Folate for Depression & Mental Health
L-methylfolate is the only folate form formally classified by the FDA as a medical food for adjunctive treatment of major depressive disorder. The 2012 Papakostas trial published in American Journal of Psychiatry established that 15 mg/day L-methylfolate (Deplin) added to SSRI antidepressants approximately doubled treatment response in patients who had failed SSRI monotherapy — an effect size comparable to switching antidepressants. The biochemistry explains why synthetic folic acid does not produce the same response: depression treatment depends on methylation-cycle reset (SAMe synthesis), monoamine production (BH4 regeneration drives tyrosine and tryptophan hydroxylase), and direct cerebrospinal-fluid folate delivery — all of which methylfolate provides directly and synthetic folic acid provides only via the same MTHFR enzyme that depressed patients (disproportionately MTHFR-variant carriers) cannot efficiently use. This page covers the trial evidence, the MTHFR-depression connection, the prescription Deplin protocol, postpartum depression, and the broader role of methylation in psychiatric care.
Table of Contents
- Mechanism: How Folate Supports Mood
- BH4 Regeneration & Monoamine Synthesis
- Observational Evidence: Folate Status & Depression Risk
- MTHFR & Treatment-Resistant Depression
- Coppen & Bailey (2000) Folic Acid + Fluoxetine
- Papakostas (2012) L-Methylfolate + SSRI
- L-Methylfolate (Deplin) FDA Medical Food Status
- Why Synthetic Folic Acid Works Less Well
- Postpartum Depression Connection
- Schizophrenia & Bipolar Disorder
- Cognitive Decline & Dementia
- Practical Protocol
- Cautions
- Key Research Papers
- Connections
- Featured Videos
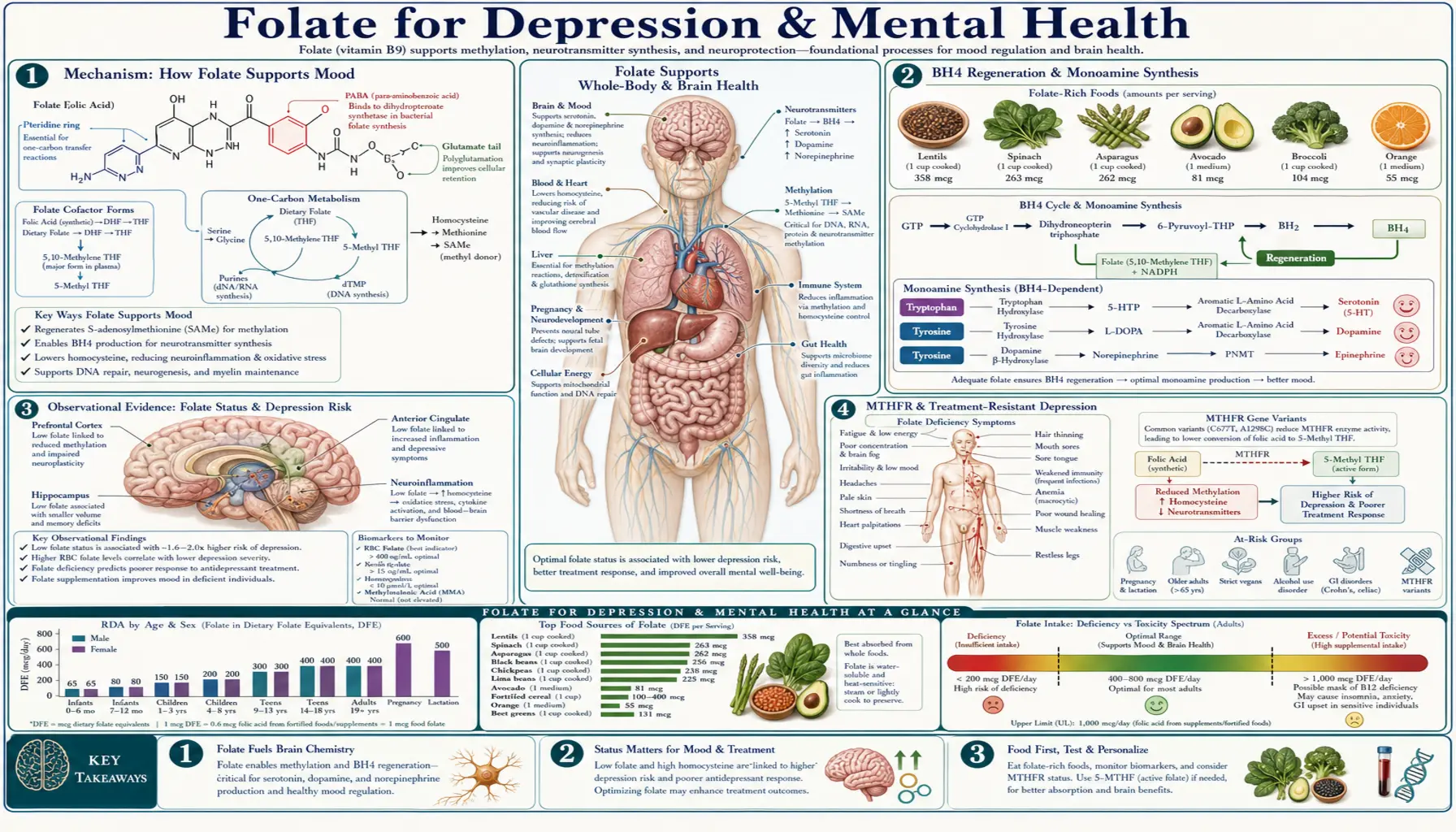
Mechanism: How Folate Supports Mood
Folate's mental-health effects operate through several converging biochemical pathways:
- SAMe (S-adenosylmethionine) synthesis — SAMe is the universal methyl donor produced through the folate-driven methylation cycle. SAMe itself has independent antidepressant activity (multiple RCTs support efficacy roughly comparable to SSRIs, with faster onset). Folate insufficiency limits SAMe production. Methylfolate supplementation increases SAMe by relieving the folate bottleneck.
