Folate for Methylation & Homocysteine
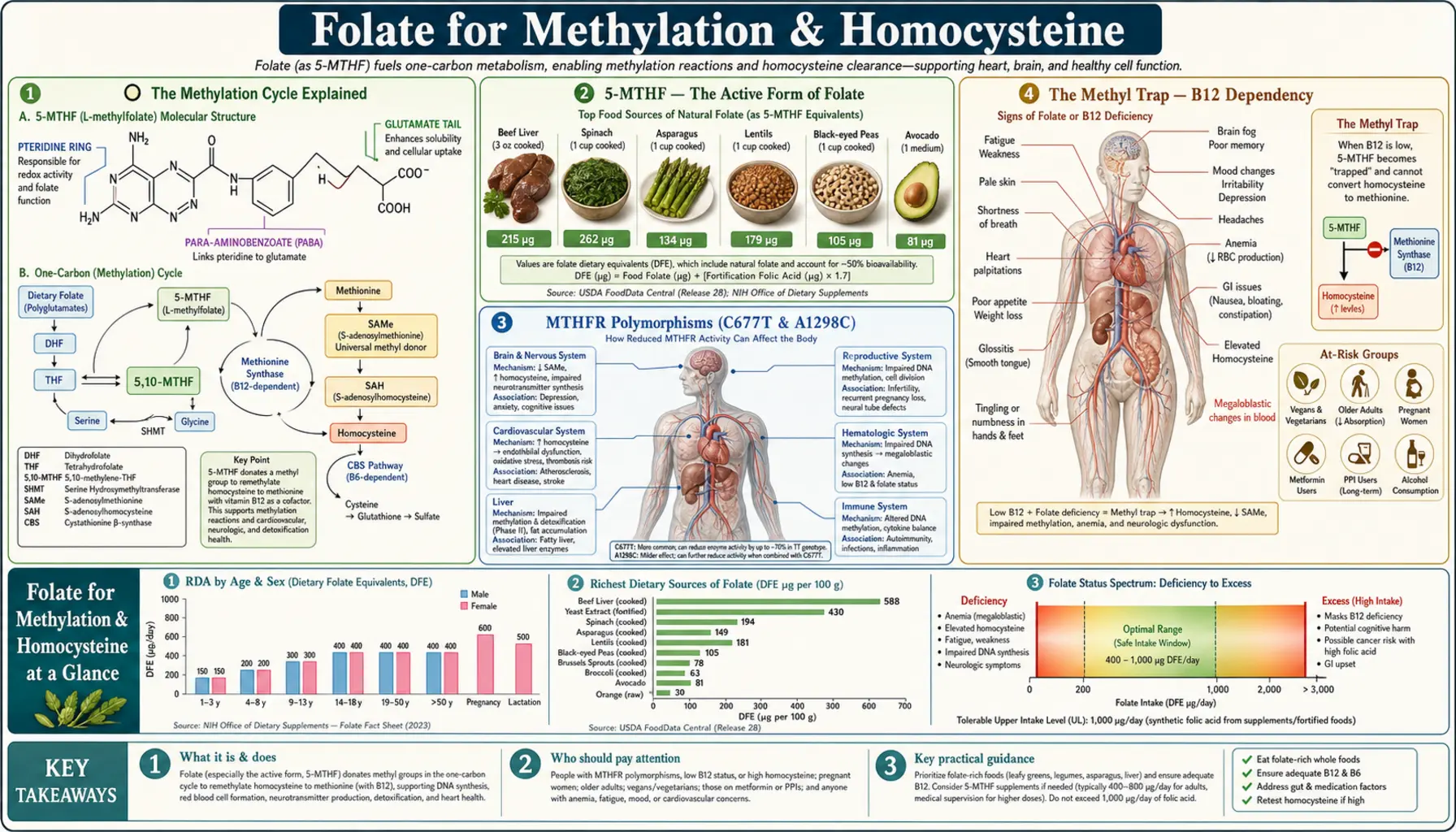
Folate's most consequential biochemical role is delivering the methyl group that converts homocysteine to methionine, regenerating S-adenosylmethionine (SAMe) — the body's universal methyl donor for over 200 substrates including DNA, RNA, neurotransmitters, phospholipids, and hormones. This single reaction sits at the rate-limiting step of the entire methylation cycle. The enzyme that produces active folate (MTHFR) is unusually polymorphic in humans: 40% heterozygous, 10-12% homozygous for variants that cut enzyme activity 30-70%. These variants explain why so many people see dramatic clinical responses to switching from synthetic folic acid to methylated folate (5-MTHF / Quatrefolic / Metafolin) — the active form that bypasses MTHFR entirely. This deep-dive walks through the methylation cycle biochemistry, the MTHFR polymorphisms, the methyl-trap concept that links folate to B12, the unmetabolized folic acid concern, and the cognitive/cardiovascular trial evidence that emerged from this framework.
