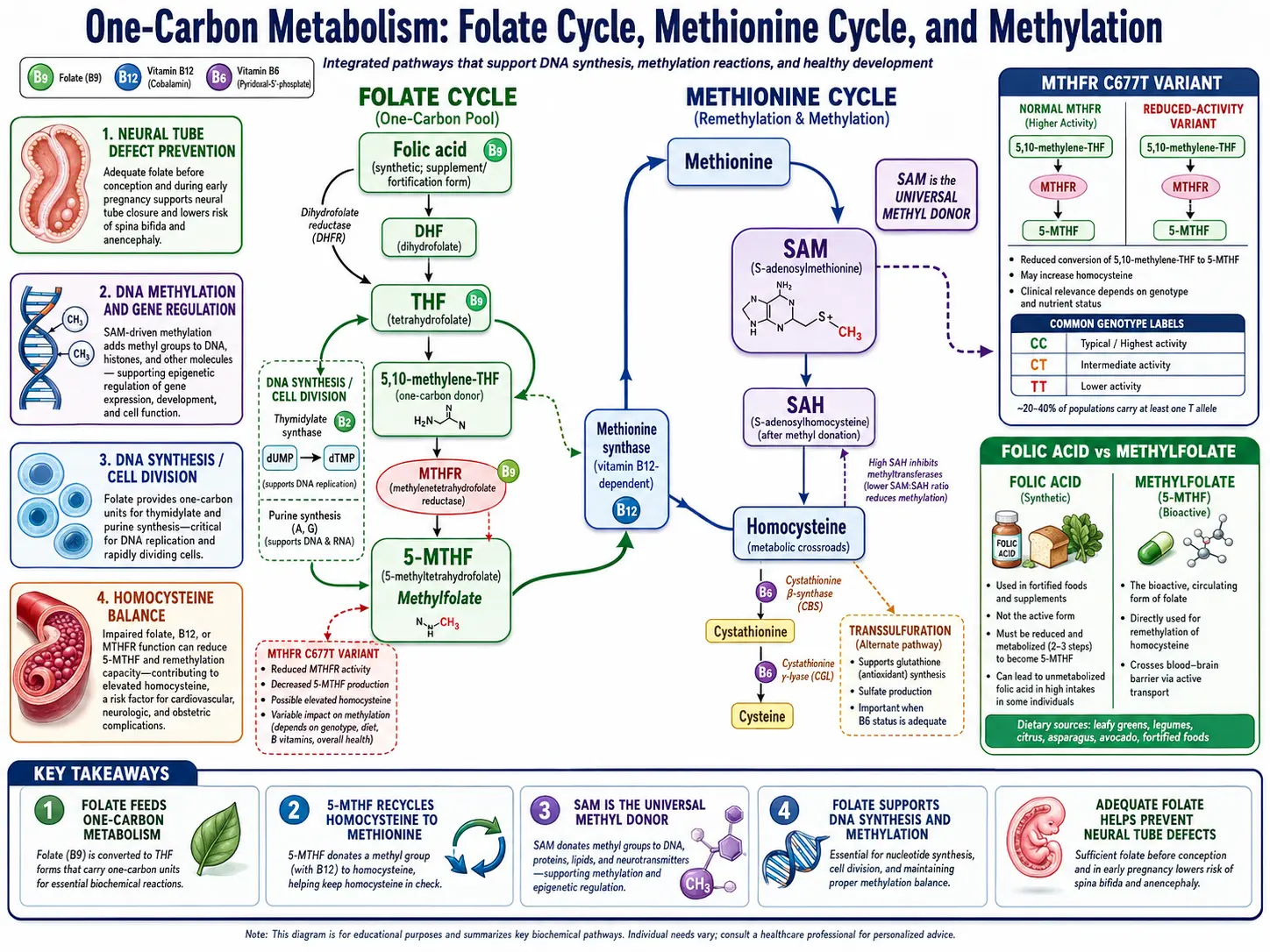
2. Methylation — The Master Biochemical Switch
Folate sits at the very heart of the body's methylation cycle — one of the most critical and far-reaching biochemical processes in human physiology.