- BH4 (tetrahydrobiopterin) regeneration — BH4 is the rate-limiting cofactor for tyrosine hydroxylase (producing dopamine) and tryptophan hydroxylase (producing serotonin). 5-MTHF regenerates BH4 from BH2 in a folate-dependent reaction. Insufficient methylfolate → insufficient BH4 → reduced monoamine synthesis → depressed mood.
- Direct cerebrospinal-fluid folate delivery — the brain has a dedicated folate-receptor-mediated transport system. 5-MTHF crosses the blood-brain barrier and concentrates in CSF at levels approximately 4× higher than plasma. Synthetic folic acid does not efficiently cross via this transporter.
- DNA methylation & epigenetic regulation — SAMe-dependent DNA methylation regulates gene expression including stress-response genes. Methylation patterns in the BDNF promoter, glucocorticoid receptor genes, and serotonin transporter genes are all altered in depression and respond to methyl-donor availability.
- Phosphatidylcholine synthesis — folate-dependent methylation produces phosphatidylcholine from phosphatidylethanolamine via the PEMT pathway. Phosphatidylcholine is a major component of myelin and synaptic membranes; insufficient methylation may contribute to white matter abnormalities seen in depression and bipolar disorder.
- Homocysteine clearance — elevated homocysteine is independently associated with depression and cognitive decline, possibly through vascular and neurotoxic mechanisms. Folate-dependent remethylation lowers homocysteine.
The clinical implication: folate insufficiency disrupts at least four independent mechanisms relevant to mood regulation. Treatment-resistant depression in MTHFR-variant carriers represents the convergence of all of them.
BH4 Regeneration & Monoamine Synthesis
Tetrahydrobiopterin (BH4) is the essential cofactor for three rate-limiting monoamine-synthesis enzymes:
- Tyrosine hydroxylase — converts tyrosine to L-DOPA, the precursor to dopamine and norepinephrine
- Tryptophan hydroxylase — converts tryptophan to 5-hydroxytryptophan, the precursor to serotonin
- Phenylalanine hydroxylase — converts phenylalanine to tyrosine
BH4 is converted to BH2 (dihydrobiopterin) during each enzymatic cycle and must be regenerated back to BH4 to continue functioning. The regeneration step requires dihydrofolate reductase (DHFR) and a methyl group donated by 5-MTHF. In folate insufficiency or MTHFR variant carriers with reduced 5-MTHF production, BH4 cannot be efficiently regenerated. The BH2:BH4 ratio rises, monoamine synthesis falls, and depressive symptoms appear or worsen.