Table of Contents
- The Methylation Cycle Explained
- 5-MTHF — The Active Form of Folate
- MTHFR Polymorphisms (C677T & A1298C)
- The Methyl Trap — B12 Dependency
- Methylfolate vs Synthetic Folic Acid
- The Unmetabolized Folic Acid (UMFA) Concern
- DHFR Saturation & the 200 mcg Threshold
- Supplement Forms: Quatrefolic, Metafolin, Folinic
- The VITACOG Cognitive Trial
- Testing Folate, Homocysteine, MTHFR
- Cautions
- Key Research Papers
- Connections
- Featured Videos
The Methylation Cycle Explained
Methylation is the chemical process of adding a CH3 (methyl) group to a substrate. In biochemistry it is one of the most ubiquitous reactions in human metabolism — methylation activates or inactivates genes, builds and breaks down neurotransmitters, processes hormones, assembles cell membranes, and produces creatine. Every methylation reaction in the body draws its methyl group from a central pool called the methylation cycle, and folate is the rate-limiting input to that pool.
The cycle, simplified:
- Dietary folate or supplemental folate → reduced and methylated through several intermediate steps → 5-methyltetrahydrofolate (5-MTHF). The rate-limiting step is methylenetetrahydrofolate reductase (MTHFR).
- 5-MTHF donates its methyl group to homocysteine, regenerating methionine. This reaction is catalyzed by methionine synthase (gene MTR), with vitamin B12 (methylcobalamin) as an essential cofactor.
- Methionine is converted to S-adenosylmethionine (SAMe) — the universal methyl donor.
- SAMe donates its methyl group to one of more than 200 different substrate molecules (DNA, RNA, neurotransmitters, phospholipids, creatine, histamine, estrogens), becoming S-adenosylhomocysteine (SAH).
- SAH is hydrolyzed back to homocysteine, completing the cycle.
From homocysteine, three things can happen: (a) remethylation back to methionine via the folate-B12 pathway just described, (b) remethylation via an alternative betaine-homocysteine methyltransferase (BHMT) pathway using betaine/TMG and choline as methyl sources (primarily in liver), or (c) clearance via the transsulfuration pathway through cystathionine to cysteine and ultimately glutathione — a B6-dependent reaction.
The clinical significance: any disruption in folate availability, B12 status, or MTHFR function impairs methyl group production. Downstream consequences include elevated homocysteine, reduced neurotransmitter synthesis, aberrant DNA methylation, reduced phosphatidylcholine production (fatty liver), and accumulated histamine and estrogen metabolites. Folate is therefore not a peripheral vitamin — it is the rate-limiting input to a pathway that touches nearly every cellular process in the body.
5-MTHF — The Active Form of Folate
Folate exists in many interconvertible forms, but only one form — 5-methyltetrahydrofolate (5-MTHF, also called L-methylfolate or levomefolic acid) — can directly donate its methyl group to homocysteine via methionine synthase.
The folate "family":
- Folate (food folate): a mix of polyglutamate forms found naturally in spinach, kale, liver, lentils, and other folate-rich foods. Must be hydrolyzed to monoglutamates by intestinal conjugase, then absorbed primarily as monoglutamate 5-MTHF.
- Folic acid (pteroylmonoglutamic acid): the fully oxidized synthetic form — does not exist in nature. Used in fortification, multivitamins, and prescription B-complex products because of stability and cost. Must be reduced to dihydrofolate by DHFR, reduced again to tetrahydrofolate by DHFR, methylated to 5,10-methylene-THF, then methylated to 5-MTHF by MTHFR.