- The Methylation Cycle: Folate, in its active form 5-methyltetrahydrofolate (5-MTHF), donates a methyl group to homocysteine, converting it to methionine through the enzyme methionine synthase (which requires Vitamin B12 as a cofactor). Methionine is then converted to S-adenosylmethionine (SAMe) — the body's universal methyl donor.
- SAMe and Methyl Transfers: SAMe donates methyl groups to over 200 different substrates in the body, including DNA, RNA, proteins, phospholipids, neurotransmitters, hormones, and creatine. Methylation is involved in virtually every aspect of cellular function.
- DNA Methylation and Epigenetics: The methylation of DNA is the primary mechanism by which genes are turned on and off — the foundation of epigenetic regulation. Proper folate status ensures healthy gene expression patterns, while deficiency leads to aberrant DNA methylation associated with cancer, developmental disorders, and aging.
- Neurotransmitter Methylation: The synthesis and metabolism of serotonin, dopamine, norepinephrine, and melatonin all require methylation reactions that depend on adequate folate.
- Phospholipid Methylation: The synthesis of phosphatidylcholine — the most abundant phospholipid in cell membranes — requires SAMe-dependent methylation. This links folate directly to cell membrane integrity, liver health, and bile production.
- Creatine Synthesis: Creatine production consumes a large portion of the body's daily SAMe output. Adequate folate ensures sufficient methyl group supply for creatine synthesis without compromising other methylation demands.
- Histamine and Estrogen Clearance: Methylation is required for the inactivation and clearance of histamine (via histamine N-methyltransferase) and estrogen metabolites (via catechol-O-methyltransferase, COMT). Poor methylation capacity — often rooted in folate insufficiency — can contribute to histamine intolerance and estrogen dominance.
3. Pregnancy, Neural Tube Defects, and Fetal Development
Folate's role in pregnancy and fetal development is perhaps its most widely recognized and critically important function.
- Neural Tube Closure: The neural tube — the embryonic structure that becomes the brain and spinal cord — closes between days 21 and 28 after conception, often before a woman even knows she is pregnant. Adequate folate during this critical window is essential for proper closure. Deficiency causes devastating birth defects including spina bifida (incomplete closure of the spinal cord), anencephaly (absence of major portions of the brain), and encephalocele (brain tissue protruding through the skull).
- Preconception Supplementation: Because the neural tube closes so early, natural practitioners strongly recommend that all women of childbearing age maintain adequate folate status continuously — not just after a positive pregnancy test. Supplementation should ideally begin at least 3 months before conception.
- Congenital Heart Defects: Adequate folate status has been associated with reduced risk of congenital heart malformations, the most common type of birth defect.
- Cleft Lip and Palate: Folate sufficiency during early pregnancy is associated with reduced risk of orofacial clefts.
- Placental Development: Folate supports the rapid cell division required for healthy placental growth and function, ensuring adequate nutrient and oxygen delivery to the developing fetus.
- Preterm Birth and Low Birth Weight: Low maternal folate status is associated with increased risk of preterm delivery and intrauterine growth restriction.
- Preeclampsia Risk Reduction: Adequate folate, through its homocysteine-lowering and endothelial-protective effects, may help reduce the risk of preeclampsia — a dangerous pregnancy complication characterized by high blood pressure and organ damage.
- Autism Spectrum Considerations: Emerging epidemiological research suggests that adequate periconceptional folate may be associated with reduced risk of autism spectrum disorder, though this remains an area of active investigation.
4. Cardiovascular Health — Homocysteine Management
Folate is the most potent dietary regulator of homocysteine levels, making it a cornerstone nutrient for cardiovascular protection.
- Homocysteine Remethylation: 5-MTHF donates a methyl group to homocysteine, converting it back to methionine through methionine synthase (B12-dependent). This is the body's primary pathway for homocysteine clearance and recycling.
- Cardiovascular Risk: Elevated homocysteine is an independent risk factor for atherosclerosis, coronary artery disease, heart attack, stroke, peripheral vascular disease, and venous thromboembolism. Folate supplementation is the single most effective nutritional intervention for reducing homocysteine levels.
- Endothelial Function: Homocysteine directly damages the endothelial lining of blood vessels, promoting oxidative stress, inflammation, and plaque formation. By maintaining low homocysteine, folate preserves vascular integrity and function.