The Bottiglieri laboratory (Baylor College of Medicine) has done much of the foundational work showing that depressed patients have reduced CSF 5-MTHF, reduced CSF BH4, reduced CSF monoamine metabolites, and that L-methylfolate supplementation restores all three. This is the biochemical basis for the L-methylfolate-depression connection: 5-MTHF doesn't just lower homocysteine — it directly rescues monoamine synthesis machinery in the brain.
Observational Evidence: Folate Status & Depression Risk
The observational literature consistently links low folate status to depression:
- ~30% of patients hospitalized for major depression have low serum or red blood cell folate — far higher than the prevalence in general medical populations (Coppen & Bolander-Gouaille, 2005 review)
- Low folate is associated with longer depressive episodes, slower SSRI response, higher rates of treatment resistance, and increased relapse risk
- Patients with treatment-resistant depression have lower CSF 5-MTHF concentrations than treatment-responsive depressed patients or controls
- Population studies show 50-80% increased depression risk in the lowest folate-intake quintile compared to the highest
- The Hordaland Homocysteine Study (Norway, ~5,500 subjects) showed elevated homocysteine and low folate both independently associated with depression and anxiety
The relationship is bidirectional — depression reduces appetite and food intake, which lowers folate intake, which worsens the methylation-cycle disruption that contributes to depression. This makes baseline folate status difficult to interpret causally but reinforces the clinical practice of testing and correcting folate insufficiency in any depressed patient.
MTHFR & Treatment-Resistant Depression
MTHFR polymorphisms are significantly enriched in patients with treatment-resistant depression. The data:
- MTHFR C677T TT homozygotes have ~1.4-1.7× increased risk of major depression in meta-analyses
- Among treatment-resistant patients specifically, MTHFR variant prevalence is approximately 70% (vs ~50% in the general population)
- MTHFR-variant patients respond preferentially to L-methylfolate over synthetic folic acid — the Papakostas 2012 trial subgroup analysis showed the strongest effect in TT genotype and obese (high inflammation) patients
- The Stanford group and others have shown MTHFR-variant depressed patients have lower CSF 5-MTHF, higher CSF BH2:BH4 ratio, and lower CSF monoamine metabolites than wild-type depressed patients — a coherent biochemical picture
Clinical implications:
- Treatment-resistant depression patients should be considered for MTHFR genotyping (many integrative psychiatrists test routinely)
- MTHFR variant carriers should receive methylfolate, not synthetic folic acid, as part of their treatment plan
- L-methylfolate trials should be considered before declaring SSRI failure and switching agents — the augmentation strategy may rescue response without changing the underlying antidepressant
Coppen & Bailey (2000) Folic Acid + Fluoxetine
One of the first randomized trials of folate as antidepressant augmentation. Coppen & Bailey randomized 127 patients with major depression to fluoxetine 20 mg + folic acid 500 mcg or fluoxetine 20 mg + placebo for 10 weeks.
Results:
- Significantly greater Hamilton Depression Rating Scale improvement in the folic acid group
- Effect was concentrated in women — female participants showed clear benefit; male participants did not (a finding never satisfactorily explained, possibly reflecting underlying differences in folate status or response)
- Established proof-of-concept for folate as SSRI augmentation
- Used synthetic folic acid (5-MTHF was not widely available at the time); a modest dose by current standards (500 mcg)
The Coppen trial led to a series of folate-augmentation trials with synthetic folic acid producing modestly positive results, but never the dramatic effect that would change clinical practice. The biochemistry — specifically the MTHFR variant problem and BH4 regeneration — would not be fully appreciated until methylfolate became available for clinical use.
Papakostas (2012) L-Methylfolate + SSRI
The pivotal trial. Papakostas et al. (American Journal of Psychiatry 2012) conducted two sequential trials of L-methylfolate as SSRI augmentation in patients with treatment-resistant major depressive disorder.