- Dihydrofolate (DHF): first reduction product. Not biologically active.
- Tetrahydrofolate (THF): the central one-carbon carrier. Can shuttle carbon units between different intermediates for DNA synthesis (thymidylate, purines) or for methylation.
- 5,10-methylene-tetrahydrofolate (5,10-methylene-THF): the donor for thymidylate synthesis — needed for DNA synthesis. Also the substrate for MTHFR.
- 5-formyltetrahydrofolate (folinic acid, leucovorin): a stable storage form. Can enter the folate cycle at multiple points without requiring MTHFR. Used clinically as methotrexate rescue and in cerebral folate deficiency.
- 10-formyltetrahydrofolate: the donor for two steps of purine synthesis.
- 5-MTHF: the active methylation-cycle form. The terminal point of dietary/supplemental folate processing and the form that enters the bloodstream from the intestine and crosses the blood-brain barrier.
The key point: every other form must ultimately be converted to 5-MTHF for the methylation-cycle benefit. The conversion is multi-step, requires DHFR and MTHFR, and is rate-limited by genetic polymorphisms in both enzymes (especially MTHFR). Supplementing 5-MTHF directly bypasses all of these steps.
MTHFR Polymorphisms (C677T & A1298C)
The MTHFR gene is one of the most polymorphic enzyme-coding genes in the human genome. Two single-nucleotide polymorphisms (SNPs) are clinically significant:
C677T (rs1801133)
- A cytosine-to-thymine substitution at position 677, causing an alanine-to-valine amino acid substitution in the enzyme
- The resulting enzyme is thermolabile — less stable, especially at body temperature
- Heterozygous (CT) carriers: ~40% of many populations (higher in Hispanic and Mediterranean populations, lower in African). Approximately 30% reduced MTHFR enzyme activity.
- Homozygous (TT) carriers: ~10-12% of populations (up to 25% in Mexican/Hispanic populations). Approximately 70% reduced enzyme activity.
- Clinical associations: mildly elevated fasting homocysteine, increased risk of neural tube defects, recurrent pregnancy loss, venous thromboembolism (in some populations), and possibly cardiovascular and cerebrovascular events (effect attenuated by folate fortification)
A1298C (rs1801131)
- An adenine-to-cytosine substitution at position 1298, causing a glutamate-to-alanine substitution
- Heterozygous (AC): ~40% of populations. Modest reduction in enzyme activity.
- Homozygous (CC): ~10% of populations. More substantial reduction.
- Less clinical impact in isolation than C677T but significant in compound heterozygosity
Compound heterozygosity (C677T + A1298C)
- ~15-20% of populations carry one copy of each variant
- Enzyme activity reduced 50-70% — clinically similar to homozygous TT
- Highest combined risk for the clinical associations above
Riboflavin stabilization
FAD (derived from riboflavin / vitamin B2) is the essential prosthetic group for MTHFR. Variant MTHFR enzymes lose their FAD cofactor more readily than wild-type enzymes. Supplemental riboflavin (B2) significantly stabilizes variant MTHFR and partially restores its function. In hypertensive C677T-TT carriers, riboflavin supplementation alone has been shown to lower blood pressure by 5-10 mmHg (Wilson 2012, McNulty research group at Ulster University).
Practical implication: MTHFR-variant carriers benefit from both methylfolate supplementation (to bypass the enzyme) and riboflavin supplementation (to stabilize what enzyme function remains). Methylated B-complex products typically include both.
The Methyl Trap — B12 Dependency
The "methyl trap" is a critical biochemical phenomenon that links folate and vitamin B12 inseparably. Understanding it is essential to appreciating why these two nutrients must always be assessed and supplemented together.
The mechanism:
- MTHFR converts 5,10-methylene-THF to 5-MTHF in an irreversible reaction. Once folate enters the 5-MTHF form, it cannot go back to other folate forms.
- To re-enter the folate cycle and provide one-carbon units for other functions (DNA synthesis, purine synthesis), 5-MTHF must donate its methyl group to homocysteine via methionine synthase, becoming tetrahydrofolate (THF).