- Nitric Oxide Production: Folate (as 5-MTHF) has been shown to enhance endothelial nitric oxide synthase (eNOS) activity, increasing nitric oxide production — a vasodilator that promotes healthy blood flow and blood pressure regulation.
- Blood Pressure: Adequate folate intake is associated with lower blood pressure, particularly in individuals with MTHFR polymorphisms or elevated homocysteine.
- Stroke Prevention: Meta-analyses of clinical trials have consistently shown that folate supplementation reduces stroke risk, particularly in populations without mandatory folic acid food fortification.
- The Triad: Optimal homocysteine management requires the synergistic action of folate, Vitamin B12, and Vitamin B6. All three must be sufficient for the homocysteine recycling and clearance pathways to function properly.
5. Mental Health — Depression, Anxiety, and Cognitive Function
Folate's role in mental health is profound, well-documented, and increasingly recognized by both natural and conventional medicine.
- Serotonin Synthesis: Folate-dependent methylation is required for the regeneration of tetrahydrobiopterin (BH4) — an essential cofactor for the enzymes that produce serotonin, dopamine, and norepinephrine. Without adequate folate, BH4 recycling is impaired and neurotransmitter synthesis declines.
- SAMe and Mood: SAMe, produced through the folate-dependent methylation cycle, is itself a well-researched natural antidepressant that promotes serotonin, dopamine, and norepinephrine synthesis. Folate deficiency reduces SAMe production, directly impairing mood regulation.
- Depression Prevalence: Low folate status is one of the most consistently observed nutritional findings in individuals with major depressive disorder. Studies estimate that up to one-third of depressed patients have low folate levels.
- L-Methylfolate as Adjunctive Therapy: The active form of folate, L-methylfolate (5-MTHF), has been approved in prescription form (Deplin) as an adjunctive treatment for major depressive disorder in patients who respond poorly to SSRI antidepressants alone. Clinical trials have demonstrated significant improvement in depressive symptoms.
- Anxiety and Emotional Regulation: Through its effects on neurotransmitter synthesis and the stress response, folate supports emotional stability, stress resilience, and reduced anxiety.
- Cognitive Decline and Dementia: Low folate status and elevated homocysteine are both independently associated with accelerated cognitive decline, brain atrophy, and increased risk of Alzheimer's disease and vascular dementia. Supplementation with folate, B12, and B6 has been shown to slow brain atrophy in at-risk individuals.
- Schizophrenia: Low folate and impaired methylation have been implicated in schizophrenia, and methylfolate supplementation has shown benefit as an adjunctive treatment in some studies.
6. Red Blood Cell Formation and Megaloblastic Anemia
- Erythropoiesis: Red blood cells are among the most rapidly dividing cells in the body, with millions produced every second. Folate is essential for the DNA synthesis that drives this extraordinary rate of cell division.
- Megaloblastic Anemia: When folate is deficient, red blood cell precursors in the bone marrow cannot properly replicate their DNA. The cells continue to grow but cannot divide, producing abnormally large, immature, and dysfunctional red blood cells called megaloblasts. This results in megaloblastic (macrocytic) anemia — characterized by fatigue, weakness, pallor, shortness of breath, and cognitive impairment.
- Distinguishing from B12 Deficiency: Both folate and Vitamin B12 deficiency can cause megaloblastic anemia with identical blood cell morphology. Distinguishing between the two is critical because treating B12-deficiency anemia with folate alone can mask the anemia while allowing irreversible neurological damage from B12 deficiency to progress. Both nutrients should always be assessed together.
- White Blood Cell and Platelet Effects: Severe folate deficiency can also impair the production of white blood cells (leukopenia) and platelets (thrombocytopenia), compromising both immune defense and blood clotting ability.
- Neutrophil Hypersegmentation: One of the earliest and most sensitive laboratory signs of folate deficiency is the appearance of hypersegmented neutrophils on a blood smear — white blood cells with abnormally multilobed nuclei.
7. Cancer Prevention
Folate's role in DNA synthesis, repair, methylation, and genomic stability gives it significant relevance to cancer prevention.
- DNA Stability: Folate deficiency causes uracil misincorporation into DNA, chromosome breaks, and aberrant DNA methylation patterns — all of which increase the risk of carcinogenesis.