Trial 1: 7.5 mg L-methylfolate
- 148 patients with MDD who had failed adequate SSRI therapy
- Randomized to L-methylfolate 7.5 mg/day or placebo added to ongoing SSRI
- 30-day treatment period
- Results: no statistically significant difference (the 7.5 mg dose was insufficient)
Trial 2: 15 mg L-methylfolate
- 75 SSRI-resistant patients
- Randomized to L-methylfolate 15 mg/day or placebo added to ongoing SSRI
- 60-day treatment period
- Results:
- HAM-D response rate: 32% with L-methylfolate vs 15% with placebo (P=0.04)
- Mean HAM-D improvement: significantly greater with L-methylfolate
- Effect concentrated in patients with elevated inflammatory markers (CRP, BMI), with MTHFR variants, and with low baseline folate — the biochemically-rational subgroups
- Safety profile excellent — no significant adverse events vs placebo
- Discontinuation rates similar between groups
The Papakostas trial established three things:
- L-methylfolate is an effective SSRI augmentation strategy in treatment-resistant depression
- The dose matters — 7.5 mg was insufficient; 15 mg was effective
- Response is most pronounced in patients with inflammatory or methylation-cycle disruption — the biochemical underpinning matters
Subsequent open-label studies and clinical experience have supported L-methylfolate use at 7.5-15 mg/day as an augmentation option in patients with major depression, particularly those with MTHFR variants, elevated inflammation, or partial SSRI response.
L-Methylfolate (Deplin) FDA Medical Food Status
L-methylfolate is available in the US as Deplin in 7.5 mg and 15 mg prescription capsules, manufactured by Alfasigma. Deplin is classified by the FDA as a "medical food" — a regulatory category that requires prescription dispensing and physician supervision but does not require the full new-drug approval pathway.
The medical food classification:
- Requires that the product is "specially formulated and processed for the partial or exclusive feeding of a patient by means of oral intake or enteral feeding by tube"
- Requires intended for "dietary management of a disease or condition for which distinctive nutritional requirements... have been established by medical evaluation"
- Must be used under physician supervision
- Different regulatory framework than prescription drugs (no Phase III trial requirement) but FDA-recognized therapeutic role
The medical food rationale for L-methylfolate in depression: patients with major depression who have failed standard antidepressant therapy may have functional folate deficiency (especially MTHFR-variant carriers) for whom standard dietary folate or even folic acid supplementation cannot adequately provide active 5-MTHF. L-methylfolate addresses this distinctive nutritional requirement directly.
Practical access:
- Deplin is dispensed by prescription, typically through specialty pharmacies (Cigna, AllianceRx Walgreens Prime, others)
- Insurance coverage is variable — many plans require prior authorization or do not cover
- Out-of-pocket cost: ~$100-200/month at the 15 mg dose
- Over-the-counter L-methylfolate at equivalent doses is available from integrative-medicine brands (Pure Encapsulations, Thorne, Designs for Health, Seeking Health) at substantially lower cost (~$20-50/month for equivalent dosing). Quatrefolic-brand methylfolate is widely used in these products.
- Patients with insurance coverage should use Deplin; patients without coverage can achieve equivalent therapeutic effect with OTC methylfolate at lower cost, with the caveat that they are not in the formally-supervised medical-food framework
Why Synthetic Folic Acid Works Less Well
The clinical observation that has driven the field: depressed patients (especially treatment-resistant ones) respond to L-methylfolate but often not to equivalent doses of synthetic folic acid. The biochemistry:
- MTHFR conversion bottleneck — ~50-70% of treatment-resistant depressed patients carry MTHFR variants that limit their ability to convert synthetic folic acid into active 5-MTHF. Even at high folic acid doses, the active form may not reach therapeutic concentrations.
- Blood-brain barrier transport — the brain's folate receptor preferentially transports 5-MTHF. Synthetic folic acid binds the receptor with high affinity but may not transport efficiently through it. CSF 5-MTHF concentrations rise more reliably with methylfolate than with folic acid supplementation.
- DHFR saturation — therapeutic depression doses of synthetic folic acid (5-15 mg) would massively exceed DHFR conversion capacity, producing very high UMFA accumulation with uncertain consequences.