- Methionine synthase absolutely requires B12 (methylcobalamin) as a cofactor.
- If B12 is deficient, methionine synthase cannot function. 5-MTHF accumulates and becomes "trapped" — unable to donate its methyl group, unable to return to THF.
- The cell experiences functional folate deficiency for DNA synthesis even when folate intake is adequate. Megaloblastic anemia develops — the same morphology as primary folate deficiency.
The clinical consequences:
- B12 deficiency causes folate-style megaloblastic anemia even with normal folate intake
- Supplementing folate corrects the anemia by providing enough total folate that some escapes the methyl trap and supports DNA synthesis — but does not correct the underlying B12 deficiency
- The neurological consequences of B12 deficiency (subacute combined degeneration of the spinal cord, peripheral neuropathy, cognitive decline) continue to progress under the cover of corrected anemia — potentially irreversibly
- This is the historical reason for the 1,000 mcg/day upper intake level on synthetic folic acid — the FDA was concerned about masking unrecognized B12 deficiency in the elderly
The takeaways:
- Never supplement high-dose folate without assessing B12 status — serum B12 below 400 pg/mL warrants methylmalonic acid (MMA) and homocysteine testing for functional B12 deficiency
- Always co-supplement methylcobalamin (B12) with high-dose methylfolate — typically 1,000 mcg methylcobalamin alongside 1-5 mg methylfolate
- The elderly, vegans, and patients on metformin or PPIs are at highest risk of unrecognized B12 deficiency and should be screened before high-dose folate
Methylfolate vs Synthetic Folic Acid
Practical comparison of the two main supplement forms:
| Aspect | Synthetic Folic Acid | 5-MTHF (Methylfolate) |
|---|---|---|
| Natural occurrence | None — does not exist in nature | The actual form found in blood after eating food folate |
| Activation steps | DHFR × 2 reductions → methylation → MTHFR | None — already active |
| Affected by MTHFR variants? | Yes — reduced conversion in 50% of population | No — bypasses MTHFR entirely |
| Produces UMFA? | Yes — above 200 mcg per dose | No |
| DHFR saturation limit | ~200-400 mcg per single dose | N/A — no DHFR conversion needed |
| Cost | Very inexpensive ($5-10/year) | Higher ($15-40/month at therapeutic doses) |
| NTD prevention evidence | Strong (original trials used this form) | Indirect — same downstream molecule |
| Depression adjunct evidence | Weak (Coppen 2000 fluoxetine adjunct) | Strong (Papakostas 2012 SSRI adjunct) |
| FDA medical food status | No | Yes (Deplin for depression) |
| Best for | Low-cost universal prophylaxis; historical RCT-validated NTD prevention | MTHFR variants; high-dose therapy; depression; methylation-dependent conditions |
The integrative medicine consensus has shifted toward defaulting to methylfolate (5-MTHF) for most therapeutic supplementation, with synthetic folic acid reserved for low-dose population-level fortification and women in low-resource settings without access to the more expensive methylated form.
The Unmetabolized Folic Acid (UMFA) Concern
When synthetic folic acid intake exceeds the liver's DHFR conversion capacity, unmetabolized folic acid (UMFA) appears in serum. In US adults consuming fortified grain products plus standard multivitamins, UMFA is detectable in essentially everyone — reflecting a chronic intake above the DHFR saturation threshold.
UMFA-associated concerns documented in the literature:
- Reduced NK cell cytotoxicity — Troen et al. 2006 found postmenopausal women with detectable UMFA had lower natural killer cell cytotoxic activity, an important component of immune surveillance against virally infected and abnormal cells
- Potential B12 deficiency masking — the historical concern that led to the 1,000 mcg/day folic acid upper limit. High folate intake corrects the megaloblastic anemia of B12 deficiency without correcting the underlying B12 deficiency, allowing neurological damage to progress unchecked
- Theoretical promotion of preexisting precancerous lesions — the "dual effect" hypothesis. Folate deficiency causes DNA damage that initiates carcinogenesis, but high folate provides DNA synthesis substrates that may accelerate growth of already-neoplastic cells. The colorectal adenoma evidence is mixed but the concern persists in chronic high-dose users
- Folate receptor binding — UMFA binds folate receptors with high affinity but may not deliver the same biological effect as 5-MTHF, potentially producing a partial receptor-blocking effect
- Possible autism risk at extreme intake — some studies (Raghavan 2018, others) found U-shaped autism risk curves with elevated risk at the highest maternal folate levels at delivery, potentially reflecting UMFA accumulation rather than true folate excess
The UMFA concern is the strongest single argument for preferring 5-MTHF over synthetic folic acid — methylfolate does not produce UMFA at any reasonable supplementation dose because it does not require DHFR conversion.