- Colorectal Cancer: The most extensively studied cancer-folate relationship. Consistently, higher folate status is associated with significantly reduced risk of colorectal cancer and colorectal adenomas (precancerous polyps). Folate deficiency is considered one of the most modifiable dietary risk factors for this cancer.
- Breast Cancer: Adequate folate intake may be protective against breast cancer, particularly in women who consume alcohol (which depletes folate and disrupts its metabolism). The protective effect appears strongest when folate comes from food sources.
- Cervical Cancer: Folate deficiency has been associated with increased susceptibility to persistent HPV infection and cervical dysplasia. Adequate folate supports DNA repair in cervical epithelial cells.
- Pancreatic, Esophageal, and Other Cancers: Emerging epidemiological evidence links adequate folate intake with reduced risk of several additional cancer types, though the evidence is less robust than for colorectal cancer.
- Important Nuance — Dual Role: While folate deficiency increases cancer initiation risk through DNA damage and aberrant methylation, some research suggests that high-dose folic acid supplementation (particularly synthetic folic acid) may accelerate the growth of pre-existing precancerous or cancerous cells by providing them with the DNA synthesis machinery they need to proliferate. This dual nature is one reason natural practitioners strongly prefer food-form folate and 5-MTHF over synthetic folic acid.
8. The MTHFR Gene — A Critical Genetic Consideration
Understanding the MTHFR gene is essential for any discussion of folate in natural medicine, as genetic variations in this gene profoundly affect how individuals process and utilize folate.
- The MTHFR Enzyme: Methylenetetrahydrofolate reductase (MTHFR) is the enzyme that converts 5,10-methylenetetrahydrofolate into 5-methyltetrahydrofolate (5-MTHF) — the biologically active form of folate that enters the methylation cycle. This is the rate-limiting step of folate activation.
- C677T Polymorphism: Approximately 10–15% of many populations are homozygous (TT) for the C677T variant, which reduces MTHFR enzyme activity by up to 70%. Another 40–50% are heterozygous (CT), with approximately 35% reduced activity. These individuals produce significantly less 5-MTHF from dietary folate and synthetic folic acid.
- A1298C Polymorphism: A second common variant that further reduces MTHFR function, particularly when combined with C677T (compound heterozygosity).
- Clinical Consequences: Individuals with reduced MTHFR function are at increased risk for elevated homocysteine, neural tube defects, cardiovascular disease, depression, recurrent pregnancy loss, blood clotting disorders, and various methylation-related conditions.
- Folic Acid vs. 5-MTHF: Individuals with MTHFR polymorphisms cannot efficiently convert synthetic folic acid into the active 5-MTHF form. Unmetabolized folic acid can accumulate in the blood, potentially blocking folate receptors and paradoxically worsening functional folate deficiency. For these individuals, supplementation with pre-formed 5-MTHF (L-methylfolate) bypasses the MTHFR enzyme entirely and is strongly preferred.
- Riboflavin Connection: FAD (from Vitamin B2) is the essential cofactor for the MTHFR enzyme. Individuals with MTHFR variants benefit significantly from concurrent riboflavin supplementation, which stabilizes the enzyme and partially restores its function.
- Prevalence Awareness: Given that up to 60% of some populations carry at least one MTHFR variant, natural practitioners increasingly recommend 5-MTHF as the default folate form for all patients, eliminating the risk of folic acid-related complications entirely.
9. Folate vs. Folic Acid — A Critical Distinction
This distinction is one of the most important topics in modern nutritional medicine, and natural practitioners are at the forefront of educating patients about it.
- Natural Folate: Refers to the various tetrahydrofolate forms found naturally in whole foods. These are reduced, bioactive forms that enter metabolic pathways directly after minimal processing in the intestinal wall.
- Folic Acid: A fully oxidized, synthetic compound that does not exist in nature. It was created for fortification and supplementation because of its superior stability and low cost. Folic acid must undergo a multi-step enzymatic conversion in the liver (via dihydrofolate reductase, DHFR) to become metabolically active — a process that is slow and easily saturated in humans.