- BH4 regeneration requirement — the rate-limiting role of folate in BH4 regeneration depends on 5-MTHF specifically; synthetic folic acid does not directly participate.
- Methylation-cycle direct entry — methylfolate enters the methylation cycle immediately, supporting SAMe production; folic acid requires multi-step conversion that depressed patients with reduced one-carbon flux may not perform efficiently.
The clinical implication: do not substitute synthetic folic acid for L-methylfolate in depression treatment. The doses are not equivalent and the clinical response is not equivalent. Patients seeking the Deplin-class effect at lower cost should use OTC methylfolate (Quatrefolic or Metafolin brand), not generic folic acid.
Postpartum Depression Connection
The postpartum period is the highest-risk window in a woman's life for major depression — with ~10-15% of women experiencing postpartum depression and ~50% of those cases representing major depressive episodes. Folate is particularly relevant in this context because:
- Pregnancy dramatically depletes folate stores — the fetus is an obligate folate consumer; maternal folate falls progressively through pregnancy even with supplementation; lactation continues the demand
- Postpartum hormone shifts — the abrupt drop in estrogen and progesterone after delivery interacts with monoamine systems already strained by folate depletion
- MTHFR-variant women are at particularly high risk — the combination of reduced 5-MTHF production at baseline, pregnancy folate depletion, and hormonal shifts creates a perfect storm for monoamine deficiency
- Sleep deprivation further disrupts the methylation cycle through cortisol elevation and circadian disruption
Clinical implications for postpartum care:
- Continue methylfolate (rather than synthetic folic acid) throughout lactation and into the early postpartum year
- Test postpartum folate, B12, ferritin, vitamin D, and thyroid in any woman with postpartum mood symptoms — all are commonly depleted
- L-methylfolate at 7.5-15 mg/day is a reasonable adjunct to standard postpartum depression treatment, particularly in MTHFR-variant women or those with documented folate insufficiency
- Methylcobalamin (B12) co-supplementation is essential — postpartum B12 insufficiency is common, especially in women who restricted meat during pregnancy
Schizophrenia & Bipolar Disorder
The folate-mental-health relationship extends beyond depression to several other psychiatric conditions:
Schizophrenia
- MTHFR C677T TT genotype is associated with increased schizophrenia risk in meta-analyses (OR ~1.4)
- Negative symptoms (avolition, anhedonia, alogia) correlate with low folate status
- Roffman et al. (JAMA Psychiatry 2013) demonstrated that L-methylfolate + B12 adjunctive treatment significantly improved negative symptoms in chronic schizophrenia patients — particularly those with MTHFR or FOLH1 (folate hydrolase) variants
- Deplin has FDA medical food approval for schizophrenia adjunctive treatment as well as depression
Bipolar disorder
- Methylation pathway disruption is increasingly recognized in bipolar pathophysiology
- Lithium itself affects DNA methylation patterns, suggesting overlap with the folate/SAMe system
- Small trials of methylfolate in bipolar depression have shown promise but require larger replication
- Caution: in bipolar patients, high-dose methylfolate (like SAMe) can potentially precipitate hypomania or mania — start low, monitor closely, coordinate with prescribing psychiatrist
Autism spectrum disorder
- Cerebral folate deficiency (folate-receptor autoantibodies) is detected in a subset of children with autism
- Folinic acid (leucovorin) at 50 mcg/kg/day for 12 weeks has shown improvement in language and behavior in autistic children with positive folate-receptor antibodies (Frye 2013 RCT)
- Distinct from methylfolate — folinic acid is required because it crosses the blood-brain barrier via the alternative receptor when the primary folate receptor is blocked
Cognitive Decline & Dementia
The folate-cognition connection bridges psychiatric and neurological territory:
- Low folate status and elevated homocysteine are both independent risk factors for accelerated cognitive decline, brain atrophy, and Alzheimer's disease
- The VITACOG trial (covered in detail on the Methylation chapter) showed 30% reduction in brain atrophy with folate + B12 + B6 supplementation in MCI patients with elevated homocysteine
- The Jerneren 2015 analysis showed the B-vitamin cognitive effect was conditional on adequate omega-3 status — both nutrient systems must be present for the benefit
- Folate-receptor autoantibodies have been detected in a subset of patients with unexplained dementia or developmental regression, suggesting a possible "cerebral folate deficiency dementia" subtype responsive to folinic acid
For the cognitive-protection use case, the protocol overlaps substantially with the cardiovascular/stroke protocol: methylfolate + methylcobalamin + P5P + riboflavin + DHA omega-3, ideally with homocysteine testing to confirm response and titrate dose.