DHFR Saturation & the 200 mcg Threshold
Human dihydrofolate reductase (DHFR) is unusually slow compared to other mammals. The enzyme reaches saturation at approximately 200-400 mcg of synthetic folic acid per single dose. Above this, unconverted folic acid spills into the bloodstream as UMFA.
Practical implications:
- A standard prenatal vitamin with 800 mcg folic acid in a single capsule exceeds DHFR capacity by 2-4×
- A loading dose of 4 mg folic acid (recommended for prior-NTD-pregnancy women) exceeds capacity by 10-20×
- A typical "B-complex 100" with 400 mcg folic acid is near the saturation threshold
- Combined with fortified grain consumption (estimated 100-200 mcg additional folic acid per day in the average US diet), most supplement users chronically generate UMFA
The methylfolate workaround: 5-MTHF does not require DHFR conversion. A 5 mg dose of 5-MTHF generates no UMFA because there is no synthetic folic acid in the system. This is why high-dose folate therapy for depression (7.5-15 mg methylfolate daily) is feasible only with the methylated form — equivalent doses of synthetic folic acid would produce dramatic UMFA accumulation.
Supplement Forms: Quatrefolic, Metafolin, Folinic
Quatrefolic ((6S)-5-methyltetrahydrofolic acid, glucosamine salt)
A patented form of 5-MTHF combined with a glucosamine salt for stability and bioavailability. Manufactured by Gnosis (now Lesaffre). Excellent water solubility, high stability, no chirality concerns (only the bioactive 6S isomer). Found in many integrative-medicine-oriented brands including Designs for Health, Pure Encapsulations, Seeking Health, Thorne.
Metafolin (L-5-methyltetrahydrofolate, calcium salt)
A patented calcium salt form of 5-MTHF manufactured by Merck KGaA (Germany). The oldest and most extensively studied methylfolate brand — nearly all pharmaceutical research uses Metafolin. Less water-soluble than Quatrefolic but well-validated. Found in Thorne, Pure Encapsulations, and many other brands.
L-methylfolate (Deplin)
Pharmaceutical-grade L-methylfolate available in 7.5 mg and 15 mg capsules. FDA-classified as a medical food for adjunctive treatment of major depressive disorder and schizophrenia. Manufactured by Alfasigma. Prescription-required in the US.
Folinic acid (5-formyltetrahydrofolate, leucovorin)
A reduced folate form that enters folate metabolism at a different point — can be converted to 5-MTHF but also to other folate forms needed for DNA synthesis without requiring MTHFR. Used clinically:
- Methotrexate rescue — folinic acid is given after high-dose methotrexate chemotherapy to "rescue" non-cancer cells while methotrexate continues to act on cancer cells
- Cerebral folate deficiency — the only folate form that crosses the blood-brain barrier via an alternative receptor when folate-receptor autoantibodies are present
- Some autism spectrum protocols — based on the cerebral folate deficiency hypothesis
- Methylation-cycle "over-methylators" who experience side effects from methylfolate (anxiety, agitation) may tolerate folinic acid better
Available as calcium folinate or as leucovorin (the calcium salt). Doses typically 800 mcg to 25 mg depending on indication.