- Unmetabolized Folic Acid (UMFA): When folic acid intake exceeds the liver's conversion capacity (which can happen at doses as low as 200 mcg in a single meal), unmetabolized folic acid accumulates in the bloodstream. UMFA has been associated with reduced NK cell activity, potential masking of B12 deficiency, and controversial associations with accelerated progression of pre-existing cancerous lesions.
- 5-MTHF (L-Methylfolate): The preferred supplemental form in natural medicine. It is the actual biologically active form of folate, requires no enzymatic conversion, bypasses the MTHFR enzyme entirely, does not produce unmetabolized folic acid, and enters the methylation cycle directly.
- Folinic Acid (5-Formyltetrahydrofolate): Another naturally occurring, biologically active folate form that can enter folate metabolism at multiple points without requiring MTHFR. It is sometimes preferred in certain clinical situations, particularly in individuals with specific genetic variants or those undergoing methotrexate "rescue" therapy.
- Food Fortification Concerns: In many countries, white flour, cereals, bread, pasta, and rice are fortified with synthetic folic acid by government mandate. While this policy has significantly reduced neural tube defect rates at the population level, it also means that many individuals are chronically exposed to folic acid that their bodies may not efficiently convert — a growing concern among natural medicine practitioners.
- Natural Practitioner Recommendation: Whenever possible, obtain folate from whole foods. When supplementation is needed, choose 5-MTHF (L-methylfolate) or folinic acid rather than synthetic folic acid.
10. Immune System Support
- Immune Cell Proliferation: Immune cells — particularly T-lymphocytes, B-lymphocytes, and neutrophils — undergo rapid clonal expansion during immune responses, requiring enormous quantities of DNA synthesis. Folate is essential for this proliferative burst.
- T-Cell Function: Folate deficiency impairs T-cell proliferation, differentiation, and cytokine production, weakening both cell-mediated and humoral immune responses.
- NK Cell Activity: Natural killer cell cytotoxicity — a frontline defense against virally infected and abnormal cells — is reduced in folate deficiency.
- Antibody Production: B-cell proliferation and immunoglobulin synthesis are folate-dependent processes. Deficiency reduces the body's ability to mount an effective antibody response to infection.
- Inflammatory Modulation: Folate influences the production of inflammatory cytokines and helps maintain the balance between pro-inflammatory and anti-inflammatory signaling.
- Elderly Immune Function: Age-related decline in immune competence is strongly correlated with declining folate status. Supplementation in older adults supports improved immune markers.
11. Liver Health and Detoxification
- Phosphatidylcholine Synthesis: Folate-dependent methylation is required for the synthesis of phosphatidylcholine from phosphatidylethanolamine via the PEMT pathway. Phosphatidylcholine is essential for VLDL assembly and hepatic fat export. Folate deficiency impairs this process, contributing to fatty liver (hepatic steatosis).
- Non-Alcoholic Fatty Liver Disease (NAFLD): Impaired methylation from low folate status is increasingly recognized as a contributing factor in the development and progression of NAFLD — one of the most prevalent liver conditions worldwide.
- Glutathione Support: Through the transsulfuration pathway (which depends on the methylation cycle that folate drives), folate indirectly supports the production of cysteine and glutathione — the liver's primary antioxidant and Phase II detoxification molecule.
- Estrogen and Histamine Clearance: Methylation-dependent enzymes (COMT for estrogen, HNMT for histamine) require SAMe produced through the folate-driven methylation cycle. Poor folate status impairs the clearance of these compounds, contributing to estrogen dominance and histamine intolerance.
- Alcohol and Folate: Alcohol directly impairs folate absorption, accelerates its degradation, increases urinary excretion, and inhibits methionine synthase. Chronic alcohol use is one of the most common causes of severe folate deficiency and its downstream consequences including fatty liver, elevated homocysteine, and increased cancer risk.
12. Gut Health
- Intestinal Epithelial Renewal: The intestinal lining is one of the most rapidly renewing tissues in the body, with the entire epithelial surface replaced every 3–5 days. This extraordinary rate of cell division is entirely dependent on folate for DNA synthesis.
- Gut Barrier Integrity: Folate deficiency impairs the replacement of damaged intestinal epithelial cells, compromising gut barrier function and increasing susceptibility to "leaky gut," food sensitivities, and systemic inflammation.