Practical Protocol
For partial SSRI response or treatment-resistant depression
- Test first: Homocysteine, serum/RBC folate, B12 + MMA, vitamin D, thyroid panel, ferritin (rule out other contributors). MTHFR genotype if available.
- L-methylfolate dose: Start 7.5 mg/day for 4 weeks; if partial response or no response, escalate to 15 mg/day for additional 6-8 weeks
- Co-supplementation (essential):
- Methylcobalamin 1,000-5,000 mcg/day — required to prevent methyl trap and B12 deficiency masking
- P5P (B6) 25-50 mg/day — transsulfuration support and additional monoamine cofactor
- Riboflavin 25 mg/day — MTHFR stabilization, especially for variant carriers
- Adjuncts to consider:
- SAMe 400-1,600 mg/day on empty stomach — complementary methylation support; can be used alongside methylfolate
- Omega-3 (EPA-dominant, 1-2 g EPA daily) — independent antidepressant evidence + supports the B-vitamin cognitive effect
- Vitamin D3 2,000-5,000 IU daily (target 25-OH-D 40-60 ng/mL)
- Magnesium glycinate 200-400 mg elemental at bedtime
- Monitoring: Reassess depression severity (PHQ-9 or HAM-D), homocysteine, and any side effects at 4 and 8 weeks
For postpartum depression
- Continue methylfolate 800 mcg - 5 mg/day (titrate based on severity and MTHFR status)
- Methylcobalamin 1,000 mcg daily
- Test ferritin, vitamin D, thyroid — treat any deficiencies
- Continue with prescribed antidepressant therapy if appropriate (most SSRIs are compatible with breastfeeding)
For schizophrenia negative symptoms (Roffman protocol)
- L-methylfolate 15 mg/day + methylcobalamin 1,000 mcg/day as adjunct to ongoing antipsychotic therapy
- Coordinate with treating psychiatrist — do not substitute for antipsychotic
For dosing approach
- Start at the lower end of the dose range to avoid methylation-overdrive side effects (anxiety, agitation, insomnia)
- Some patients with COMT slow variants experience methylation overdrive at standard doses — for these patients, start with 400-800 mcg methylfolate and titrate slowly
- Folinic acid (leucovorin) at 800 mcg to 5 mg is an alternative for patients who tolerate methylfolate poorly — provides folate cycle support without the methyl-donation effect
- Niacin (500 mg) can rescue acute methyl overload by acting as a methyl sink via the NNMT enzyme
Cautions
- B12 deficiency masking — the universal folate caution. High-dose folate (methylfolate or folic acid) corrects megaloblastic anemia from B12 deficiency while allowing irreversible neurological damage to progress unchecked. Always assess B12 status (serum B12, MMA, homocysteine) before initiating high-dose folate. Co-supplement methylcobalamin 1,000+ mcg/day with any high-dose methylfolate regimen. This is the single most important folate safety consideration.
- Bipolar precipitation — high-dose methylfolate (like SAMe) can potentially precipitate mania or hypomania in bipolar patients. Screen carefully for bipolar history before initiating; monitor closely; coordinate with prescribing psychiatrist; start at lower doses (7.5 mg).
- Methylation overdrive symptoms — anxiety, agitation, irritability, insomnia, jitteriness in the first 1-2 weeks of methylfolate. Particularly common in COMT-slow variants. Strategies: reduce dose, switch to folinic acid (does not provide methyl groups directly), rescue with niacin 500 mg or B3 to act as methyl sink, or discontinue if intolerable.
- SSRI/SNRI interactions — no direct pharmacokinetic interactions; methylfolate is a pharmacodynamic adjunct that enhances SSRI/SNRI response without altering blood levels. Safe to combine. Patients should not stop their prescribed antidepressant when starting methylfolate — the strategy is augmentation, not substitution.