Forms to avoid
- Synthetic folic acid at therapeutic doses (1 mg+) chronically
- "Folate" labels with no specification — if a label says "folate" without specifying 5-MTHF / Quatrefolic / Metafolin / folinic acid, it is usually synthetic folic acid in disguise
The VITACOG Cognitive Trial
The VITACOG trial (Smith et al., PLoS ONE 2010; de Jager et al., Int J Geriatr Psychiatry 2012) is the most cited B-vitamin cognitive trial. 271 elderly subjects (over 70) with mild cognitive impairment and elevated homocysteine were randomized to a B-vitamin combination (800 mcg folic acid + 500 mcg cyanocobalamin B12 + 20 mg pyridoxine B6) versus placebo for 2 years. The primary outcome was rate of brain atrophy measured by serial MRI.
Results:
- Mean rate of brain atrophy reduced by 30% in the B-vitamin group versus placebo
- Effect concentrated in the subgroup with baseline elevated homocysteine (above ~11 μmol/L)
- Subsequent analysis showed atrophy reduction specifically in cognitively important brain regions (medial temporal lobe, hippocampus)
- Cognitive outcomes (episodic memory) improved in subjects with the highest baseline homocysteine
- The protective effect of B vitamins was conditional on adequate omega-3 status (Jerneren et al. 2015) — B vitamins worked in subjects with adequate DHA but not in subjects with low omega-3
VITACOG established that homocysteine-lowering through folate, B12, and B6 supplementation can slow the brain atrophy associated with mild cognitive impairment and early Alzheimer's — particularly in subjects with elevated baseline homocysteine and adequate omega-3 intake. The implication for clinical practice: testing homocysteine and intervening with methylfolate + methylcobalamin + B6 + DHA in patients with elevated levels is a defensible cognitive-protection strategy supported by RCT evidence.
Testing Folate, Homocysteine, MTHFR
Serum folate
Reflects recent intake (days-weeks). Optimal range varies by laboratory; typical reference is >5 ng/mL with most integrative practitioners targeting >10 ng/mL. Limited utility because of short half-life.
Red blood cell folate
Reflects tissue folate stores over the lifespan of the red blood cell (~120 days). The preferred measure for assessing true folate status. Optimal range: >400 ng/mL (some practitioners target >600 ng/mL). For pregnancy prevention of NTDs, the WHO recommends RBC folate >906 nmol/L (>400 ng/mL) as the threshold for protective status.
Homocysteine
The integrated functional marker of folate, B12, and B6 status — if any of the three is insufficient, homocysteine rises. Optimal: <7 μmol/L. Elevated: >10 μmol/L. Most laboratories report <15 μmol/L as "normal" but functional medicine targets are tighter. See the Homocysteine lab test page for full details on interpretation.
Methylmalonic acid (MMA)
A functional marker specific for B12 deficiency. Elevated MMA indicates B12 deficiency at the cellular level even when serum B12 is normal-low. Useful for distinguishing folate deficiency (normal MMA, elevated homocysteine) from B12 deficiency (elevated MMA and elevated homocysteine).
MTHFR genotyping
Tests for the C677T and A1298C variants. Available through 23andMe, Ancestry, commercial laboratories, and most physician-ordered genetic panels. Not strictly necessary in clinical practice because the conservative response is to default to methylfolate regardless of genotype — but useful for risk stratification and patient education about the underlying biology. The genotype is fixed at conception and cannot change — one test in a lifetime is sufficient.
Cautions
- B12 deficiency masking — the methyl trap concern. Always assess and correct B12 status before high-dose folate. Co-supplement methylcobalamin (1,000 mcg daily) with any high-dose methylfolate regimen.
- Methylation overdrive ("methyl overload") — some patients experience anxiety, agitation, irritability, or insomnia when starting high-dose methylfolate — particularly those with COMT polymorphisms (slow COMT enzyme reduces catecholamine clearance). Start with lower doses (400-800 mcg), titrate slowly, and consider folinic acid as an alternative for patients who tolerate methylfolate poorly. Niacin (500 mg) can rescue acute methyl overload by acting as a methyl sink via the NNMT enzyme.
- Methotrexate interaction — methotrexate is a DHFR inhibitor used for rheumatoid arthritis, psoriasis, and chemotherapy. Standard folate supplementation co-administered with methotrexate is standard care for rheumatoid arthritis (reduces side effects, preserves efficacy). For cancer chemotherapy methotrexate, only folinic acid (leucovorin) rescue is appropriate — not folic acid — and timing is critical (consult oncology team).