- Folate Absorption: Dietary folate is absorbed primarily in the jejunum of the small intestine via the proton-coupled folate transporter (PCFT). Conditions that damage the intestinal lining — celiac disease, Crohn's disease, tropical sprue — significantly impair folate absorption, creating a vicious cycle of deficiency and gut damage.
- Microbiome Interactions: Certain gut bacteria synthesize folate, while others consume it. The composition of the gut microbiome influences overall folate availability, and folate status in turn influences microbial diversity.
13. Bone Health
- Homocysteine and Bone: Elevated homocysteine interferes with collagen cross-linking in bone tissue, reducing bone strength and increasing fracture risk independent of bone mineral density. Folate's homocysteine-lowering effect therefore directly supports bone structural integrity.
- Osteoblast Function: Emerging evidence suggests that folate and methylation status influence osteoblast (bone-building cell) activity and differentiation.
- Osteoporosis Risk: Epidemiological studies have associated low folate status and elevated homocysteine with increased risk of osteoporotic fractures, particularly in the elderly.
14. Natural Food Sources
True to its name derived from "leaf," folate is most abundant in dark leafy greens and other plant foods. Animal liver is also an exceptionally rich source.
Richest Whole Food Sources
- Beef Liver and Chicken Liver: The single most concentrated natural source of folate, providing several times the daily requirement per serving
- Dark Leafy Greens: Spinach, kale, collard greens, turnip greens, mustard greens, and romaine lettuce — the archetypal folate foods
- Lentils: One of the richest legume sources, providing approximately 90% of the daily value per cooked cup
- Black Beans, Chickpeas, and Kidney Beans: Excellent legume sources of folate along with fiber and plant protein
- Asparagus: One of the richest vegetable sources of folate — four spears provide roughly 25% of the daily value
- Broccoli and Brussels Sprouts: Cruciferous vegetables that provide folate alongside sulforaphane and other protective compounds
- Avocados: A rich source of folate with healthy monounsaturated fats that enhance absorption of fat-soluble nutrients
- Beets: Provide folate along with betaine (trimethylglycine), which serves as an alternative methyl donor in the methylation cycle
- Citrus Fruits (oranges, lemons, grapefruits): Good fruit sources of folate along with Vitamin C
- Eggs (pasture-raised): Provide folate in a bioavailable, food-matrix context
- Sunflower Seeds and Flaxseeds: Nutrient-dense seeds with meaningful folate content
- Nutritional Yeast: A plant-based B-vitamin powerhouse, especially valued in vegan diets
Important Notes on Folate Preservation
- Heat Sensitivity: Folate is one of the most heat-sensitive vitamins. Cooking can destroy 50–90% of the folate in foods, depending on the method and duration. Steaming and light sautéing preserve significantly more folate than boiling or prolonged cooking.
- Water Solubility: Folate leaches readily into cooking water. If boiling vegetables, use the cooking liquid in soups or sauces to recapture lost folate.
- Light and Air Exposure: Folate degrades upon prolonged exposure to light and air. Store leafy greens and folate-rich produce in dark, cool conditions and consume promptly after preparation.
- Raw Consumption: Incorporating raw leafy greens (in salads, smoothies, and juices) is one of the best ways to maximize folate intake from food sources.
15. Recommended Daily Intake
Folate intake is measured in Dietary Folate Equivalents (DFE) to account for the higher bioavailability of synthetic folic acid compared to food folate. 1 mcg DFE = 1 mcg food folate = 0.6 mcg folic acid from supplements or fortified food taken with food = 0.5 mcg folic acid taken on an empty stomach.
- Adult Men and Women: 400 mcg DFE per day
- Pregnant Women: 600 mcg DFE per day (many practitioners recommend 800–1,000 mcg of 5-MTHF)
- Breastfeeding Women: 500 mcg DFE per day
- Women of Childbearing Age: At minimum 400 mcg DFE daily, ideally from food and 5-MTHF supplementation, maintained continuously as a neural tube defect prevention measure
- Children (4–8 years): 200 mcg DFE per day
- Children (9–13 years): 300 mcg DFE per day
Therapeutic Doses: In natural medicine practice, therapeutic doses of 5-MTHF commonly range from 400 mcg to 15 mg daily depending on the clinical indication. For depression (adjunctive therapy), 7.5–15 mg of L-methylfolate is commonly used. For MTHFR support and homocysteine reduction, 1–5 mg of 5-MTHF is typical. The Tolerable Upper Intake Level (UL) of 1,000 mcg applies specifically to synthetic folic acid due to concerns about masking B12 deficiency; this limit does not apply to food folate or 5-MTHF.