- MAOI interactions — methylfolate enhances monoamine synthesis through BH4 regeneration. Theoretical interaction with MAOIs (which inhibit monoamine breakdown). The combination may produce dramatic responses but should be initiated cautiously and only under prescribing psychiatrist supervision.
- Lithium — folate is safe with lithium; no specific interaction. Methylation-pathway disruption is part of bipolar pathophysiology and methylfolate may complement lithium.
- Cerebral folate deficiency requires folinic acid — in patients with documented folate-receptor autoantibodies, methylfolate may not adequately reach the CSF. Folinic acid (leucovorin) is the appropriate folate form via the alternative receptor.
- Pregnancy & breastfeeding — methylfolate is safe and preferred in pregnancy and lactation. Choose 5-MTHF over synthetic folic acid for any therapeutic dosing.
- Hold off in immediate post-MI period — while not specifically a depression concern, high-dose B vitamins in the immediate post-MI period have been associated with adverse signals (NORVIT trial). Wait until cardiac status is stable before initiating high-dose folate-based protocols in patients with recent MI.
Key Research Papers
- Papakostas GI et al. (2012). L-methylfolate as adjunctive therapy for SSRI-resistant major depression: results of two randomized, double-blind, parallel-sequential trials. Am J Psychiatry. — PubMed
- Coppen A, Bailey J (2000). Enhancement of the antidepressant action of fluoxetine by folic acid: a randomised, placebo controlled trial. J Affect Disord. — PubMed
- Fava M, Mischoulon D (2009). Folate in depression: efficacy, safety, differences in formulations, and clinical issues. J Clin Psychiatry. — PubMed
- Coppen A, Bolander-Gouaille C (2005). Treatment of depression: time to consider folic acid and vitamin B12. J Psychopharmacol. — PubMed
- Bottiglieri T (2005). Homocysteine and folate metabolism in depression. Prog Neuropsychopharmacol Biol Psychiatry. — PubMed
- Gilbody S et al. (2007). Methylenetetrahydrofolate reductase (MTHFR) genetic polymorphisms and psychiatric disorders: a HuGE review. Am J Epidemiol. — PubMed
- Roffman JL et al. (2013). Randomized multicenter investigation of folate plus vitamin B12 supplementation in schizophrenia. JAMA Psychiatry. — PubMed
- Frye RE et al. (2013). Folinic acid improves verbal communication in children with autism and language impairment: a randomized double-blind placebo-controlled trial. Mol Psychiatry. — PubMed
- Bottiglieri T (1996). Folate, vitamin B12, and neuropsychiatric disorders. Nutr Rev. — PubMed
- Stahl SM (2007). L-methylfolate: a vitamin for your monoamines. J Clin Psychiatry. — PubMed
- Lewis SJ et al. (2006). The thermolabile variant of MTHFR is associated with depression in the British Women's Heart and Health Study. Mol Psychiatry. — PubMed
- Lazarou C, Kapsou M (2010). The role of folic acid in prevention and treatment of depression: an overview of existing evidence. Complement Ther Clin Pract. — PubMed
- Lewis SJ et al. (2012). The thermolabile variant of MTHFR is associated with depression in the British Women's Heart and Health Study and a meta-analysis. Mol Psychiatry. — PubMed
PubMed Topic Searches
- PubMed: L-methylfolate depression
- PubMed: MTHFR treatment-resistant depression
- PubMed: folate SSRI augmentation
- PubMed: postpartum depression folate B12
- PubMed: BH4 folate monoamine
- PubMed: SAMe depression
- PubMed: folinic acid cerebral folate deficiency autism
Connections
- Vitamin B9 Overview
- B9 Benefits Hub
- B9 Pregnancy & Neural Tube
- B9 Methylation & Homocysteine
- B9 Cardiovascular & Stroke
- Folate and Mental Health
- Vitamin B12 (Methylcobalamin)
- Vitamin B6 (P5P)
- Vitamin B2 (Riboflavin)
- Vitamin D
- Methionine
- Tryptophan
- Tyrosine
- Homocysteine
- Depression
- Anxiety
- Alzheimer's Disease
- Dementia
- All Vitamins