- Anticonvulsant interactions — phenytoin, carbamazepine, valproate, and primidone reduce folate status and elevate homocysteine. Higher folate doses are needed during anticonvulsant therapy, but coordinate with the prescribing neurologist because folate can affect anticonvulsant blood levels.
- Cerebral folate deficiency — in patients with folate-receptor autoantibodies, serum folate may be normal but CSF folate is low. Requires folinic acid (not methylfolate) for crossing the blood-brain barrier via the alternative receptor.
- Pregnancy — high-dose folate is generally safe in pregnancy but should be coordinated with prenatal care. Avoid synthetic folic acid above 1 mg/day in pregnancy if alternatives are available; choose methylfolate.
- Cancer history — patients with current or recently treated colorectal adenomas, hormone-sensitive cancers, or other folate-responsive malignancies should discuss high-dose folate with their oncologist due to the "dual effect" hypothesis. Standard intakes are not in the concern range; therapeutic high doses (5-15 mg) warrant individualized discussion.
Key Research Papers
- Frosst P et al. (1995). A candidate genetic risk factor for vascular disease: a common mutation in methylenetetrahydrofolate reductase. Nat Genet. — PubMed
- Smith AD et al. (2010). Homocysteine-lowering by B vitamins slows the rate of accelerated brain atrophy in mild cognitive impairment: a randomized controlled trial. PLoS ONE (VITACOG). — PubMed
- de Jager CA et al. (2012). Cognitive and clinical outcomes of homocysteine-lowering B-vitamin treatment in mild cognitive impairment: a randomized controlled trial. Int J Geriatr Psychiatry. — PubMed
- Jerneren F et al. (2015). Brain atrophy in cognitively impaired elderly: the importance of long-chain omega-3 fatty acids and B vitamin status in a randomized controlled trial. Am J Clin Nutr. — PubMed
- Troen AM et al. (2006). Unmetabolized folic acid in plasma is associated with reduced natural killer cell cytotoxicity among postmenopausal women. J Nutr. — PubMed
- Pietrzik K et al. (2010). Folic acid and L-5-methyltetrahydrofolate: comparison of clinical pharmacokinetics and pharmacodynamics. Clin Pharmacokinet. — PubMed
- Wilson CP et al. (2012). Riboflavin offers a targeted strategy for managing hypertension in patients with the MTHFR 677TT genotype. Am J Clin Nutr. — PubMed
- McNulty H et al. (2017). Effect of continued folic acid supplementation beyond the first trimester of pregnancy on cognitive performance in the child. Am J Clin Nutr. — PubMed
- Bailey SW, Ayling JE (2009). The extremely slow and variable activity of dihydrofolate reductase in human liver and its implications for high folic acid intake. Proc Natl Acad Sci. — PubMed
- Selhub J (2002). Folate, vitamin B12 and vitamin B6 and one carbon metabolism. J Nutr Health Aging. — PubMed
- Scaglione F, Panzavolta G (2014). Folate, folic acid and 5-methyltetrahydrofolate are not the same thing. Xenobiotica. — PubMed
- Crider KS et al. (2011). Folate and DNA methylation: a review of molecular mechanisms and the evidence for folate's role. Adv Nutr. — PubMed
PubMed Topic Searches
- PubMed: MTHFR polymorphism folate
- PubMed: methylation cycle SAMe homocysteine
- PubMed: 5-methyltetrahydrofolate methylfolate
- PubMed: unmetabolized folic acid UMFA
- PubMed: methyl trap B12 folate
- PubMed: cerebral folate deficiency autoantibody
Connections
- Vitamin B9 Overview
- B9 Benefits Hub
- B9 Pregnancy & Neural Tube
- B9 Cardiovascular & Stroke
- B9 Depression & Mental Health
- Vitamin B12 (Methylcobalamin)
- Vitamin B6 (P5P)
- Vitamin B2 (Riboflavin)
- Choline
- Methionine
- Homocysteine
- Anemia (Megaloblastic)
- Depression
- Alzheimer's Disease
- Dementia
- B12 Deficiency Diagnosis
- All Vitamins