16. Supplemental Forms
- L-5-Methyltetrahydrofolate (5-MTHF / L-Methylfolate): The biologically active, coenzymated form of folate. It bypasses all enzymatic conversion steps (including MTHFR), enters the methylation cycle directly, does not produce unmetabolized folic acid, and is effective regardless of MTHFR genotype. This is the gold standard recommendation in natural medicine. Common branded forms include Metafolin® (calcium L-methylfolate) and Quatrefolic® (glucosamine salt of 5-MTHF).
- Folinic Acid (5-Formyltetrahydrofolate / Leucovorin): A naturally occurring, reduced folate form that enters the folate cycle without requiring MTHFR. Used clinically in methotrexate rescue therapy and sometimes preferred in cerebral folate deficiency and certain autism spectrum protocols. It supports both methylation and DNA synthesis pathways.
- Folic Acid (Pteroylglutamic Acid): The synthetic, oxidized form used in food fortification and most inexpensive supplements. Requires hepatic conversion via DHFR and then MTHFR to become active. Natural practitioners generally recommend avoiding this form due to UMFA accumulation risks and MTHFR compatibility concerns.
- Whole Food Folate: Some supplements provide folate derived from food concentrates (such as lemon peel extract). While closer to food-form folate, the actual dose and bioavailability may vary.
17. Synergistic Nutrients
Folate is deeply embedded in a web of nutrient interdependencies:
- Vitamin B12 (Cobalamin): The most critical synergistic partner. B12 is required by methionine synthase to accept the methyl group from 5-MTHF. Without B12, folate becomes "trapped" as 5-MTHF and cannot re-enter the folate cycle — a phenomenon known as the "methyl trap" that functionally creates folate deficiency even when folate intake is adequate.
- Vitamin B2 (Riboflavin): FAD (from riboflavin) is the cofactor for the MTHFR enzyme. Adequate B2 stabilizes MTHFR function and is especially important for individuals with MTHFR polymorphisms.
- Vitamin B6 (Pyridoxine): B6 is essential for the transsulfuration pathway that clears homocysteine via conversion to cysteine. B6, folate, and B12 form the essential homocysteine-management triad.
- Betaine (Trimethylglycine, TMG): An alternative methyl donor that can convert homocysteine to methionine via the BHMT enzyme, providing a backup pathway when the folate-dependent route is insufficient.
- Choline: Choline is both a methyl donor (via betaine) and a product of methylation (phosphatidylcholine). Choline and folate metabolism are deeply intertwined, and deficiency in one increases the requirement for the other.
- Zinc: Required for the function of several enzymes in folate metabolism, including folylpolyglutamate synthetase, which retains folate within cells.
- Vitamin C: May help stabilize and preserve folate in food and in the body, protecting it from oxidative degradation.
- Iron: Folate and iron deficiency often coexist and share symptoms (anemia, fatigue). Both should be assessed and addressed together.
18. Populations at Higher Risk of Deficiency
- Women of Childbearing Age: The most critical at-risk group due to the extreme sensitivity of neural tube development to folate status in the earliest weeks of pregnancy.
- Pregnant and Breastfeeding Women: Dramatically increased demands for DNA synthesis, cell division, and methylation raise folate requirements substantially.
- Individuals with MTHFR Polymorphisms: Up to 60% of some populations carry variants that reduce the ability to produce active 5-MTHF from dietary folate and folic acid.
- Individuals with Alcohol Use Disorders: Alcohol impairs folate absorption, accelerates its degradation, increases urinary loss, and inhibits methionine synthase — making alcoholism one of the most common causes of severe folate deficiency.
- Individuals with Malabsorptive Conditions: Celiac disease, Crohn's disease, tropical sprue, short bowel syndrome, and gastric bypass surgery all impair folate absorption from the jejunum.
- Elderly Individuals: Reduced dietary intake, impaired absorption, medication interactions, and increased inflammation all contribute to elevated deficiency risk.
- Individuals on Methotrexate: This drug (used for rheumatoid arthritis, psoriasis, and cancer) is a folate antagonist that directly inhibits dihydrofolate reductase. Folinic acid supplementation is standard practice during methotrexate therapy.
- Individuals on Anticonvulsants: Phenytoin, carbamazepine, and valproate interfere with folate metabolism and increase deficiency risk.
- Individuals on Oral Contraceptives: Hormonal birth control has been associated with reduced folate status, with potential implications for women who conceive shortly after discontinuation.
- Individuals with Inflammatory Conditions: Chronic inflammation increases folate consumption and accelerates turnover.
- Smokers: Smoking depletes folate and impairs methylation capacity.
19. Signs of Deficiency
Folate deficiency can be subtle at first but eventually affects nearly every system — causing megaloblastic anemia (fatigue, weakness, pallor), a sore red tongue and mouth ulcers, depression and brain fog, elevated homocysteine, and, in early pregnancy, neural tube defects. Excess is a different concern: high doses of synthetic folic acid can leave unmetabolized folic acid in the blood and may mask the anemia of an underlying B12 deficiency while nerve damage progresses. For a full, patient-friendly guide to the symptoms, causes, and treatment of each, see Folate Deficiency and Folate / Folic Acid Excess.
20. Special Therapeutic Applications
- Depression (Adjunctive Therapy): L-methylfolate at 7.5–15 mg daily alongside antidepressants or as part of a comprehensive natural mood-support protocol. Particularly effective in individuals with MTHFR variants or low baseline folate.
- Preconception and Prenatal Care: 800–1,000 mcg of 5-MTHF daily beginning at least 3 months before conception and continuing throughout pregnancy, combined with a comprehensive prenatal formula.
- Cardiovascular Protection: 1–5 mg of 5-MTHF daily in combination with B12 and B6 for homocysteine reduction and vascular protection.
- MTHFR Support Protocols: 1–5 mg of 5-MTHF daily combined with riboflavin (B2), methylcobalamin (B12), P5P (B6), betaine (TMG), and choline for comprehensive methylation support.
- Cognitive Decline Prevention: Folate, B12, and B6 combination therapy for slowing brain atrophy and cognitive decline in at-risk elderly individuals.
- Methotrexate Rescue: Folinic acid (leucovorin) to counteract the folate-depleting effects of methotrexate therapy while maintaining therapeutic efficacy.
- Fertility Support: Folate optimization in both women and men as part of preconception care, supporting egg quality, sperm health, and healthy implantation.
- Histamine Intolerance: Methylation support with 5-MTHF, B12, and B6 to enhance histamine clearance via HNMT.
- Estrogen Dominance: Methylation optimization to support COMT-mediated estrogen clearance, reducing symptoms of estrogen excess.
Final Thoughts
Vitamin B9 is nothing less than the vitamin of life itself — the nutrient upon which DNA replication, cellular division, methylation, fetal development, neurotransmitter synthesis, cardiovascular protection, and cancer prevention all fundamentally depend. In natural medicine, the folate conversation has evolved far beyond simply "take your folic acid." Today, we understand the critical importance of form (5-MTHF over synthetic folic acid), genetics (MTHFR polymorphisms), and synergy (B12, B2, B6, choline, betaine) in ensuring that folate fulfills its extraordinary potential. Whether you are supporting a woman through pregnancy, addressing depression, protecting the cardiovascular system, optimizing methylation, or simply striving to maintain the integrity of your DNA with every cell division, folate deserves a place at the very center of your nutritional strategy.
From the first fold of the neural tube to the last methyl group donated in a lifetime, folate writes the story of life in the language of DNA — nourish it well, and the story will be one of health, resilience, and vitality.
Connections
- The Methylation Cycle & Homocysteine — interactive animation
- Folate Deficiency
- Folate / Folic Acid Excess
- Anemia
- Depression
- Homocysteine
- Cancer
- Vitamin B12
- Vitamin B6
- Folate and Mental Health
- Folate and Pregnancy
- Anxiety
- Methionine
- Choline
- Vitamin C
- Iron
- B12 Deficiency Diagnosis
- Alzheimer's Disease
- Dementia
- Lentils
- Broccoli